
Research Article | DOI: https://doi.org/10.31579/2690-8808/123
Radionuclide Diagnostics Department, Medical Radiological Research Centre, Russia
*Corresponding Author: Vladimir Zaichick, Radionuclide Diagnostics Department, Medical Radiological Research Centre, Russia
Citation: Vladimir Zaichick. (2022) Distinguish Thyroid Malignant from Benign Alterations using Neutron Activation Analysis of Chemical Element Contents in Nodular Tissue; Journal of Clinical Case Reports and Studies; 3(5); DOI: 10.31579/2690-8808/123
Copyright: © 2022 Vladimir Zaichick, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 April 2022 | Accepted: 10 May 2022 | Published: 06 June 2022
Keywords: thyroid; thyroid malignant and benign nodules; chemical elements; neutron activation analysis
Thyroid benign (TBN) and malignant (TMN) nodules are a common thyroid lesion. The differentiation of TMN often remains a clinical challenge and further improvements of TMN diagnostic accuracy are warranted. The aim of present study was to evaluate possibilities of using differences in chemical elements (ChEs) contents in nodular tissue for diagnosis of thyroid malignancy. Contents of eight ChEs including bromine (Br), calcium (Ca), chlorine (Cl), iodine (I), potassium (K), magnesium (Mg), manganese (Mn), and sodium (Na) were prospectively evaluated in nodular tissue of thyroids with TBN (79 patients) and to TMN (41 patients). Measurements were performed using instrumental neutron activation analysis. It was observed that in TMN tissue the mass fractions of Br and I are approximately 2.9 and 14 times, respectively, lower, while the mass fraction of Ca, K, and Mg are 94%, 56%, and 36%, respectively, higher than in TBN tissue. Contents of Cl, Mn, and Na found in the TBN and TMN groups of nodular tissue samples were similar. Finally, it was proposed to use the I mass fraction and I/Ca, I/K, and I/Mg mass fraction ratios in a needle-biopsy of thyroid nodules as a potential tool to diagnose thyroid malignancy. Further studies on larger number of samples are required to confirm our findings and proposals.
Nodules are a common thyroid lesion, particularly in women. Depending on the method of examination and general population, thyroid nodules (TNs) have an incidence of 19–68% [1]. In clinical practice, TNs are classified into benign (TBN) and malignant (TMN), and among all TNs approximately 10% are TMN [2]. It is appropriate mention here that the incidence of TMN is increasing rapidly (about 5
All patients suffered from TBN (n=79, mean age M±SD was 44±11 years, range 22-64) and from TMN (n=41, mean age M±SD was 46±15 years, range 16-75) were hospitalized in the Head and Neck Department of the Medical Radiological Research Centre (MRRC), Obninsk. Thick-needle puncture biopsy of suspicious nodules of the thyroid was performed for every patient, to permit morphological study of thyroid tissue at these sites and to estimate their ChEs contents. In all cases the diagnosis has been confirmed by clinical and morphological results obtained during studies of biopsy and resected materials. Histological conclusions for TBN were: 46 colloid goiter, 19 thyroid adenoma, 8 Hashimoto's thyroiditis, and 6 Riedel’s Struma, whereas for TMN were: 25 papillary adenocarcinomas, 8 follicular adenocarcinomas, 7 solid carcinomas, and 1 reticulosarcoma. Samples of nodular tissue for INAA-SLR were taken from both biopsy and resected materials.
All studies were approved by the Ethical Committees of MRRC. All the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments, or with comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
All tissue samples obtained from TBN and TMN were divided into two portions using a titanium scalpel to prevent contamination by ChEs of stainless steel [49]. One was used for morphological study while the other was intended for ChEs analysis. After the samples for ChEs analysis were weighed, they were freeze-dried and homogenized [50]. The pounded samples weighing about 10 mg (for biopsy) and 100 mg (for resected materials) were used for ChEs measurement by INAA-SLR.
To determine contents of the ChE by comparison with a known standard, biological synthetic standards (BSS) prepared from phenol-formaldehyde resins were used [51]. In addition to BSS, aliquots of commercial, chemically pure compounds were also used as standards. Ten sub-samples of certified reference material (CRM) of the International Atomic Energy Agency (IAEA) IAEA H-4 (animal muscle) weighing about 100 mg were treated and analyzed in the same conditions as thyroid samples to estimate the precision and accuracy of results.
The content of Br, Ca, Cl, I, K, Mg, Mn, and Na were determined by INAA-SLR using a horizontal channel equipped with the pneumatic rabbit system of the WWR-c research nuclear reactor (Branch of Karpov Institute, Obninsk). Details of used nuclear reactions, radionuclides, gamma-energies, spectrometric unit, sample preparation, and the quality control of results were presented in our earlier publications concerning the INAA-SLR of ChEs contents in human thyroid [27,28], scalp hair [52], and prostate [53,54].
A dedicated computer program for INAA-SLR mode optimization was used [55]. All thyroid samples for ChEs analysis were prepared in duplicate, and mean values of ChEs contents were used in final calculation. Using Microsoft Office Excel software, a summary of the statistics, including, arithmetic mean, standard deviation, standard error of mean, minimum and maximum values, median, percentiles with 0.025 and 0.975 levels was calculated for ChEs contents in two groups of nodular tissue (TBN and TMN). The difference in the results between two groups of samples was evaluated by the parametric Student’s t-test and non-parametric Wilcoxon-Mann-Whitney U-test.
Table 1 depicts certain statistical parameters (arithmetic mean, standard deviation, standard error of mean, minimal and maximal values, median, percentiles with 0.025 and 0.975 levels) of the Br, Ca, Cl, I, K, Mg, Mn, and Na mass fraction in thyroid intact tissue samples of two groups of samples - TBN and TMN.
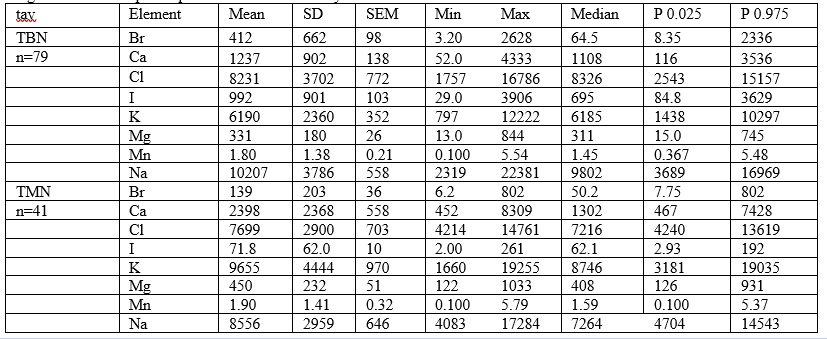
M – arithmetic mean, SD – standard deviation, SEM – standard error of mean, Min – minimum value, Max – maximum value, P 0.025 – percentile with 0.025 level, P 0.975 – percentile with 0.975 level.
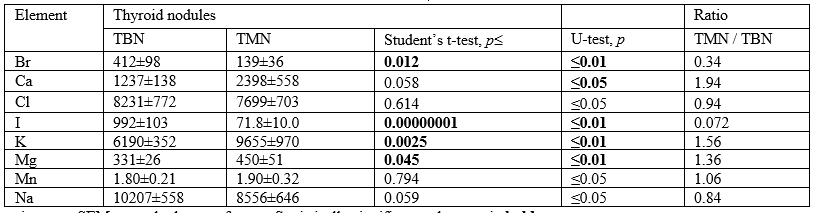
The ratios of means and the comparison of mean values of Br, Ca, Cl, I, K, Mg, Mn, and Na mass fractions in pair of sample groups such as TBN and TMN is presented in Table 2.
The comparison of our results with published data for Br, Ca, Cl, I, K, Mg, Mn, and Na mass fraction in TBN [56-65] and TMN [56,59,62,66-70] is shown in Table 3. A number of values for ChEs mass fractions were not expressed on a dry mass basis by the authors of the cited references. However, we calculated these values using published data for water (75%) [71] and ash (4.16% on dry mass basis) [72] contents in thyroid of adults.
As was shown before [27,28,52-54] good agreement of the Br, Ca, Cl, I, K, Mg, Mn, and Na contents in CRM IAEA H-4 samples analyzed by INAA-SLR with the certified data of this CRM indicates acceptable accuracy of the results obtained in the study of TBN and TMN groups of tissue samples presented in Tables 1-3.
From Table 2, it is observed that in TMN tissue the mass fractions of Br and I are approximately 2.9 and 14 times, respectively, lower, while the mass fraction of Ca, K, and Mg are 94%, 56%, and 36%, respectively, higher than in TBN tissue. In a general sense Cl, Mn, and Na, contents found in the TBN and TMN groups of tissue samples were similar (Table 2).
Mean values obtained for Br, Ca, I, and Mn contents in TBN (Table 3) agree well with median of mean values reported by other researches [56-58,60,61,64]. Mean mass fractions of Cl and Na in TBN obtained in present study were almost one order of magnitude and 3 times higher those in only published article on Cl [59] and Na [65]. Mean mass fraction of K in TBN obtained in present study was a little higher the upper value of range of published means [58], while mass fraction of Mg was a little lower the lowest value of range of published means [62].
Mean values obtained for Ca, I, Mg, and Mn contents in TMN (Table 3)
agree well with median of mean values reported by other researches [56,59,62,66,68-70]. Mean mass fraction obtained for Br in TMN was almost one order of magnitude higher median of previously reported means but inside the range of means [66,67]. Mean mass fraction of K founded in TMN was a little higher the upper value of range of published means {56], while mean mass fraction of Cl was almost one order of magnitude higher that in only published article on this ChEs content in malignant thyroid [59]. No published data referring Na contents of TMN were found (Table 3).
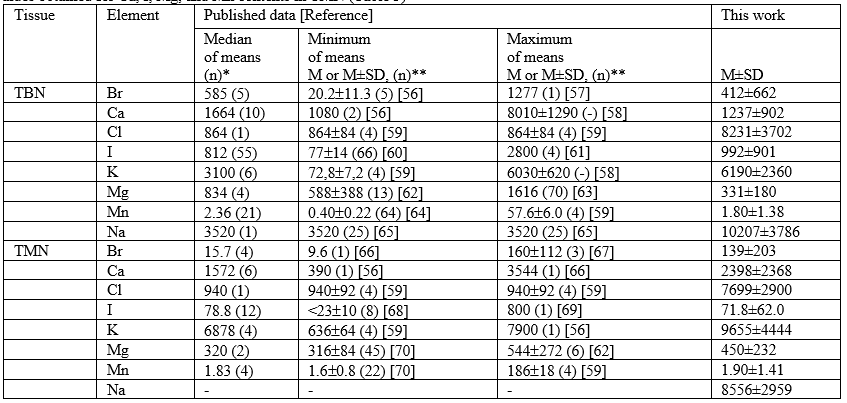
M –arithmetic mean, SD – standard deviation, (n)* – number of all references, (n)** – number of samples
The range of means of Br, Ca, Cl, I, K, Mg, Mn, and Na level reported in the literature for TBN and TMN vary widely (Table 3). This can be explained by a dependence of ChEs content on many factors, including age, gender, ethnicity, mass of the TNs, and the stage of diseases. Not all these factors were strictly controlled in cited studies. However, in our opinion, the leading causes of inter-observer variability can be attributed to the accuracy of the analytical techniques, sample preparation methods, and inability of taking uniform samples from the affected tissues. It was insufficient quality control of results in these studies. In many scientific reports, tissue samples were ashed or dried at high temperature for many hours. In other cases, thyroid samples were treated with solvents (distilled water, ethanol, formalin etc). There is evidence that during ashing, drying and digestion at high temperature some quantities of certain ChEs are lost as a result of this treatment. That concerns not only such volatile halogen as Br, but also other ChEs investigated in the study [73-75]. On the other hand, when destructive analytical techniques are used, the tissue samples may be contaminated by ChEs contained in chemicals using for digestion.
Elemental analysis of affected thyroid tissue could become a powerful diagnostic tool. To a large extent, the resumption of the search for new methods for early diagnosis of TMN was due to experience gained in a critical assessment of the limited capacity of the US-examination [2,3]. In addition to the US test and morphological study of needle-biopsy of the TNs, the development of other highly precise testing methods seems to be very useful. Experimental conditions of the present study were approximated to the hospital conditions as closely as possible. In all cases we analyzed a part of the material obtained from a puncture biopsy of the TNs. Therefore, our data allow us to evaluate adequately the importance of ChEs content information for distinguish TMN from TBN.
Tissue content of Br, Ca, I, K, Mg, are different in most TMN as compared to TBN (Tables 2). It should be noted, however, that Br compounds, especially potassium bromide (KBr), sodium bromide (NaBr), and ammonium bromide (NH4Br), are a component of many tranquilizers and frequently used as sedatives, for example, in Russia [76]. Uncontrolled use of tranquilizers may be the reason for elevated levels of Br in specimens of patients with TNs. Therefore, for diagnostic purposes, data for Br content should be used with caution. Level of I in nodular tissue has very promising prospects as a biomarker of malignancy, because there is a great difference between content of this ChE in TBN and TMN (Tables 2). It is very interest a potential possibilities of using the I/Ca, I/K, and I/Mg ratios as cancer biomarker, because during the thyroid malignant transformation contents of these ChEs in nodular tissue change in different directions – a drastically decrease of I and an increase of Ca, K, and Mg (Tables 2). Thus, the results of study show that nondestructive INAA-SLR analysis if ChEs contents in biopsy of TNs may serve as a potential tool for accurate detection of TMN. Because measurements using INAA-SLR are fast (a few minutes) and they do not need in any samples treatment, this analytical method can be used before morphological examination of biopsy samples.
This study has several limitations. Firstly, analytical technique employed in this study measure only eight ChEs (Br, Ca, Cl, I, K, Mg, Mn, and Na) mass fractions. Future studies should be directed toward using other analytical methods which will extend the list of ChEs investigated in TBN and TMN. Secondly, the sample size of TBN and TMN group was relatively small and prevented investigations of TEs contents in this group using differentials like gender, functional activity of nodules, stage of disease, and dietary habits of patients with TNs. Lastly, generalization of our results may be limited to Russian population. Despite these limitations, this study provides evidence on significant ChEs level alteration in thyroid nodular tissue and shows the necessity to continue ChEs research as potential biomarkers of thyroid malignant transformation.
In this work, elemental analysis was carried out in the nodular tissue samples of thyroid with TBN and TMN using INAA-SLR. It was shown that INAA-SLR is an adequate analytical tool for the non-destructive determination of Br, Ca, Cl, I, K, Mg, Mn, and Na content in the tissue samples of human thyroid, including needle-biopsy material. It was observed that in TMN tissue the mass fractions of Br and I are approximately 2.9 and 14 times, respectively, lower, while the mass fraction of Ca, K, and Mg are 94%, 56%, and 36%, respectively, higher than in TBN tissue. Contents of Cl, Mn, and Na found in the TBN and TMN groups of nodular tissue samples were similar. In our opinion, the drastically decrease in level I and abnormal increase in level Ca, K, and Mg in thyroid nodular tissue could be a specific consequence of malignant transformation. It was proposed to use the I mass fraction and I/Ca, I/K, and I/Mg mass fraction ratios in a needle-biopsy of thyroid nodules as a potential tool to diagnose thyroid malignancy. Further studies on larger number of samples are required to confirm our findings and proposals.
The author is extremely grateful to Profs. B.M. Vtyurin and V.S. Medvedev, MRRC, Obninsk, as well as to Dr. Yu. Choporov, former Head of the Forensic Medicine Department of City Hospital, Obninsk, for supplying thyroid samples.
Distinguish between Thyroid Malignant and Benign Nodules
There were no any sources of funding that have supported this work.
The author has not declared any conflict of interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
