
case report | DOI: https://doi.org/10.31579/2690-1897/205
Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
*Corresponding Author: Ibrahim Haruna Gele, Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
Citation: Karra A, Gargouri A, Ghorbel I, Kammoun C, Hammami F, Henteti Y, et al, (2024), Diaphyseal Aclasia (Multiple Exostosis) In an Adult: A Case Report of Rare Giant Lesions with Review of The Imaging Features, J, Surgical Case Reports and Images, 7(6); DOI:10.31579/2690-1897/205
Copyright: Karra A, Gargouri A, Ghorbel I, Kammoun C, Hammami F, Henteti Y, et al, (2024), Diaphyseal Aclasia (Multiple Exostosis) In an Adult: A Case Report of Rare Giant Lesions with Review of The Imaging Features, J, Surgical Case Reports and Images, 7(6); DOI:10.31579/2690-1897/205
Received: 02 July 2024 | Accepted: 18 July 2024 | Published: 26 July 2024
Keywords: Diaphyseal aclasia; Giant Lesions; Plain Radiograph
Exostosis or osteochondroma is a bony developmental anomaly, which arise from exophytic outhgrowth on bone surfaces in a characteristic manner. They are usually solitary. The multiple osteochondromas (MO) are known as diaphyseal aclasia or hereditary multiple exostoses (HME)3,4. MO is a rare disorder with an estimated prevalence of 1:20,000 - 30,0005,6. There are many reports of exostosis with a solitary giant lesion and otherwise on multiple giant lesions. A 24 year old male presented with complain of multiple body swellings in the lower limbs and the chest of about 15 years duration. The onset was insidious and gradually increases in size. They are painless but occasionally experience numbness in the left lower limb. Physical examination, revealed multiple large masses noted at the knee bilaterally. They appear hard and non tender with normal skin over them. There was limitation of flexion at the knee. Plain radiographs demonstrate giant bony or lesions in the distal femurs and the proximal aspect of left tibia and fibula. The lesions are seen to grow away from the adjacent joint and shows calcification in their distal end (cap). Similar lesions to a lesser extend were demonstrated in the proximal right tibia and fibula and the distal left fibula. Chest radiograph shows sessile bony density lesions in the region of the right 5th anterior and left 6th posterior ribs (fig. 3). A diagnosis of multiple exostosis was made. The patient later had surgery with removal of the lesions in stages. Histology report confirms osteochondroma.
Exostosis or osteochondroma is a bony developmental anomaly, which arise from exophytic outhgrowth on bone surfaces in a characteristic manner. [1] It is the most common benign bone tumor and has a male preponderance (M:F = 2:1)[1,2].
Exostosis are usually solitary. The multiple osteochondromas (MO) are known as diaphyseal aclasia or hereditary multiple exostoses (HME) [3,4] MO is a rare disorder with an estimated prevalence of 1:20,000 - 30,000 [5,6]. These tumours arise mainly in tubular bones near the metaphyses related to the sites of tendinous attachments. They are particularly common around the knee and proximal end of the humerus [3]. The lesions manifest more in early childhood, may involute with increasing age and usually cease to grow with skeletal maturity [3,5,4,2,7].
The index case is peculiar because of the multiplicity of the giant lesions (fig 1 and 2).
A 24-year-old man presented at the orthopaedic unit of Usmanu Danfodiyo University Teaching Hospital with complain of multiple body swellings in the lower limbs and the chest of about 15 years duration. The swelling was noted first in the left lower limb followed by right lower limb and then the chest. The onset was insidious and gradually increases in size. They are painless but occasionally experience numbness in the left lower limb. There is associated limitation of movement at the knees and of recent find it difficult to do his usual activity. No history of trauma. Not a known sickle cell disease, diabetic mellitus or hypertensive patient. He had visited a primary health care facility in his village in the past, which he was prescribed some medications to no avail. He is single, living with his parents in a polygamous setting, engage in farming activities. No family history of similar swelling. Physical examination shows a young man, anxious but not in any painful or respiratory distress. Not pale, anicteric. Vital signs were satisfactory. Multiple large masses were noted at the knee bilaterally. They appear hard and non-tender with normal skin over them. The largest was noted at the left knee. There was limitation of flexion at the knee. Similar masses were noted in the distal left leg and the right anterior aspect of the chest. Other systemic examinations were unremarkable. A provisional diagnosis of multiple exostosis was made and refer him to radiology department for x-ray. Plain radiographs of femurs, knees and legs reveals giant bony outgrowth or lesions in the antero-medial aspect of the distal femurs and the proximal aspect of left tibia and fibula (fig 1 and 2). The lesions are seen to grow away from the adjacent joint and shows calcification in their distal end (cap). Similar lesions to a lesser extend were demonstrated in the proximal right tibia and fibula as well as the distal left fibula (fig 2). Postero-anterior chest radiograph shows sessile bony density lesions in the region of the right 5th anterior and left 6th posterior ribs (fig. 3). A diagnosis of multiple exostosis (diaphyseal aclasia) was made. The patient later had surgery with removal of the lesions in stages. Histology report confirms osteochondroma.


Figure 1: Cone down antero-posterior view of distal femurs showing giant exostoses with areas of calcification bilaterally (arrows)
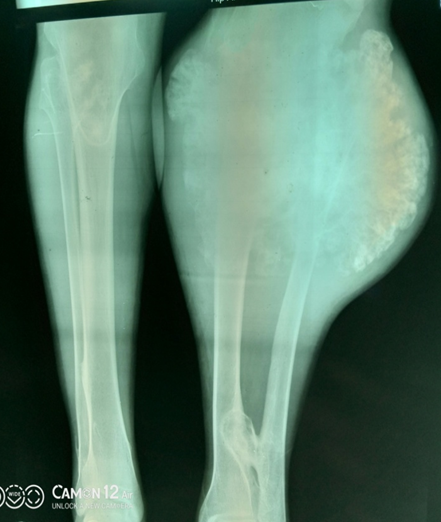

Figure 2: Radiograph of both legs antero-posterior view and the left knee lateral view showing giant exostoses with calcification of the cap in the proximal left tibia and fibula. Also note exostoses in the proximal right tibia and distal left fibula (arrows).
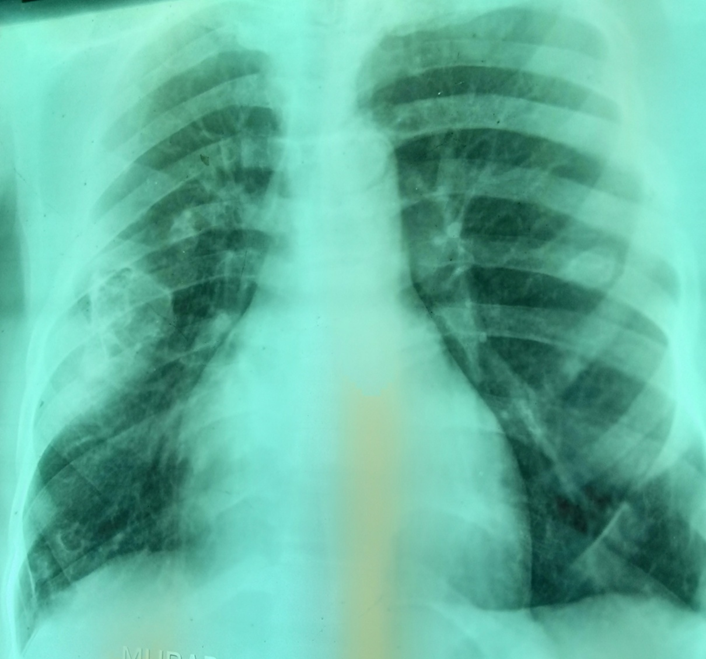
Figure 3: Chest postero-anterior view showing a bony density structures in the regions of the right 5th anterior and left 6th posterior ribs (arrows)
Exostosis is the most common benign bone tumour accounting for 35% of benign bone tumours and 8% of all bone tumours [2]. They occur most frequently in long bones commonly around the knees (distal femur and proximal tibia) and then the proximal humerus 1. Unusual sites such as spine, rib and pelvis has been reported [4,5,7]. The index case also has lesion involving the ribs as shown in (figure 3). Osteochondroma can be solitary or multiple, pedunculated or sessile [2,7]. The solitary form is commoner and non-hereditary. The exact etiology of the growth is not known but the peripheral portion of the epiphysis is thought to herniate from the growth plate. The herniation may be idiopathic or may be the result of trauma or a perichondrial ring deficiency resulting in abnormal extrusion of metaplastic cartilage that responds to the factors that stimulate growth plate and this result to exostosis growth [2,7,8]. Multiple exostosis disease is an autosomal dominant disorder known as hereditary multiple exostoses (HME) or diaphyseal aclasia characterized by the development of multiple bony outgrowths [2]. About 80% of cases of multiple exostosis have an identifiable mutation in one of two genes, exostosin-1 (EXT1) and exostosin-2 (EXT2) on chromosomes 8 and 11 respectively. These genes are believed to code for transmembrane glycosyltransferases partly responsible for regulation of heparin sulphate proteoglycans involved in cell signaling and chondrocyte proliferation and differentiation [9,10]. Solitary and small osteochondromas are usually asymptomatic and are discovered incidentally during radiological examination [1]. Multiple and large lesions present with deformity, restriction of joint movement and pressure symptoms. Complications commonly associated with these lesions include bony deformity, fracture, vascular compromise and neurological sequele due to compression of adjacent vessels or nerves. The lesion may also undergo malignant transformation. The risk of malignancy has been estimated to range from 1 – 25% of HME cases [2,5,9]. Imaging is the investigation of choice in evaluating patient with suspected exostosis. The imaging modalities used include plain radiography, computed tumography (CT), magnetic resonance imaging (MRI) and radionuclide scan. Osteochondroma on plain radiograph show characteristic appearance which alone can be sufficient for diagnosis. The tumour shows a combination of radiolucent cartilaginous cap with varying degree of ossification and calcification that increases with age. They may appear as sessile with broad base or pedunculated lesion with narrow base11. In long bones, typically tumour arises at end of bone and grows away from the adjacent joint as demonstrated in this case. CT and MRI demonstrate the cartilage cap more clearly and show continuation of the cortex and medulla of the lesion with that of the host bone. Evaluation of thickness of the cartilaginous cap can also be done with CT and MRI. However, it is best evaluated on MRI because of the high signal intensity on T2W images. Thickening of the cap greater than 1cm on MRI is suspicious of sarcomatous change [1,3]. In addition MRI can assess compression of spinal cord or nerves caused by exostosis. Vascular compression is evaluated with angiography. Positron emission tomographic (PET) scan is occasionally done to evaluated for benignity or otherwise of the tumour. Increase or high grade fluorodeoxyglucose (FDG) uptake suggest malignant degeneration [4]. Differential diagnosis of exostosis include giant cell tumour, fibrous dysplasia and chondrosarcoma. These can be differentiated by the characteristic radiological appearance of exostosis earlier described. The treatment of osteochondroma depends on the size or deformity caused as well as the symptoms of lesion. Tumours that are small and asymptomatic or minimally symptomatic are given supportive care and follow up, while larger and symptomatic lesions are surgically resected [5].
Giant exostoses are rare and usually solitary. We report a rare case of multiple giant lesions (diaphyseal aclasia) on plain radiograph with review of imaging features.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
