
Review Article | DOI: https://doi.org/10.31579/2690-4861/789
Radiodiagnosis Department, Faculty of Medicine, Misr University for Science and Technology.
*Corresponding Author: Umar Muhammad Darma, Radiodiagnosis Department, Faculty of Medicine, Misr University for Science and Technology.
Citation: Marwa A. Shaaban, Yousef Ahmed, Umar M. Darma, (2024), Diagnostic Performance of Gray Scale Ultrasound and Elastography in Solid Thyroid Nodules, International Journal of Clinical Case Reports and Reviews, 21(1); DOI:10.31579/2690-4861/789
Copyright: © 2024, Umar Muhammad Darma. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 November 2024 | Accepted: 19 December 2024 | Published: 31 December 2024
Keywords: gray scale ultrasound; elastography; solid thyroid nodules
Background: Thyroid nodules are common diseases, and their incidence has increased rapidly during the past decades. Thyroid nodules detected by ultrasound (US) have been detected in up to 50% of the general population.
Objective: To evaluate the diagnostic performance of Gray-scale ultrasonography (US) and elastography in differentiating benign and malignant thyroid nodules.
Data Sources: Medline databases (PubMed, Medscape, ScienceDirect. EMF-Portal) and all materials available in the Internet till 2023.
Conclusion: Innovative advances in high-resolution ultrasound now enable detailed anatomical characterization and accurate differentiation of benign from malignant disease. Ultrasound has become the core component of thyroid nodule guidelines, but it is important that the key technological aspects of the modality are understood and that challenges and limitations remain with the technique.
Benign and malignant thyroid nodules are treated differently: the 2015 edition of the American Thyroid Association’s “Guidelines for the Diagnosis and Treatment of Adult Thyroid Nodule and Differential Thyroid Cancer” recommends surgery for malignant thyroid nodules but no further treatment for benign nodules. Therefore, it is important to distinguish between benign and malignant thyroid nodules. At present, Ultrasound is the preferred imaging method for thyroid nodules, but it has limitations in differential diagnosis between atypical benign and malignant nodules [1].
Thyroid Ultrasound (US) being easily accessible, noninvasive, and cost-effective, is a key examination for the management of thyroid nodules. Thyroid US assessment of the risk of malignancy is crucial in patients with nodules, in order to select those who should have a Fine Needle Aspiration (FNA) biopsy performed. Certain features of thyroid nodules on Ultrasound (US) are predictive of malignancy and are used as criteria for FNA. Ultrasound characteristics that have been reported as potential predictors of thyroid malignancy include irregular margins, hypo-echogenicity, absence of a halo, a predominantly solid composition, or presence of calcification. These criteria have various sensitivity and specificity, but unfortunately none of them alone is sufficient to discard or detect malignancy efficiently [2].
Ultrasound elastography, which was introduced in the 1990s, provides real-time information regarding the tissue elasticity and allows in vivo assessment of the tissue's mechanical properties, mapping of tissue stiffness, and characterization of soft tissue lesions. Ultrasound elastography is based on the principle that, under compression, the softer parts of tissues deform easier than the harder parts. Ultrasound Elastography is reported to be useful in differentiation of the benign and malignant lesions of the prostate, breast, pancreas, and lymph nodes. In the last years, important studies have been conducted in the differential diagnosis of thyroid nodules by US elastography [3].
Anatomy of Thyroid Gland
The anatomy and pathology of the thyroid gland can be thoroughly demonstrated by the ultrasound. Structures such as vascular structures, lymph nodes and related structures are clearly visible. An adequate comprehension of the normal anatomy of the thyroid is mandatory for the appropriate understanding of the gland and its pathologies [4].
The gland varies from an H to a U shape and is formed by 2 elongated lateral lobes with superior and inferior poles connected by a median isthmus, with an average height of 12-15 mm, overlying the second to fourth tracheal rings. The isthmus is encountered during routine tracheotomy and must be retracted (superiorly or inferiorly) or divided. Occasionally, the isthmus is absent, and the gland exists as 2 distinct lobes [5].
The lobes of the thyroid gland are wrapped around the cricoid cartilage and superior rings of the trachea. The gland is located within the visceral compartment of the neck (along with trachea, esophagus and pharynx). This compartment is bound by the pre-tracheal fascia [5].
Ultrasound Anatomy of the Thyroid Gland
Thyroid ultrasound uses sound waves to produce pictures of the thyroid gland within the neck. It does not use ionizing radiation and is commonly used to evaluate lumps or nodules found during a routine physical or other imaging exam [6].
A good understanding of the anatomic structures of the neck surrounding the gland is a requisite for safely performing image guided procedures on the thyroid gland. Patients presenting for treatment of thyroid nodules can have anatomy that is distorted by the nodules or by prior surgery [6].
High-resolution ultrasound is considered the best imaging technique for evaluating the thyroid gland, as it is accessible, non-invasive, and highly sensitive concerning the detection and characterization of thyroid nodules [7].
Thyroid ultrasound is performed for multiple indications including but not limited to confirmation of a thyroid nodule, nodule characterization, differentiating thyroid lesions from other cervical masses, evaluation of thyroid parenchyma, postoperative evaluation for residual or recurrent tumor, cancer screening (such as multiple endocrine neoplasia or MEN), and to guide FNA/biopsy [8].
Elastography of the Thyroid Gland
High-resolution ultrasound (US) is the most sensitive modality for the noninvasive identification and evaluation of thyroid nodules [9].
Elastography is a promising new technique that may improve the US evaluation of Thyroid nodules. Elastography was developed at the University of Texas Medical School, Houston, by Trimboli and colleagues [9]. This technology evaluates tissue stiffness.
Ultrasound elastography (USE) allows the visualization of the displacement and deformation of tissue by applying external force, as well as the remodeling of tissue after cessation of the external force. The changes both within the tissue exposed to strength and its surroundings can be measured, and the elasticity values of the tissue of interest can be determined semi quantitatively and/or quantitatively [10].
Malignant lesions tend to be stiffer than the surrounding benign tissues. There are two general US methods for determining Thyroid nodules stiffness; when a force is applied to the tissue, either the deformation parallel to the force direction (strain) or the deformation propagating perpendicular to the force direction (shear wave) is measured by using US signals [11].
Pathology of the Thyroid Gland
The incidence of all thyroid diseases is higher in females than in males. Nodular thyroid disease is the most common cause of thyroid enlargement [3].
Majority of patients with thyroid disease present with midline neck swelling, occasionally causing dysphagia and hoarseness of voice. Broadly the thyroid diseases are classified into three categories:
i) Benign thyroid masses,
ii) Malignant tumors of thyroid gland, and
iii) Diffuse thyroid enlargement (3).
Differentiation between benign and malignant nodules is important and even though fine needle aspiration (FNA) is the gold standard for diagnosis, pre-screening with ultrasound (US) is essential since performing FNA in all nodules is not feasible. US elastography is an additional non-invasive tool that is available and able to differentiate between benign and malignant nodules [12].
Multiplicity of the nodule is not an indicator of benignity. The incidence of malignancy is same in solitary nodules as it is in multiple nodules [12].
Clinical history: A 37 years old woman underwent a routine evaluation. A solid hypoechoic nodule in the central region of the right thyroid (a) 3 in transverse (arrows) and (b) 5 in longitudinal (arrows) strain elastography images.
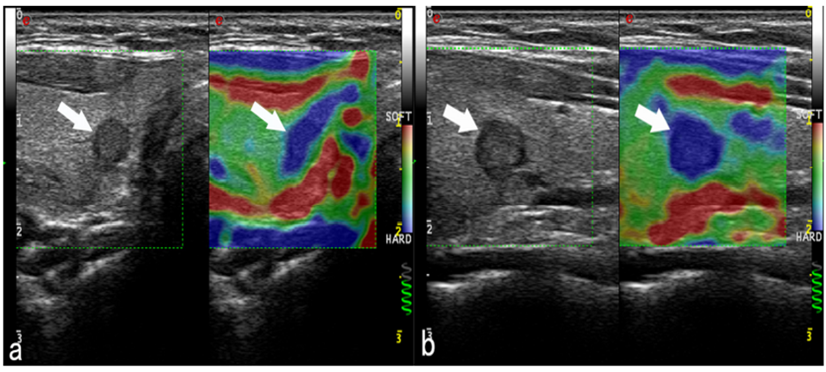
The final diagnosis reached: papillary thyroid carcinoma.
Case history: a 43year old woman underwent a routine evaluation. A solid hypo echoic nodule in the dorsal region of the left lobe of the thyroid was scored 3 in both (a) transverse arrows and (b) longitudinal arrows strain elastography images.
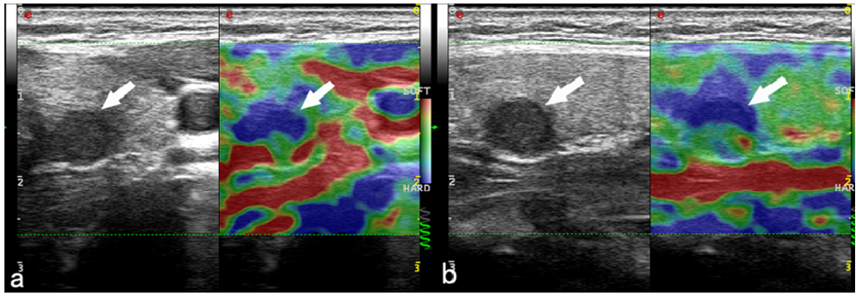
Final diagnosis: papillary thyroid carcinoma.
Case history: A 53-year-old male patient with hypoechoic mass in the right thyroid lobe with irregular margins and heterogenous appearance. Strain elastography showed a relatively hard nodule with a strain ratio with the surrounding parenchyma of 3.98 and hence suspicious for malignancy.
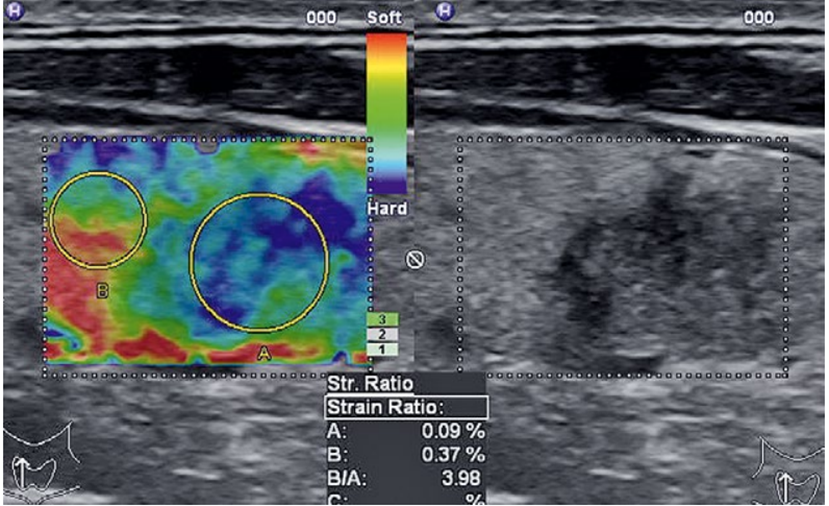
Final diagnosis: Histopathology after thyroidectomy showed a papillary thyroid carcinoma.
lastography has been introduced to evaluate hardness objectively, to improve the diagnostic performance of gray-scale US examination in differential diagnosis of thyroid nodules, and to eventually reduce unnecessary benign biopsies in thyroid nodules [13].
Many previous studies have proved that elastography is useful in differentiating malignant from benign nodules [14].
Elastography is usually performed in thyroid nodules detected at grayscale US, and the high diagnostic performances of combinations of suspicious gray-scale US features are validated through many previous studies as well as in our study. Accordingly, for elastography to be used widely as an adjunctive diagnostic tool supporting gray-scale US or to be used as a separate diagnostic tool, several conditions should be fulfilled. The diagnostic performance of elastography itself or a combination of elastography and gray-scale US should be superior to that of gray-scale US alone [14, 15].
Although Rago et al demonstrated that elastography with freehand technique shows high diagnostic performances even in nodules smaller than 10 mm, we found that specificities, PPVs, NPVs, accuracies, and in nodules larger than 10 mm and larger than 5 mm were inferior to those in nodules 10 mm or smaller and 5 mm or smaller, respectively. Nodules 5 mm or smaller, specifically, accuracies and ORs of gray-scale US [15]. Suspicious gray-scale US features have high false-positive rates in nodules 5 mm or smaller [16]
In our study, the false-positive rates of the three criteria sets were also high in nodules 5 mm or smaller. In nodules smaller than or equal to 5 mm, both gray-scale US and elastography have their limitations in predicting thyroid malignancy, although the clinical importance of these small cancers is not clear.
US is the preferred technology for thyroid nodules due to its convenience, maneuverability and low cost. Conventional US malignant characteristics, including microcalcifications, hypo echogenicity, irregular margins, and taller than wide were significantly different between malignant and benign nodules in this study. Logistic regression analysis showed that microcalcifications, taller than wide, irregular margins and ETE were independent predictors of malignancy. However, previous studies have reported largely varied sensitivities and specificities [17]
The diagnostic efficacy of conventional US parameters in this study was also unsatisfactory. Although irregular margins and ETE yielded good sensitivity, their specificity was rather poor. Similarly, despite their high specificity, the sensitivity of taller than wide and disrupted rim calcifications with a small extrusive hypoechoic soft tissue component was unacceptable. The accuracy of conventional US parameters was also limited.
Elastography takes advantage of the change in elasticity of soft tissues resulting from specific pathological or physiological processes, and the low elasticity observed on USE is highly correlated with malignancy. Since the emergence of elastography, it has shown an outstanding sensitivity, specificity, PPV and NPV [12], with the specificity and PPV reaching up to 100%.
Elasticity, which is absent in conventional US, is the single feature with the best diagnostic performance (17), as well as a potent predictor of malignant thyroid nodules [14].
With an increase in the ES, the percentage of malignancy increased significantly in our study, confirming that the ES is correlated with malignancy. In this research, we used the 5 scoring parameters proposed by Itoh, who defined an ES > 3.5 as the cut-off value; the sensitivity, specificity, accuracy, PPV and NPV were 92.4, 60.7, 79.0, 76.3 and 85.5%, respectively, with an AUC of 0.828. However, contrary opinions have also been presented. A multicenter study by Moon et al. reported that elastography showed an inferior performance in the differentiation of malignant and benign thyroid nodules relative to grayscale US features [18].
Innovative advances in high-resolution ultrasound now enable detailed anatomical characterization and accurate differentiation of benign from malignant disease. Ultrasound has become the core component of thyroid nodule guidelines, but it is important that the key technological aspects of the modality are understood and that challenges and limitations remain with the technique. The large evidence base for ultrasound elastography indicates that the assessment of nodule stiffness can improve the imaging evaluation of thyroid lesions and potentially avoids unnecessary FNAC/surgery for benign nodules, particularly if integrated with US classification. Elastography is a new technique for evaluating the stiffness of nodules. It is generally recognized that malignant thyroid lesions are harder than benign lesions. A positive electrogram, suggestive for malignancy is more useful in diagnosis than a positive grey-scale ultrasound evaluation.
Elastography increases the specificity of grey scale ultrasound (US), it should be always integrated with its information and should be considered as a complement of conventional ultrasound.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
