
Case-Report | DOI: https://doi.org/10.31579/2578-8868/088
1 Juha Hernesniemi International Neurosurgery Center, People's Hospital of Zhengzhou University (Henan Provincial People’s Hospital), Henan University, Zhengzhou, 450003, China.
2 Faculty of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
3 Department of Radiology, People's Hospital of Zhengzhou University (Henan Provincial People’s Hospital), 7 Weiwu Road, Zhengzhou, Henan, 450003, China.
*Corresponding Author: Qinghua Liang, Juha Hernesniemi International Neurosurgery Center Henan Provincial Peopl´s Hospital, Henan University Zhengzhou, 450003, China.
Citation: Hernesniemi J., Zemmar A., Malhotra R.K., Haiyang L., Shenglong L., Yazhou X., Qiang L. et al. (2019) Distinct Neuro-Recovery Pattern in Calcified Subdural Hematoma with False-Localizing Sign: A Case Report. J. Neuroscience and Neurological Surgery. 4(5); DOI: 10.31579/2578-8868/088
Copyright: © 2019 Juha Hernesniemi, Ajmal Zemmar. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 August 2019 | Accepted: 09 September 2019 | Published: 23 September 2019
Keywords: false-localizing sign;distinct neuro-recovery
Background: Chronic subdural hematoma is a frequently encountered clinical entity in neurosurgical practice. A small subgroup of chronic subdural hematomas present with calcification or ossification. This entity can pose different operative challenges and distinct clinical features.
Case Description: We describe a 39-year-old male with adult-onset epilepsy presenting with gradual development of headaches and dizziness with right-sided weakness and hyperreflexia. He was found to have a large, right-sided calcified chronic subdural hematoma and underwent craniotomy for evacuation. Postoperatively, the patient had full-strength on the right side but was plegic on the left side, which gradually improved back to normal strength.
Conclusion: We present the case of an adult patient with false-localizing sign and distinct motor recovery pattern attributable to a large calcified chronic subdural hematoma which required delicate resection due to cortical adherence.
Chronic subdural hematomas (CSDH) are a frequently encountered neurosurgical pathology. By comparison, calcification and ossification of CSDH are rare phenomena occurring in approximately 0.3-2.7% of cases.[1] Though approximately 100 cases have been reported in the literature, the exact etiology remains unclear. Calcification and ossification has been observed in post-traumatic subdural hematomas, post-infectious subdural collections and in patients undergoing ventriculoperitoneal (VP) shunting for hydrocephalus.[5] The operative management of calcified CSDHs may be complicated by adherence of the internal subdural membrane to the brain cortex posing challenges for resection.[6] Yet, delicate resection is critical to preserve the plasticity required for motor recovery. Here, we report a case of a large calcified CSDH with Kernohan-Woltman phenomenon.
Case Report
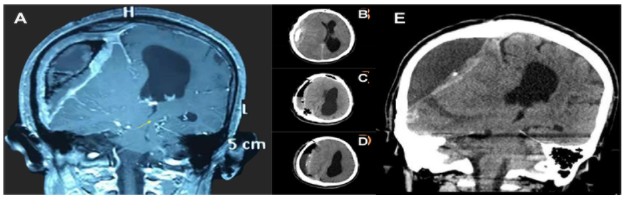
A 39-year-old, right handed male presented with insidious onset of dizziness and headaches for six months. The patient had a 6-year history of epilepsy of unknown etiology and was managed on phenytoin. His seizure frequency had culminated up to 5 seizures daily. An electroencephalogram (EEG) demonstrated epileptiform discharges originating from the right cerebral hemisphere, computed tomography (CT) was significant for a large right-sided calcified pan-hemispheric chronic subdural collection resulting in 4/5 motor power in the right upper (UE) and lower extremities (LE) and right-sided hyperreflexia. (Fig. 1A).
Figures & Figure Legends
Figure 1: A: Pre-operative coronal CT scan demonstrating a large, right sided chronic calcified subdural hematoma with significant mass effect resulting in impingement of the contralateralFigure 1: A: Pre-operative coronal CT scan demonstrating a large, right sided chronic calcified descending motor fibers against the tentorium cerebelli (yellow arrow). B-D: Axial CT scans immediately after evacuation (B), at 2 weeks (C) and 4 weeks (D) post-evacuation. E: Coronal image 2-months after evacuation, note the relationship between descending motor fibers and left tentorium cerebelli despite presence of midline-shift.
A right-sided craniotomy was performed, the inner CSDH membrane was adherent to the cortical surface. A small incision was made into the margin of the internal layer, which was delicately dissected from the cortical surface below. The central membranous portion was tightly adherent to the cortex and left in situ to avoid cortical damage. Strikingly, on postoperative exam, the patient had full-strength (5/5) in both right extremities but was now plegic on the left UE and LE (0/5). CT showed no acute hemorrhague, a chronic subdural collection and midline shift (Fig. 1B), which improved at discharge (Fig. 1C) correlating with significantly enhanced motor strength in left LE & UE (4+/5). Midline-shift regressed at 1-month (Fig. 1D) and 2-month follow-up, at which motor strength was back to normal (5/5) and seizure frequency had decreased back to baseline with normal phenytoin blood levels.
Discussion
We present the case of a large, calcified CSDH producing Kernohan’s phenomenon. After a tightly adherent membrane was delicately separated and left in situ to protect the cortex, a distinct neuroplasticity pattern was observed postoperatively: Ipsilateral hemiparesis recovered rapidly whereas contralateral hemiplegia developed. A likely explanation is a shift in mechanical compression: Once the descending fibers were released at the contralateral tentorium, the fibers recovered resulting in postoperative functional recovery on the ipsilateral side. This was likely paralleled by compression of significant fibers attributable to contralateral motor function, which recovered over time leading to full bilateral recovery at 2-month follow-up. These dynamics identify the remarkable ability of the central nervous system to promote plasticity and functional recovery within a fast-temporal scale. This is a rare presentation of a large calcified CSDH with this distinct pattern of neuroplasticity.
A critical aspect was the extent of resection of the subdural membrane. Li et al. reviewed treatment strategies and outcomes among patients with calcified/ossified CSDH.[3] They identified 21 patients, 18 of whom underwent neurosurgical intervention. Total removal of the subdural hematoma was possible in 8 of 16 patients undergoing craniotomy. Dissection of the inner subdural membrane was identified as the critical operative step. Others reported thinning of the membrane using a high-speed drill, [4] cutting the inner membrane in a grid-like fashion to resolve tension of adherent membrane on the cortex [6] or tenting the inner subdural membrane to the dura. [2] In our case, despite rigorous attempt, en-bloc resection was not possible. Thus, the tightly adherent central visceral membranous attachment was left in situ to achieve maximal-safe resection of subdural membrane and maximally protect the cortex.
Conclusion
We present an adult patient with right-sided calcified subdural hematoma and a distinct motor recovery profile: Although ipsilateral hemiplegia resolved completely post-operatively, the patient developed contralateral hemiplegia, which improved back to normal function. The authors opted for maximal-safe resection of the tightly adherent hematoma membrane, which led to favorable neurological outcome.
Sources of Funding: This work was supported by grants from the Henan Provincial People’s Hospital Outstanding Talents Founding Grant Project, the Heidi Demetriades Foundation and the ETH Foundation (HE-327) to AZ.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
