
Case Report | DOI: https://doi.org/10.31579/2768-2757/047
Department Of Orthopaedics, Holy Spirit Hospital, Andheri, Mumbai.
*Corresponding Author: Clevio Desouza, Department of Orthopaedics, Holy Spirit Hospital, Andheri, Mumbai.
Citation: C Desouza, M Langaliya, P Banka, J Pestonji. (2022). Distal Ulna Giant Cell Tumor: A Case Report. Journal of Clinical Surgery and Research, 3(4); DOI:10.31579/2768-2757/047
Copyright: © 2022, Clevio Desouza. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 March 2022 | Accepted: 01 April 2022 | Published: 27 April 2022
Keywords: giant cell tumor; intralesional curettage; bone grafting
Introduction:Long bone giant cell tumors have been documented in the literature in a large number of cases. A patient with a large giant cell tumor in the distal ulna is described. With a reported prevalence of 0.5 to 6%, this is extremely rare.
Case Presentation:A 16-year-old male presented to the orthopedic OPD with pain and swelling in the wrist. A diagnosis of distal ulna giant cell tumor was made after a histological examination. Intralesional curettage, phenol treatment, and bone grafting were used to treat the malignancy.
Conclusion:If a giant cell tumor is detected early and treated aggressively, it has an excellent prognosis. It is critical to be aware of unusual cancer localizations in order to make an accurate diagnosis.
GCT or Giant cell tumor of the bone is a benign, rare, and locally aggressive tumor. It accounts for about 3 percent to 5 percent of all primary bone malignancies. Adults between the ages of 20 and 40 are most affected. Giant cell tumor of the bone is exceedingly uncommon in children and people over the age of 65. Giant cell tumors affect about one person in a million people each year. The tumor is usually found in the long bone meta-epiphyseal region, particularly in the distal radius and femur, as well as the proximal humerus and tibia. The ulna distal extremity is an uncommon location for a primary bone Giant cell tumor with its occurrence being around 0.45 percent to 3.2 percent. We present the case of a 16-year-old male who was diagnosed with a distal ulna Giant cell tumor. Intralesional curettage and adjuvant therapy in the form of 5 percent phenol with a bone graft reconstruction were used to treat it.
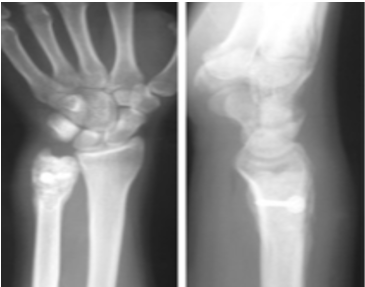
A 16-year-old male came to the Outpatient department with pain and swelling in the left wrist since 3 days. He gave a history of fall while playing football 3 days back. On Examination, there was presence of swelling on the dorsal ulnar aspect of the wrist of size 2.5 cm. Range of movements of the wrist was assessed and was found to be 70 degrees of flexion, 45 degrees of extension, 15 degrees of radial deviation and 10 degrees of ulnar deviation. Circumduction, pronation, and supination were restricted and painful. Radiograph of the left wrist was taken. There was no evidence of fracture on the radiograph, however an osteolytic lesion inducing an expansion was seen in the meta-epiphyseal region of the ulna [Figure 1]. A Magnetic resonance imaging examination was performed. It showed in the T1 sequence presence of a hypointense signal and in the short T1 inversion recovery (STIR) sequences a hyperintense signal was seen which showed enhancement after contrast administration [Figure 2].

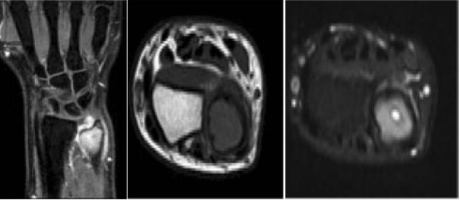
Figure 2: MRI of the Left Wrist showing hypointense signal in the T1 sequences and a hyperintense signal in the short TI inversion recovery (STIR) sequences.
A biopsy was planned, and the sample was sent for histopathology where a diagnosis of Giant cell tumor was made. This was an atypical site for a Giant cell tumor. The lesion was classified as a grade II with fracture [Figure 1], according to the Campanacci Classification and as a stage II according to the Enneking Classification for benign bone tumors. Treatment options were discussed with the patient, and it was planned to do an intralesional curettage with 5 percent phenol and bone graft reconstruction.
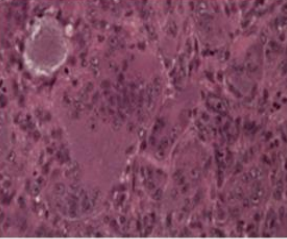
Figure 3: Histopathology diagnosis of Giant cell tumor.
Incision was taken over the distal ulna and a cortical piece of bone was removed to enter inside the cavity. Once inside the cavity, there was presence of chocolate brown gelatinous material. This was emptied with a curette, and it was followed by application of 5 percent phenol with hydrogen peroxide [Figure 4]. This was followed by filling of the bone defect with synthetic bone graft and the bone piece was then fixed back using a cannulated screw [Figure 5].

The patient was asked to follow-up at 1, 3, 6, 12 months post-operatively to evaluate for bone consolidation. After one month, patient completely regained the range of movements of his wrist. There were no signs of recurrence as well.
Cooper and Travers were the first to describe the bone Giant cell tumor in 1818. Nelaton emphasized its local aggression, while Virchow emphasized its malignant potential. It's an uncommon tumor that's mostly benign, but it can act strangely, regardless of the results of radiological or histological diagnosis. Larger tumors may spread into the metaphysis and, in rare cases, into the diaphysis. It is commonly found in the long bone meta-epiphysis and frequently includes the subchondral bone without involving the articular surface. Typical sites include the proximal tibia, humerus, distal femur, and radius. GCT accounts for around 3% to 5% of all bone tumors and 21% of benign bone tumors [1, 2]. In 70% of the cases, it affects women in their third to fourth decades of life. The distal epiphysis of the ulna is a rare location for a primary bone GCT; only 0.45 percent to 3.2 percent of all primary bone GCTs occur here [3]. Amputation or extensive resections with subsequent reconstructions were once used to treat these malignancies. Currently, surgical treatments which are done are Intralesional curettage, Cryotherapy of the cavity after curettage, Curettage and bone grafting, Application of phenol after curettage, Radiation, insertion of methyl methacrylate cement in the cavity after curettage, Resection followed by allograft, En-bloc resection with or without reconstruction or stabilization of the ulna and prosthetic reconstruction. The variables related to the tumor, such as size, location, biological activity, cortical bone destruction or pathologic fracture evidence, determine the treatment [4]. Although an en-bloc resection attacks the tumor aggressively, lowering the probability of recurrence, the functional prognosis is poor. When compared to patients who received adjuvant therapy, a simple curettage delivers a satisfactory functional outcome, but with a recurrence rate of 40% [1–5]. As a result, different adjuvant therapies such as phenol, cryotherapy [6–8], cement, or polymethyl methacrylate (PMMA) administered intraoperatively have been used in curettage. When cement is employed, the recurrence rate ranges from 5% to 8%, and after cryosurgery, it is around 2.3 percent [6, 7]. However, it is worth noting that multicenter research conducted by the Canadian Sarcoma Group [9] found an overall recurrence rate of 17% and stated that the filling material or adjuvant type had no effect on recurrence. Furthermore, certain studies demonstrate that in some circumstances, such as intraosseous GCT, the use of an adjuvant is unnecessary [10]. Therefore, the correct treatment should achieve a balance between oncological radicality and the restoration of skeletal segment functionality. In the present case intralesional curettage was possible because the tumor was a grade II and the reconstruction was carried out with synthetic cancellous bone, due to the young age of the patient.
Osteolytic lesions discovered by chance near the epiphysis of a long bone can be misinterpreted. If treated early and aggressively, this tumor may have an excellent prognosis. It is critical to understand unusual cancer locations to get an accurate diagnosis.
A written informed consent was obtained from the patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
