
Review Article | DOI: https://doi.org/10.31579/2640-1053/221
*Corresponding Author: Ahmad Reza Rahnemoon. Retired in hematology department, I.U.M.S, Tehran, Iran.
Citation: Ahmad Reza Rahnemoon, (2024), Diagnostic importance of blood and bone marrow study in blood cancers., J Cancer Research and Cellular Therapeutics, 8(8); DOI:10.31579/2640-1053/221
Copyright: © 2024, Ahmad Reza Rahnemoon. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 November 2024 | Accepted: 02 December 2024 | Published: 12 December 2024
Keywords: peripheral blood & bone marrow smears; hematopoietic stem cell; niche; leukemia
We know bone marrow cells have distinctive cytological appearances that reflect the lineage and stage of maturation which these features may be disordered in disease specifically. That’s why, HSC mainly reside in BM and special environment or niche orchestrates HSC fate including their quiescence and proliferation cells in normal and abnormal situations extrinsically. On the one hand, in distinguishing a reactive lymphoid proliferation from a lymphoproliferative disorder requires to lymphocyte morphology for pleomorphic lymphocyte vs. a monomorphic population with a latter favoring a lymphoid malignancy. On the other hand, the clumps of abnormal cells could indicate the infiltration of metastatic tumor. Hence, the manual differentiation is key which means whether a myeloid or lymphoid leukocytosis is favored, the presence of increased blasts should prompt bone marrow examination with providing additional necessary help studies. In this case, along with correct enumeration of blasts and blast equivalent, we should be checked immature granulocytes, basophils and eosinophils as well as distinguishing dysplasia to identify myelodysplastic syndrome or leukemia as well.
The diagnosis of any type of blood cancer depends on comprehension of the whole picture the film presents in peripheral blood smears analyses and/or the red blood cells, leukocytes and platelets which should all be examined. In this regard, Raymond Schofield was the first one of the propose the niche concept for the human hematopoietic system which the hematopoietic stem cells (HSCs) not only reside but may stablish associations with other cells to modulate their behavior. In fact, niches are defined as microenvironments that combine non hematopoietic cells as well as the architecture of the bone marrow (BM) to promote self-renewal and differentiation of HSCs by providing invaluable and essential factors. In other words, HSCs and some of their derived subpopulations are to several stimuli which orchestrate self-renewal, quiescence, migration, differentiation, maturation and survival driving to an adequate hematopoiesis. (3-4,8-9)
We know. there are two core cell lineages in the BM including the common myeloid progenitor line dedicated to erythrocyte/megakaryocyte lineages and to granulocyte/monocyte lineages as well as the common lymphoid progenitor line that ultimately originates the lymphocytes. In this connection, many publications divide the bone marrow geographically into vascular, endosteal and reticular niches and so in the crosstalk between niches and HSC, it is expected how a disturbance of the regulatory and integrating network can lead to/ at least be related into hematological diseases like leukemias.
Some researchers revealed an important point in a sophisticated interaction network between multiple bone marrow cells that regulate different HSC properties like proliferation, differentiation, maturation, localization as well as self-renewal during hemostasis. The various types of BM cells contribute to HSC niche activity and among these are stromal cells closely associated with the vascular as well. The other important point is in the after bone marrow transplantation (BMT), the BM niche is rebuild or completely repaired. Hence, the structure of bone marrow niche must intact, but after the impair of hematopoiesis, could change. Also, due to the malignant transformation of hematopoietic stem/progenitor cells induced by mutation, their normal hematopoietic function is damaged, resulting in deregulated differentiation and cells maturation, also impaired apoptosis and uncontrolled proliferation. So based on the single cell studies conducted on leukemia and in challenging with how single cells are subverted and go to drive into leukemia, so we have a specific focus on these aspects which are including: a) leukemia’s clonal architecture b) malignant hematopoietic microenvironment c) frameworks in supporting structure of the microenvironment to determine leukemia aspects. [2-4,7-9]
But the main question is: what’s the role of leukemic stem cells and its niche during the leukemic disease? In response, BM microenvironment (BMM) run a way regulation of HSCs participated in the transition from HSCs to LSCs. The transformed LSCs not only initiated hematopoietic hemostasis breaking, but also promoted remodeling of the surrounding BMM. For example, in acute myeloid leukemia (AML) accumulating evidence suggested that AML cells reshape a supportive micro-environment to accelerate leukemia progression and suppress the normal hematopoiesis. In this regard, besides providing energy for leukemic cells , the disruption of adipocyte BM niche also impaired endogenous myelo-erythropoiesis. The attention should be paid on identifying the specific self-renewal signaling pathway in LSCs but not shared by normal HSCs. Moreover, some researchers indicated that LSCs could remodel BM niche and the educated BMM provided a protective shelter to promote chemotherapy resistance. [4,8-11]
Leukemias are lethal blood malignancies that are characterized by abnormal clonal proliferation of hematopoietic cells. Due to hematopoietic stem cells (HSCs) malignant transformation, their normal hematopoietic function is damaged, resulting in uncontrolled proliferation, impaired apoptosis and dis-regulated differentiation. For example,1) unexplained cytopenia is an abnormal hematopoietic state characterized by undetermined peripheral blood cell reduction. In better words, the cytopenia is a condition characterized by peripheral cytopenia whose origin is not attributable to cause detectable with conventional tests or to any concomitant diseases with anemia particularly that are often found in older individuals. [1-6]

Fig 1: A- clonality (orange) is common (>50%) in AA when assessed by mutations and other genetic lesions, such as cytogenetic abnormalities, using advanced genomics. AA patients are diagnosed as having MDS when cytopenia is present and clonality is evidenced by MDS-specific cytogenetic abnormalities like monosomy 7, even in the dysplasia absence or increased blast counts (pink circle). B- a parallel relationship is also found in unexplained cytopenia in the general population.
Actually, for older patients with idiopathic aplastic anemia, differential diagnosis includes myelodysplstic syndrome (MDS) that can atypically present in a hypo-cellular form. Moreover, some blasts and overt dysplasia, the presence of chromosomal abnormalities and somatic mutations perhaps revealing. 2)Cytogenetic abnormalities in aplastic anemia (AA) are rare while their incidence increases in hypo-cellular myelodysplastic syndrome (HMDS), in better words, both clonal cytogenetic aberrations and somatic mutations most typically correspond to a clonal myelodysplasia (figure 2) but clonal somatic mutations have been found in AA as well. The other important points are including pelger cells and ring forms and hypo-granularity in neutrophils can be increased in HMDS. Also, there are no univocal abnormalities associated with a precise diagnosis, monosomy 7 and 7q deletion are consistent with MDS rather than severe aplastic anemia (SAA). However, isolated abnormalities of trisomy 8, del(20q), and –Y, are not considered to be sufficient evidence of MDS diagnosis without morphological evidence or increased blast counts, because these isolated lesions may be found in normal individuals and do not likely to correlate with typical MDS pictures.(figures 1 &3) Similarly, without other evidence of MDS, somatic mutations, including those affecting common targets of myeloid malignancies, are not thought to be evidence of malignant clonal evolution by themselves. It is noticeable that, in some AA cases, somatic mutations or other clonality can be compatible with normal or almost normal blood counts. 3) Maturation abnormalities such as giant pro-erythroblast, dysfunctional maturation evidence including nuclear-cytoplasmic asynchrony will suggest specific diagnosis like parvovirus B19 infection in the first instance or MDS or megaloblastic anemia in the second.(11-15)

Fig. 2 : The morphological analyses between AA & HMDS are challenging due to the poor cellularity of the bone marrow. Hence, for indications of clonal evolution in the course of AA are an increased blast percentage, BM cellularity in the presence of recurrent or persistent cytopenia, and the appearance of new cytogenetic or molecular genetic aberrations.
In fact, when BM dysplasia is the only additional finding in unexplained cytopenia(s) cases (neither blast increase nor cytogenetic aberrations) an exact MDS may be challenging specially for younger adults with hypo-cellular BM, with a correct differential diagnosis with other bone marrow failure syndrome (BMFS) must be made. In reality, in pre-leukemia position appear to have an identical clonality of both myeloid and lymphoid compartments. It suggests that the clone can initiate in a very early hematopoietic stem cell. In this case, the mutant genes involve in ineffective dysplastic hematopoiesis pathway. In other words, some driver mutations produce an essential block in differentiation providing a proliferative advantage to the clone cells. Actually, chronic inflammation or exposure to specific environmental stimulus might allow such clones to become dominant. Also, it is noticeable that when a single ancestor cell of the positively expanded clone obtains additional driver mutations, leukemic cells emerge. Likewise, clonal expansion occurs even in tissues that normal apparently. MDS BM findings in the erythrocyte precursors comprise nuclear and cytoplasmic abnormalities. The former consist of budding ,intra-nuclear bridging, more than one nucleus, karyorrhexis or fragmentation, abnormal fine or dense chromatin as well as cytoplasmic abnormalities including vacuolization, ring sidesroblasts. Also abnormal granulopoisis on peripheral blood includes Mas decreased or absent cytoplasmic granules. Dense chromatin clumping in nuclei and many hypo-lobulated that resembling pelger-huet anomaly which all together strongly suggests an underlying MDS [1-9] (figure 3-5).

Fig 3 : MDS morphologic classification based on maturation dysplastic and production ineffective.
Also, in eosinophil and basophil diminished granules possibly and decreased nuclear lobulation. Thrombocytopenia, giant platelets with decreased or absent granules. Micro-megakaryocyte with abnormal nuclei that are multiple and separated widely or even absent or decreased lobulation.
Notably, when the hematopoiesis become abnormal or marked by additional mutations acquisition as well as other additional external factors, the malignancy can appear. Therefore, these points including: a) clonal selection, b) abnormal microenvironment c) mutations acquisition and d) some external additional factors can result in switching from healthy stage to pre- leukemia, MDS or/and leukemia.

Fig. 4 & Fig. 5: Composite image taken from some MDS cases showing dysplastic nuclear features seen in circulating granulocytes and nucleated RBCs which findings in the erythrocyte and granulocyte precursors comprise nuclear and cytoplasmic abnormalities. (Google website)
It is noticeable that in interaction between pre-leukemic cells and its microenvironment, since the pre-leukemia phase is usually clinical silent, but the study of these cells and their characteristics are different which can be the very important point in the disease diagnosis.
In chronic lymphocytic leukemia (CLL), some peripheral blood smears show lymphocytosis and increased smudge cells as a result of the fragility of the CLL cells, namely the blood smear shows an increased number of mature small lymphocytes with a little cytoplasm and dense, clumped chromatin which can produce some smudge cells (figure 6). (16-21)
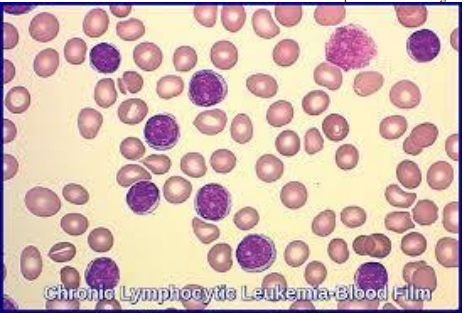
Fig 6: CLL in blood smear including some small mature lymphocyte with condensed, clumpy chromatin, regular nuclear contours and a smudge cell as well. (Google website)
In the CLL pattern, some of them are classic cells which have a small nucleus with a soccer ball chromatin pattern. Also, several cells have increased large cells or pro-lymphocytes with more open chromatin and occasionally punched-out nucleoli. In a variant, CLL with increased pro-lymphocytes a clinically more aggressive disease than CLL which pro-lymphocyte represent 10% to 55% of the lymphocytes. In fact, CLL has many cells being more fragile than normal lymphocytes, disrupt during the smear preparation producing smudge cells in which the cytoplasm is lost and the nucleus spread out or bare nuclei isolated from the broken cells varying from well preserved nuclei without cytoplasm which may be constituted of apoptotic leukocytes dying in circulation representing the auto- suicide of cells in process. We can say, the mechanism is often associated with traumatic disruption of cells primarily during blood film preparation which can be a similar lymphocyte artifacts and it is recommended to include smudge cells in the differential as an absolute count particularly the numbers are increase noticeably. Principally, it was shown that patients in all cancers with the percentage of smudge cell less than 50%had lower mortality rate till when compared with those who had the percentage of smudge cells of 50% or more. (Or it was seemingly that cases with smudge cells of 50% or more had a lower survival rate than those with smudge cells less than 50% in all cancers with follow up at a 2 month interval) which can be an important point in these patients. (15-21)
The cases of chronic myeloid leukemia (CML) characterized by markedly increased myeloid activity resulting in increased numbers of morphologically and functionally normal granulocytes, predominantly comprised of myelocytes and neutrophils.

Fig 7: In the peripheral blood of CML, the immature myeloid cells such as myelocytes are increased.(Google website)
Basophilia can present and sometimes eosinophilia is seen. Thrombocytosis is usually seen. When the disease clinically resembles acute leukemia which means the blast percentage rises further in the context of marrow failure, namely blastic transformation is happened (BP-CML).
In chronic phase(CML-CP) the blood studies typically show mild anemia and leukocytosis that usually exceeds 25x 109 /L primarily comprising neutrophils in maturation various stages particularly increases in myelocytes and neutrophils as well.(figure7) The bone marrow shows hyper-cellularity which CML leukemic stem cells (LSCs) retain the ability to regenerate multi-lineage hematopoiesis and generate a vast expansion of malignant myeloid cells that retain differentiating capacity and displace residual normal hematopoiesis. In the disease progression from an initial CP to advance accelerated phase (AP)(figure 8) to myeloid blast phase ( BC) which can change to AML, or in changing to lymphoid blast phase and eventually transform to ALL( acute lymphoblastic leukemia).(3-7,15-16)

Fig 8 : In the case of CML, there are obviously some immature granulocyte from promyelocyte till neutrophil.( Google website)
The structural and functional disruption in normal BMM which can create changing to the nic.he in proliferation of leukemic blasts and other malignant immature cells while suppressing the proliferation and differentiation of normal HSCs absolutely, namely BMM is significantly altered by leukemic cells for their survival and proliferation (according to BM & PB analyses in the patients) . Actually, this remodeling is a result of the complex interplay between LSC, their BM niche and the treatment outcome. On the other hand, some points are important such as, the changes in the proportion of primitive to mature myeloid cells may reflect response to leukemia treatment or recovery from agranulocytosis. Also, in necrotic areas, the cells stain irregularly with blurred outlines, cytoplasmic shrinkage and nuclear pyknosis which can occur in sickle cell anemia, sometimes in lymphomas, acute lymphoblastic and chronic lymphocytic leukemia. Some other abnormalities like irregular contracted red cells, distorted cells, etc. can be important. Therefore, we should focus a) on mechanisms and structural of BM, b) on the cellular components of BM niche including HSCs , progenitor and precursor cells. However, in some cases such as HMDS and AA, their differentiation and maturation may be difficult without clinical follow-up and repeat BM aspiration or/and its biopsy to demonstrate the transient clonal abnormality nature, because these cases illustrate the challenges of establishing a diagnosis of AA in the hypo-cellular marrow setting with the abnormality of clonal cytogenetic.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
