
Research Article | DOI: https://doi.org/10.31579/2690-8794/112
1 Eskisehir Acibadem Hospital, Obstetrics and Gynecology Clinic, Eskisehir, Turkey.
2 Department of Obstetrics and Gynecology, Eskisehir Osmangazi University School of Medicine, Eskisehir Turkey.
*Corresponding Author: Ceren Yildiz Eren, Eskisehir Acibadem Hospital, Obstetrics and Gynecology Clinic, Eskisehir, Turkey.
Citation: Ceren Yildiz Eren, Ozlem Ozgur Gursoy, Hulusi Goktug Gurer, Turgay ŞENER (2022) Does A New Fascial Closure Technique during Cesarean Section have an Impact on the Postoperative Corner Pain and Patient Satisfaction?, J, Clinical Medical Reviews and Reports. 4(2); DOI: 10.31579/2690-8794/112
Copyright: © 2022, Ceren Yildiz Eren, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 November 2021 | Accepted: 18 December 2021 | Published: 06 January 2022
Keywords: fascial closure; cesarean section; corner pain
Cesarean section is one of the most common operations worldwide. For this reason, techniques related to cesarean delivery have extremely important. In this study, it was aimed to evaluate postoperative pain and patient satisfaction following a new fascia closure technique.
This study was designed as a prospective randomized controlled trial. In this context, a total of 51 women who were planned for lower segment cesarean section with Pfannenstiel incision were randomly divided into two groups. In our new technique, the corner nodes were embedded under the fascia layer on the muscle layer. The main outcome measures used in the assessment were postoperative corner pain not requiring analgesic supplementation and patient satisfaction. Postoperative pain was evaluated with the verbal rating scale and patient satisfaction with the verbal rating satisfaction scale. Preparative and postoperative hemoglobin estimation, blood loss, and length of hospital stay were used as secondary outcome measures.
There was no statistically significant difference between the two groups in terms of estimated blood loss, pre- and post-procedure hemoglobin values, and length of hospital stay (p>0.05). Similarly, no statistically significant difference was found in terms of the results of the early postoperative verbal rating scale and the patient satisfaction scale. A rating scale was applied to the participants in the sixth week postpartum. According to the results, corner pain and patient satisfaction scores in the group in which the new technique was applied were found to be more satisfactory than the traditional technique. This difference is also statistically significant.
Examination of our technique in large samples with multicenter planned studies will benefit its development. It is thought that after this stage, it can enter into widespread use.
Cesarean section is an operation that involves an open incision in the abdomen and an incision made on the uterus for the purpose of delivery. One of the most common operations worldwide is cesarean section, with more than one million per year in the USA alone. For this reason, techniques related to cesarean delivery have extremely important effects in the lives of women and their families. In cesarean deliveries, the surgeon must pass through all the layers surrounding the fetus to reach the fetus. First, the skin is opened, followed by the subcutaneous tissues. The next layer is the fascia of the rectus abdominis muscles. Following the separation of the rectus muscles, the abdominal cavity is entered. In pregnant women, the uterus is often encountered as soon as it enters the abdomen [1].
Cesarean section is an operation that includes many techniques. Various techniques are used at each stage or tissue layer during the operation. Many factors affect the operator's decisions regarding the technique to be used. Decisions on cesarean section techniques, no different from any medical field, should also be evidence-based [2].
It is essential that all surgeries to be performed on the human body are performed with the least damage to the tissue. Respect for tissue is extremely important at all stages of surgery. The most common incision today is the Pfannenstiel incision. Post-operative complications are often pain and infection [3].
The incidence of cesarean delivery has increased significantly in recent years. Although it is considered a safe operation, possible complications are important. In all cases where cesarean delivery is indicated, the appropriate technique should be selected, and surgical principles should be followed. It is necessary to enhance current cesarean section techniques and to conduct continuous research [4].
In this study, it was aimed to evaluate postoperative pain and patient satisfaction following a new fascia closure technique.
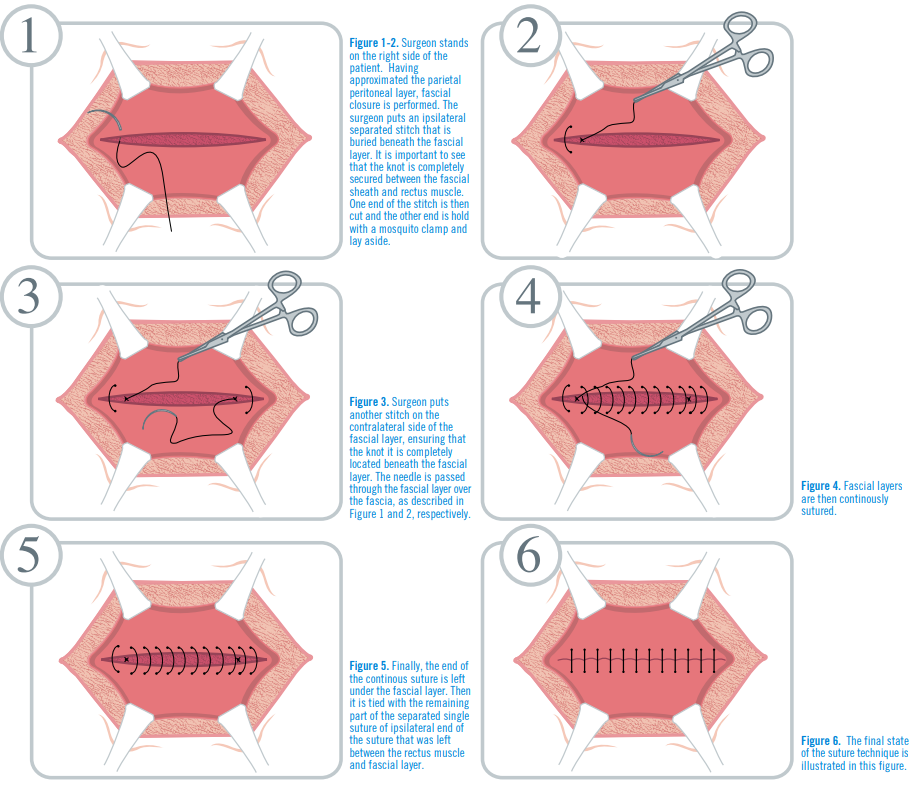
This study was designed as a prospective randomized controlled trial. In this context, a total of 51 women who were planned for lower segment cesarean section with Pfannenstiel incision were randomly divided into two groups. While a new technique was used to close the fascia in one of the groups (group I, n:26), the classical closure technique was used in the other (group II, n:25). In the traditional technique, both corner nodes remained below the subcutaneous layer, above the fascia. In our new technique, the corner nodes were embedded under the fascia layer on the muscle layer (Figure 1-6).
The main outcome measures used in the assessment were postoperative corner pain not requiring analgesic supplementation and patient satisfaction. Postoperative pain was evaluated with the verbal rating scale and patient satisfaction with the verbal rating satisfaction scale. Preparative and postoperative hemoglobin estimation, blood loss, and length of hospital stay were used as secondary outcome measures.
There was no statistically significant difference between the two groups in terms of estimated blood loss, pre- and post-procedure hemoglobin values, and length of hospital stay (p>0.05). Similarly, no statistically significant difference was found in terms of the results of the early postoperative verbal rating scale, which evaluates postoperative corner pain, and the patient satisfaction scale, which examines patient satisfaction. A rating scale was applied to the participants in the sixth week postpartum. According to the results, corner pain and patient satisfaction scores in the group in which the new technique was applied were found to be more satisfactory than the traditional technique. This difference is also statistically significant (p<0>
Today, cesarean section is one of the most frequently performed operations. Although considered simple compared to other operations, possible complications can have devastating consequences for both mother and fetus. It is very important for specialist physicians to be informed about new developments and various modifications in standard cesarean section techniques to minimize morbidity and mortality [5].
The risk of developing an infection after cesarean section is higher in women who gave birth by cesarean section by up to 20 times compared to those who gave birth normally. In addition to infection, wound complications such as hematoma, seroma, and separation can also be seen after cesarean section. Complications may cause adverse effects on maternal health, the mother's ability to care for her baby, and birth experience in the postpartum period [6, 7].
In cesarean section operations, closure of the fascia is an important step since it is largely responsible for the durability of the skin in the postoperative period [8].
Postoperative pain that develops after cesarean section affects daily activities and contributes to the development of permanent pain. This pain has also been reported to affect their ability to care for the infant, effective breastfeeding, and quality interaction with infants. The factors affecting the perception of pain in the postoperative period have not been examined in detail. In a study, the incidence of moderate-to-severe postoperative pain was found to be approximately 80% [9].
Pain after cesarean section has not been adequately studied. To examine this issue, a prospective study was planned and the incidence of chronic pain at 3, 6, and 12 months after cesarean section was examined. Accordingly, the incidence of chronic pain at the 3rd, 6th, and 12th months after cesarean section was calculated to be 18.3%, 11.3%, and 6.8%, respectively [10].
In one study, 111 women who gave birth by cesarean section were prospectively examined. In women who were operated with the Pfannenstiel cesarean section method, the duration of delivery and surgery was found to be significantly longer. Complaints of incision pain and need for analgesic injections were also found to be significantly higher in women on the second postpartum day [11].
A study was conducted to investigate the prevalence of post-Pfannenstiel pain complaints. A questionnaire assessing pain in the Pfannenstiel area was administered to all women who had a Pfannenstiel incision for cesarean delivery or abdominal hysterectomy. After a two-year follow-up, approximately 35% of the participants experienced chronic pain in the incision area [12].
Pain complications arise in cesarean section operations, especially after Pfannenstiel's incision. It is also common for this condition to turn into chronic pain. In addition, the comfort of life of the mother and baby decreases due to the pain experienced. With the new fascia closure technique examined in our study, the sutures are left under the fascia during closure, thus reducing postoperative corner pains and indirectly increasing patient satisfaction and the life comfort of mother and baby. Examination of our technique in large samples with multicenter planned studies will benefit its development. It is thought that after this stage, it can enter into widespread use.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
