
Case Report | DOI: https://doi.org/10.31579/2641-0419/184
*Corresponding Author: Rohit Mody, Department of Cardiology, Max Super specialty hospital, Bathinda, Punjab, India
Citation: Rohit Mody, Debabrata Dash, Bhavya Mody, Aditya Saholi, Shubham Sachdeva. (2021) Direct or Direct-Like Stenting in Acute Stemi with High-Grade Thrombus: A Clinical Case Series. J. Clinical Cardiology and Cardiovascular Interventions, 4(13); Doi:10.31579/2641-0419/184
Copyright: : © 2021 Rohit Mody, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 May 2021 | Accepted: 21 June 2021 | Published: 25 June 2021
Keywords: direct stenting; st elevation myocardial infarction; high grade thrombus; primary percutaneous coronary intervention
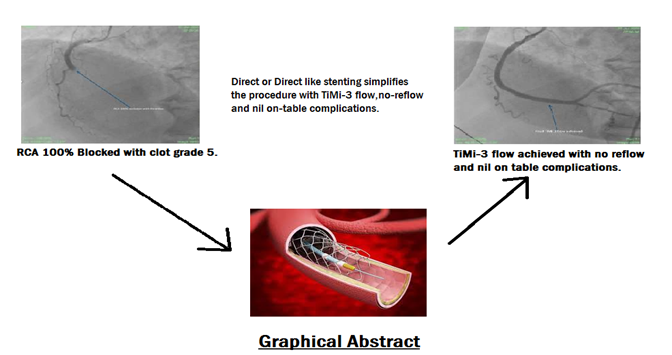
We consider herewith acute ST-elevation myocardial infarction cases having high grade thrombus who underwent direct stenting or direct like stenting of the culprit vessel in those a drug-eluting stent was not crossable directly or distal landing zone was not visible directly after successful guidewire navigation in distal true lumen. All the 4 patients had presented with acute STEMI and high-grade thrombus on angiography. All of them were treated with percutaneous coronary intervention incorporating either direct stenting or direct like stenting. All had a very good angiographic outcome with TIMI 3 flow and MBG >/= 2. In most patients with acute STEMI and high-grade thrombus, direct or direct-like stenting is possible, it simplifies the procedure with almost nil on table complications.
Twee table abstract
Direct and direct-like stenting in patients with high grade thrombus with STEMI is possible in most of the patients. It resulted in TIMI 3 flow and MBG 2 in all our patients. None of them had no-reflow phenomenon.
Lay Abstract
In any case of ST-elevation MI, time is one of the most important aspects. In this process, it is important to minimize the damage to the heart muscle. Therefore, we need to open the culprit artery in a timely and urgent fashion to restore the blood flow to the heart muscle as quickly as possible. During this restoration of the blood flow, we need to minimize the distal embolization of the clot which may be detrimental to the heart muscle. Here, we describe the cases where we have done stenting directly without touching the clot and that resulted in minimal embolization and better outcomes.
Primary percutaneous intervention (PCI) is nowadays the preferred reperfusion strategy in patients with ST-Elevation myocardial infarction (STEMI) which aims to restore both epicardial flow and achieve microvascular perfusion at the earliest. This limits the extent of irreversible myocardial injury [1].
However, with primary PCI emerging as the gold standard, new questions are arising-
Due to these findings, there was an interest in the development of procedural device-based strategies to minimize distal embolization. Among the most studied strategies are distal protection devices, aspiration thrombectomy, and direct stenting [3].
Direct stenting is another method by which we can prevent distal embolization by fixing loose material to the vessel wall that otherwise might have been dislodged during lesion preparation which might have caused distal embolization [4] in the setting of myocardial infarction, there are only five small trials with 754 patients enrolled that compared direct stenting with conventional stenting, which have been summarized in a recent meta-analysis [5]. Direct stenting as compared with conventional stenting, improved reperfusion as evidenced by a significant improvement of ST-resolution and a significant reduction in no-reflow, and was also associated with a significant reduction of in-hospital mortality. Still, there is uncertainty because of the small sample size in these trials. And, the use of DES and adjunctive medical therapy was scarce [3]. In this case series, our patients treated with timely PCI using DS or Direct like stenting indicate that this therapy is useful in reducing no-reflow, improving TIMI flow, nil on-table complications, which might translate into better long-term outcomes
CASE 1
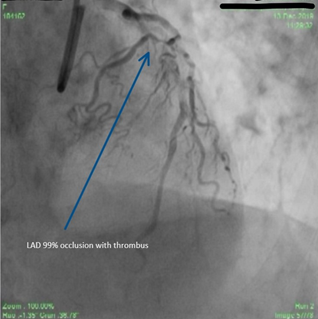
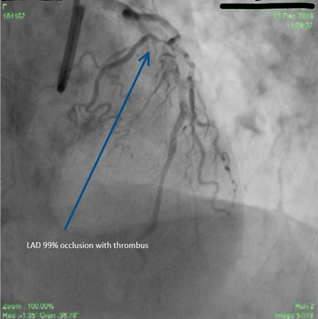
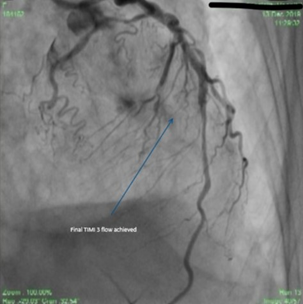
A 57-year-old male patient came with a history of Non-Insulin Dependent Diabetes Mellitus (NIDDM) for 5 years, hypertension for 3 years, and dyslipidemia for 3 years with normal body weight. He presented in the emergency room (ER) with a history of chest pain consistent with angina of 6-hour duration. On admission, the patient’s vitals were stable, blood pressure (BP) of 130/80 mm of Hg, heart rate of 85 beats per minute (bpm), respiratory rate of 20 breaths/minute, SpO2 of 95%. The patient’s electrocardiography (ECG) and echocardiography (ECHO) showed ST elevation in anterior leads, regional wall motion abnormalities (RWMA) in left anterior descending (LAD) territory, and ejection fraction (EF) 28% respectively. Coronary angiography (CAG) done through radial approach, revealed single vessel disease with 100% lesion of proximal LAD having grade 5 thrombus (Figure 1A).

He was taken up for primary PCI through the radial approach promptly. Before primary PCI 300 mg aspirin and 180 mg ticagrelor were administered. Also, an IV bolus of 70 units/kg of heparin and 25 ug/kg bolus of tirofiban was administered. Tirofiban was continued as an intravenous (IV) infusion at a dose of 0.15ug/kg/min for 24 hours. The left main coronary artery (LMCA) was cannulated with an extra back-up (EBU) 3.5 guiding catheter (Medtronic). The lesion was crossed with a BMW guidewire (Boston scientific corporation). After crossing the guidewire, there was a thrombolysis in myocardial infarction (TIMI) 1 grade flow.
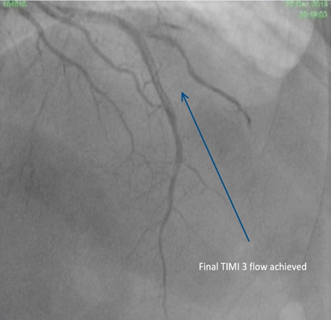
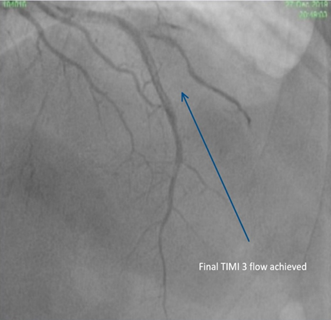
We could assess the distal landing zone. Despite heavy clot burden, we deployed a 3 x 38 mm drug-eluting stent (DES) (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) directly at 16 atm. Post-procedure scores of TIMI 3 flow and myocardial blush grade (MBG) 2 were obtained (Figure 1B).
The patient’s vitals remained stable throughout the procedure (Table 1). The patient was discharged with a prescription of lisinopril, bisoprolol, aspirin, ticagrelor, and rosuvastatin. On follow-up at seven days, the patient was clinically examined in the out-patient department. The patient was asymptomatic and free of angina. ECG showed QS from V1 to V6 with settled ST segments and ECHO revealed an improved EF of 35%. The last follow-up at 6 months was uneventful. ECHO showed an improved EF of 46%. Ticagrelor was discontinued after one year.
A 70-year-old female came with a history of NIDDM, hypertension, and dyslipidemia for the past 10 years with normal body weight. She presented in the ER with complaints of chest pain consistent with angina of 12-hour duration. On assessment, the patient was breathless and hypotensive with a respiratory rate of 27 breaths/minute and BP of 80/50mm of Hg. Bilateral basal crepitations were present. Norepinephrine infusion was started at 3 micrograms/kg/minute and increased up to 10mcg/kg/minute. The patient was started on furosemide infusion for the pulmonary edema. Patient mentation was normal, with slightly cold peripheries and adequate urine output. The patient’s ECG and ECHO showed ST elevation in anterior leads RWMA in LAD territory and EF 26% respectively. After her vitals were stable, she was taken up for PCI. CAG was done immediately and revealed single vessel disease with 99% lesion of proximal LAD having grade 3 clot (Figure 2A).
Before PCI 300 mg aspirin and 180 mg ticagrelor were administered. Also, tirofiban and heparin were given in the same dose as Case 1. Tirofiban was continued as an IV infusion at a dose of 0.15ug/kg/min for 24 hours.
6F EBU 3 guide catheter (Medtronic) was used to engage LMCA. The lesion in LAD was crossed with a BMW guidewire (Boston scientific corporation) and a 3 x 28 mm DES (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) was deployed directly at 16 atm for 30 minutes. The length could be assessed as the distal landing zone was visible. Post-procedure there was TIMI 3 flow and MBG 3 (Figure 2B).

left main coronary artery (LMCA) was cannulated with an extra back-up (EBU) 3.5 guiding catheter (Medtronic). The lesion was crossed with a BMW guidewire (Boston scientific corporation). After crossing the guidewire, there was a thrombolysis in myocardial infarction (TIMI) 1 grade flow.
We could assess the distal landing zone. Despite heavy clot burden, we deployed a 3 x 38 mm drug-eluting stent (DES) (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) directly at 16 atm. Post-procedure scores of TIMI 3 flow and myocardial blush grade (MBG) 2 were obtained (Figure 1B).
The patient’s vitals remained stable throughout the procedure (Table 1). The patient was discharged with a prescription of lisinopril, bisoprolol, aspirin, ticagrelor, and rosuvastatin. On follow-up at seven days, the patient was clinically examined in the out-patient department. The patient was asymptomatic and free of angina. ECG showed QS from V1 to V6 with settled ST segments and ECHO revealed an improved EF of 35%. The last follow-up at 6 months was uneventful. ECHO showed an improved EF of 46%. Ticagrelor was discontinued after one year.
A 70-year-old female came with a history of NIDDM, hypertension, and dyslipidemia for the past 10 years with normal body weight. She presented in the ER with complaints of chest pain consistent with angina of 12-hour duration. On assessment, the patient was breathless and hypotensive with a respiratory rate of 27 breaths/minute and BP of 80/50mm of Hg. Bilateral basal crepitations were present. Norepinephrine infusion was started at 3 micrograms/kg/minute and increased up to 10mcg/kg/minute. The patient was started on furosemide infusion for the pulmonary edema. Patient mentation was normal, with slightly cold peripheries and adequate urine output. The patient’s ECG and ECHO showed ST elevation in anterior leads RWMA in LAD territory and EF 26% respectively. After her vitals were stable, she was taken up for PCI. CAG was done immediately and revealed single vessel disease with 99% lesion of proximal LAD having grade 3 clot (Figure 2A).
Before PCI 300 mg aspirin and 180 mg ticagrelor were administered. Also, tirofiban and heparin were given in the same dose as Case 1. Tirofiban was continued as an IV infusion at a dose of 0.15ug/kg/min for 24 hours.
6F EBU 3 guide catheter (Medtronic) was used to engage LMCA. The lesion in LAD was crossed with a BMW guidewire (Boston scientific corporation) and a 3 x 28 mm DES (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) was deployed directly at 16 atm for 30 minutes. The length could be assessed as the distal landing zone was visible. Post-procedure there was TIMI 3 flow and MBG 3 (Figure 2B).
The patient’s vitals remained stable throughout the procedure (Table 1). The patient was shifted to the cardiac care unit for observation. On day three, the patient was assessed for signs of decreased myocardium perfusion. ECG showed QS from V1 to V6 with settled ST segments and ECHO revealed EF of 28%. The patient was discharged with a prescription of lisinopril, bisoprolol, aspirin, ticagrelor, and rosuvastatin. At three months’ follow-up, the patient was asymptomatic and free of angina. The last follow-up at 6 months was uneventful. ECHO showed an improved EF of 44%. Ticagrelor was discontinued after one year.
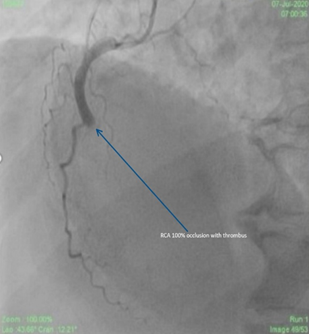
A 65-year-old obese female, with a body mass index (BMI) of 36, dyslipidemic for 5 years, presented to ER with a history of chest pain of 36-hour duration. ECG showed ST elevation in inferior leads. Vitals at the time of admission were stable with a heart rate of 90bpm, BP of 110/70mm of Hg, and respiratory rate of 16 breaths/minute. ECHO showed RWMA in the inferior-posterior wall with an EF of 40% without mitral regurgitation (MR). The patient was taken for PCI in a timely fashion. Her CAG revealed single-vessel disease involving right coronary artery (RCA) - 100% lesion of proximal RCA with grade 5 clot (Figure 3A).
Before PCI 300 mg aspirin and 180 mg ticagrelor were administered. Also, tirofiban and heparin were given in the same dose as Case 1. Tirofiban was continued as an IV infusion at a dose of 0.15ug/kg/min for 24 hours.
A 6 F JR 3.5 guiding catheter (Medtronic) was used to engage RCA. The lesion was crossed with a BMW guidewire (Boston scientific corporation) and a 3 x 26 mm DES (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) was implanted directly at 16 atm. Post-procedure there was TIMI 3 flow and MBG 3 (Figure 3B).

The patient’s vitals remained stable throughout the procedure (Table 1). Just a day after the procedure, ECHO revealed an improved EF of 44% which further increased to 45% by day three (Table 1).
The patient was discharged with a prescription of lisinopril, bisoprolol, aspirin, ticagrelor, and rosuvastatin with advice to follow-up at 7 days, one month, three months, six months, and one year. Ticagrelor was discontinued after one year.
A 60-year-old obese (BMI= 34) male dyslipidemic for the last 10 years, without any history of diabetes and hypertension presented in ER with a history of chest pain consistent with angina of 20-hours duration. On examination, the heart rate was 92 bpm with a BP of 108/72 mm of Hg and respiratory rate of 17 breaths/minute. His ECG showed ST elevation in anterior leads and ECHO revealed RWMA in LAD territory with EF 28%. The patient was taken for PCI in a timely fashion. CAG was done immediately and revealed single vessel disease with 100% lesion of proximal LAD grade 5 thrombus (Figure 4A).

Before PCI 300 mg aspirin and 180 mg ticagrelor were administered. Also, tirofiban and heparin were given in the same dose as Case 1. Tirofiban was continued as an IV infusion at a dose of 0.15ug/kg/min for 24 hours.
LMCA was hooked with 6F EBU 3.5 guiding catheter (Medtronic). The lesion was crossed with a BMW guidewire (Boston scientific corporation) but the stent could not cross the lesion directly. Hence, a small 1.25 x12 mm balloon (AccuForce; Terumo) was used to create a small passage to just visualize the distal landing zone (direct like stenting). Subsequently, 2.5 x 45 mm and 3 x 44 mm DES (Cobalt-chromium everolimus-eluting stent; Xpedition; Abbott Vascular, Santa Clara, California, USA) were implanted distally and proximally at 18 atm respectively. Post-procedure there was TIMI 3 flow and MBG 2 (Figure 4B).

The recovery was uneventful without any complication (Table 1). ECHO after 24 hours of the procedure showed EF of 30%. At discharge, after 3 days EF was 35%. The patient was discharged with a prescription of lisinopril, bisoprolol, aspirin, ticagrelor, and rosuvastatin and advice for regular follow-ups. ECHO was repeated at the six months’ follow-up visit and revealed an EF of 41%. Ticagrelor was discontinued after one year
In patients with STEMI undergoing PCI, several strategies have been used to improve myocardial reperfusion. Direct stenting has been shown to decrease distal embolization and microvascular obstruction in some of the studies [6]. The strategy is widely practiced although no formal guidelines or recommendations for it exist [7]. In a study by Thrombectomy Trialist Collaboration [8], direct stenting was not associated with improved 30 day or 1-year clinical outcomes as compared to conventional stenting, but in this data patients on whom direct stenting was done, many patients had thromboaspiration done before the stenting. Of note, it has been observed that thrombus aspiration during PCI before direct stenting may cause distal embolization as well due to the dottering effect of the thrombectomy device itself. ‘The risk of distal embolization, especially during a hurried maneuver or the inevitable multiple passes required in a large thrombus, cannot be dismissed’ [9]. Hence the effect of direct stenting for preventing distal embolization could not have been fully exploited.
The Thrombectomy Trialists Collaboration [8] performed the largest observational study comparing direct stenting with conventional stenting during PPCI. They also addressed its interaction with aspiration thrombectomy [10]. In this study, 32% of the 17329 patients included underwent direct stenting. Direct stenting was performed more often in patients who underwent aspiration thrombectomy as compared to those with conventional PCI (41% vs. 22%; P < 0>
Specifically, 30-day incidences of cardiovascular death or cerebrovascular events were low and not significantly different between direct stenting and conventional stenting (1.7% vs. 1.9%). There were no significant differences in all-cause mortality, myocardial infarction, and stent thrombosis. The 1-year incidence of vessel revascularization was lower after direct stenting than after conventional stenting (4.3% vs. 5.6%). Nevertheless, this finding is important. It has been previously believed that direct stenting may result in inadequate sizing of the stent resulting in an increased risk of stent thrombosis and restenosis. But the current analysis makes these concerns insignificant by showing a trend in the opposite direction. In TAPAS [11] and TOTAL [12] 6534 propensity-matched patients, incomplete ST-segment resolution (<70>
Only a trend towards improved ST-segment resolution by direct stenting was noted (P = 0.06). Thus, the current analysis failed to prove a favorable effect of direct stenting on myocardial perfusion which had been the putative mechanism for a clinical benefit. There is no doubt that distal protection devices capture embolized material during PPCI and that aspiration thrombectomy removes thrombus and reduces thrombus burden; it is also highly intuitive that direct stenting reduces distal embolization. A positive effect of these measures on distal reperfusion, however, has been hard to demonstrate. By the time of PPCI, the STEMI has already caused prior distal embolization of thrombus and plaque. Reperfusion injury may worsen this. Thus, only one among the many elements of reperfusion in STEMI can be modified by using device-based strategies. In the current era of optimized PCI and adjunctive treatment, this limited effect may not translate into a meaningful clinical benefit. As the mortality in uncomplicated STEMI is already very low—1.8% at 30 days and 2.9% at 1 year, it is very hard to show further improvement [3].
But the positive effects of DS cannot be denied. In a recent article, it has been concluded that in patients with acute reperfused STEMI, DS is safe and feasible with a significant reduction of infarct size compared to CS and subsequent lower incidence of heart failure hospitalizations and mortality [13]. But some other studies did not show any significant difference between DS and CS [14,15,16,17].
A meta-analysis that included 7 studies comparing DS and CS strategies revealed a lower adverse event rate with DS. Studies included in this meta-analysis were mostly observational and utilized first-generation drug-eluting stents. Patient and lesion selection may explain these positive results [18,19].
Despite high clinical and angiographic risk profile, the Swedish Coronary Angiography and Angioplasty Registry (SCARR registry) established very low rates of clinical restenosis and stent thrombosis (close to 1% and 0.5%, respectively) while reporting the clinical outcomes in a patient treated with state-of-the-art DES. Thus, we have almost achieved victory in the battle of restenosis. In view of such encouraging outcomes, it seems difficult to obtain a sizeable benefit with the compulsory use of DS [20].
‘The meta-analysis - Comparing Direct Stenting with Conventional Stenting in Patients with Acute Coronary Syndromes: A Meta-Analysis of 12 Clinical Trials’ demonstrated that in selected patients with ACS, DS is not only safe and feasible but also reduces short-term and 1-year mortality as well as the occurrence of after-procedural no-reflow phenomenon [21].
A predefined sub-study of the LIPSIA CONDITIONING trial was a prospective, controlled, single-center randomized trial investigating the effects of ischemic preconditioning plus postconditioning in STEMI patients undergoing primary PCI. 171 patients who underwent conventional stenting with balloon pre-dilatation were case-matched to 171 patients who underwent direct stenting for age (+ 5 years), sex, and TIMI flow before PCI. Three-vessel coronary artery disease (CAD) was more prevalent in the conventional stenting group and thrombectomy was used more often in the direct stenting group. The results of the study showed that direct stenting resulted in a significantly smaller infarct size on MRI 2-5 days after the index event (16% vs. 19%) and a lower 6-month mortality rate (5% vs. 12%) [22].
As the mortality of primary angioplasty in recent years has decreased considerably with a mortality of less than 2% in uncomplicated MI, the subtle effect of DS on mortality might not be easily demonstrable. But this concept should be extrapolated to high-risk patients like patients of STEMI in Cardiogenic shock [23].
The take-home message is that, if direct stenting or direct-like stenting is done in patients with high-grade thrombus in the setting of STEMI, the distal embolization is minimal as observed in these patients. In case direct stenting is not possible, a direct like stenting following pre-dilatation with a small balloon could be performed. In literature also, deflated balloon-assisted direct stenting has been reported and has shown to increase the success rate of direct stenting [24]. By using direct stenting, even in patients of high-grade thrombus, we have not used thrombosuction in any of the patients.
In most patients direct stenting is feasible. In patients in whom stent does not cross or distal vessel landing zone is not visible direct-like stenting can be performed successfully and even thrombosuction can be avoided. Direct or direct-like stenting simplifies the procedure with less contrast used and nil on table complications. TIMI 3 flow is achieved in all and distal embolization is less. However, a proper randomized controlled trial is warranted further to demonstrate if this strategy of direct or direct like stenting without the use of thrombectomy is more useful and has an impact on hard clinical outcomes. In a nutshell, our study and discussion point to a strategy where we should be as direct as possible while dealing with patients of primary PCI in STEMI.
In most patients with acute STEMI and high-grade thrombus, direct or direct-like stenting is possible. Direct or direct-like stenting simplifies the procedure with less contrast used and almost nil on table complications. TIMI grade 3 flow can be achieved more often and the incidence of distal embolization is very less.
No funding has been received for the current study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
I confirm that all figures and tables are original and created by me specifically for use in this paper.
Ethics approval and consent to participate
Ethical approval was not required since it is an accepted procedure.
Consent for publication
Written consent has been obtained to publish the case report from the guardian. The consent copy is available with the authors and ready to be submitted if required.
Competing interests
The authors declare that they have no competing interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
