
Case Report | DOI: https://doi.org/10.31579/2690-4861/336
University of Kinshasa.
*Corresponding Author: Israël Maoneo Azabali, University of Kinshasa.
Citation: Israël M. Azabali, Antoine B. Kalubye, Dieu M. K. Kantenga, Pierre Mukuetala I. Mukuetala, Glennie N. Eba, (2023), Dichotomous Profile of Thoraco-Lumbar Dislocation Fractures. Case Report and Review of the Literature, International Journal of Clinical Case Reports and Reviews, 14(4); DOI:10.31579/2690-4861/336
Copyright: © 2023, Israël Maoneo Azabali. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 August 2023 | Accepted: 14 September 2023 | Published: 22 September 2023
Keywords: thoracolumbar fracture dislocation; denis' three columns; magerl classification
Dislocated thoracolumbar fractures are uncommon injuries following a major trauma. We report a case of thoraco-lumbar dislocated fracture of which radiological finding was in discrepancy with clinical aspect and postoperative neurological recovery. A 32-year-old female admitted in Neurosurgery Department of the University Hospital of Kinshasa for low back pain, functional impotence of lower limbs and urinary retention following a road traffic accident three weeks prior. She presented a painful swelling at level of T12-L2 spinous processes and Wagner's grade IV gluteal pressure sores. Neurologically, on both limbs, the sensation was preserved and motor strength was graded 3/5 globally. CT-Scan showed a fracture of the vertebral body and pedicles of L2 with retrolisthesis of L1/L2 grade IV (Magerl B.3.3). She underwent posterior spinal decompression followed by spinal stabilisation with pedicle screws. The gluteal ulcers were debrided and sutured during the same surgery. Postoperatively, the pressure ulcers healed and the patient recovered full motor and urinary sphincter functions after twelve months of physiotherapy. This case report demonstrates the possibility of discordance between radiological images of dislocated thoracolumbar fractures and spinal cord injury clinical.
Thoracolumbar injuries are very common compared to other spinal segments [1]. More than 90% of spinal injuries are located at the thoracolumbar region (T11-L2) [2]. This transition zone between the rigid dorsal column and the mobile lumbar column constitutes a point of weakness exposed to various traumas. Fracture dislocations are rare lesions whose production requires a high-energy trauma leading to the rupture of three spinal columns [3]. The rupture of all three columns by a major trauma leads to instability of the spine, likely to cause a dislocation (Denis’s type III injury) with a very high risk of spinal cord or nerve root injury [4]. In the majority of cases, high-grade thoracolumbar dislocation fractures are manifested by complete neurological deficit [3]. Cases with incomplete or no neurological deficit are rare. We report a case of a grade IV traumatic thoracolumbar fracture dislocation with incomplete neurological deficit treated in our department in order to discuss the discrepancy between the radiological finding and the clinical and therapeutic aspects.
We report a 32-year-old female patient, referred from a peripheral hospital on 3rd February 2021 to the Neurosurgery Department of the University Teaching Hospital of Kinshasa for low back pain, functional impotence of the pelvic limbs and urinary retention following a road traffic accident three weeks prior. Her past medical and surgical history was unremarkable.
On examination, she was stable and coherent, pink and vital signs were within normal limits. In the dorsolumbar region, there was swelling in regard to L1-L2. Palpation revealed moderate tenderness. In the gluteal region, there was an oval wound in the upper-internal quadrant of the right buttock, about 8/6 cm in diameter, covered with a whitish crust. And on the superior-internal quadrant, an oval wound, 12/10 mm in diameter, covered with a blackish crust. In the genital area, the urinary catheter connected to the collecting bag was in place with clear urine.
Neurologically, Glasgow coma Scale was 15/15. The pupils were equal and reactive to light. She had paraparesia with global power of 3/5. Sensation was preserved on both lower limbs. She was classified as ASIA C. The anal sphincter was slightly tonic and bulbocarvenosus reflexe was present.
Thoraco lumbar CT scan showed fracture with bony fragments of the L1 vertebral body along the right inferior articular process with a Meyerding grade 3 retrolisthesis of L1 on L2 corresponding to Magerl B.3.3. Displaced fractures of the left transverse process of L1, two transverse processes and pedicles of L2 and the right transverse process of L3 were also noted on these CT scans. Finally, the CT scan showed the loss of lumbar lordosis (Figure 1A, B, C).
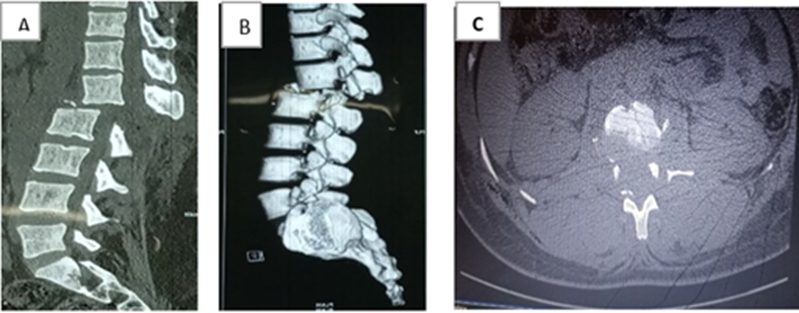
Figure 1: Preoperative CT images showing retrolisthesis on sagittal slices (A-B) and fracture of the pedicles and transverse processes of L2 on an axial slice (C).
The results of the biological examinations performed were within the normal range. In view of the above, we made a diagnosis of incomplete spinal cord injury secondary to fracture dislocation of L1/L2, ASIA C, Meyerding grade IV and Wagner stage II sacral pressure sores. Spinal decompression surgery followed by spinal stabilisation was indicated. Eleven weeks later, the patient underwent spinal stabilisation and spinal decompression laminectomy via the posterior approach. Stabilisation was performed using two parallel rods attached to 8 pedicle screws, 4 on each side, placed at 4 levels (D12, L1, L2 and L3) under §uoroscopy. This stabilisation was preceded by contraction of two dislocated spinal ends (Figure 2). During the same procedure, the gluteal ulcers were debrided and sutured in two layers, first with number 2/0 vicryl and then with number 0 monofilament nylon.
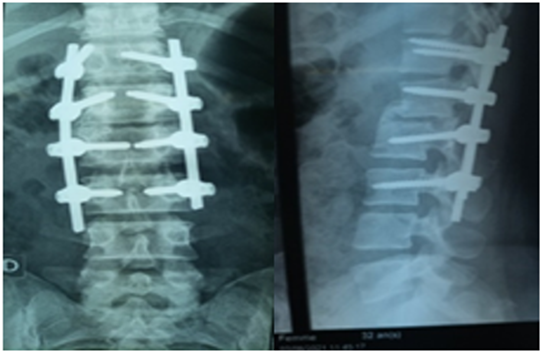
Figure 2: Postoperative images showing reduction and stabilisation with pedicle screws.
Postoperatively the patient could regain power and could stand up at one week, followed by walking with a walking frame at three weeks and normal walking at two months after several sessions of rehabilitation and physiotherapy (Figure 3). She also recovered the vesico-sphincter function.

Figure 3: Patient regained power, standing station and walking.
Thoracolumbar dislocation fractures are uncommon. Mostly young people between 15 and 35 years of age are affected as a result of road accidents or falls from height [5]. Because of the high degree of violence required to produce dislocated fractures, they are often associated with major neurological deficits, such as complete paraplegia [3, 6].
The reported case is a dislocation fracture of the thoracolumbar hinge (L1-L2) in a 32-year-old female patient following a traffic accident. Clinically, the patient presented with paraparesia and urinary retention (ASIA C). Radiologically, it is a grade IV dislocation fracture, Magerl type B.3.3. The radio-clinical dichotomy is explained by the fact that such a type of lesion should normally manifest itself as a complete paraplegia (ASIA A) and not an incomplete neurological deficit. Several authors have reported cases similar to ours, even complete fracture dislocations, Meyerding grade V, without neurological deficit. They have tried to explain this radio-clinical discrepancy by the possibility of spontaneous decompression caused by the separation of the anterior column from the middle column following the fracture of the pedicles during the trauma. This would enlarge the spinal canal and preserve the cord from traumatic injury [5, 6, 7, 8]. In our case, the pedicles were ruptured, which could justify this incomplete neurological deficit.
This case demonstrates the possibility of discordance between radiological images of thoracolumbar dislocation fractures, spinal cord injury, clinic and postoperative neurological recovery.
Limit of study: MRI was not performed. It was not available during that period; But the surgery findings revealed a slight damage to the spinal cord and nerve roots.
The authors do not have a financial relationship with any organization that sponsored the research.
The authors declare that they have no conflict of interest.
IM followed the case, collated the figures, wrote the manuscript and sought consent from the patient.
PM was the senior physician overseeing the case.
DK corrected the manuscript English version.
AB supervised the work.
GN was the principal operator and the supervisor of the article redaction.
All the authors read and approved the final manuscript
Not applicable
Not applicable
We declare that we have obtained written consent for publication.
Not applicable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
