
Case Report | DOI: https://doi.org/10.31579/2694-0248/001
1Department of Orthopaedics, Kettering Health Network – Grandview Medical Center, 405 W. Grand Ave., Dayton, OH 45405, United States.
2Department of Orthopaedics, Orthopedic Associates of SW Ohio, 7677 Yankee St., Suite 110 Centerville, OH 45459, United States.
*Corresponding Author: Jesse A. Raszewski, Department of Orthopaedics, Kettering Health Network Grandview Medical Center, 405 W. Grand Ave., Dayton, OH 45405, United States.
Citation: Jesse A. Raszewski, H. Brent Bamberger (2019) Case Report of Diagnostic Evidence Depicting Palmaris Longus Origin Reversal: Ultrasound and MRI Evaluation. Clinical Orthopaedics and Trauma Care. 1(1); DOI:10.31579/2694-0248/001
Copyright: ©2019 Jesse A. Raszewski, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 November 2019 | Accepted: 19 November 2019 | Published: 30 November 2019
Keywords: palmaris longus; anatomic variant; forearm musculature; forearm flexor.
Introduction: The palmaris longus (PL) is very prone to anatomical variance. It may exhibit agenesis, reversal, and duplication. The reversal variant presents with the PL tendinous aspect proximally and the muscle belly distally. It is an important finding, and it is important to consider when making a differential diagnosis. This is the only reported case of a left distal forearm PL muscle variant with ultrasound and magnetic resonance imaging (MRI) in a Caucasian adult male.
Case Report: A 28-year-old Caucasian male presented to the clinic with an abnormal ultrasound finding of a left wrist mass. The patient was instructed to get an MRI, which demonstrated and further confirmed the reversed PL muscle.
Conclusion: Although rare, anatomic muscle variance may occur in many places of the body leading to symptoms that need attention. These variants should be considered in orthopedic differential diagnosis and ruled out appropriately with proper diagnostic techniques. By making the correct diagnosis, it leads to improved patient outcomes and satisfaction both conservatively and surgically.
There are many cases of anatomical variance in the musculature of the upper extremity (UE). The fusiform palmaris longus (PL) muscle is prone to variance, and in order of prevalence; the completely absent is the most common, followed by the reverse, duplicated, bifid or hypertrophied form [1]. Opposite to normal anatomy, the reversed PL exhibits a proximal tendinous structure and a muscle belly distally [1]. A recent meta-analysis from 1975 to 2014 reported that there is only one medical record of magnetic resonance imaging (MRI) displaying the reversed PL [2]. The present report describes a case of a reversed PL diagnosed with ultrasound and MRI, with a literature review to demonstrate the vast spectrum of variation seen in the musculature of the UE.
Case Report
A right hand dominant, 28-year-old Caucasian male presented to the orthopedic associates of Southwest Ohio as a referral to a hand specialist due to an abnormal ultrasound finding and left wrist mass. The ultrasound of the suspected left wrist mass was executed 10 days prior, exhibiting increased echogenicity within the musculature of the left distal wrist at the site of the patient’s reported abnormality. This echogenicity was asymmetric when compared to the right wrist. The image of the left anterior distal forearm on ultrasound is displayed in Figure. 1.
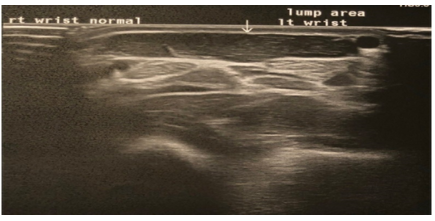
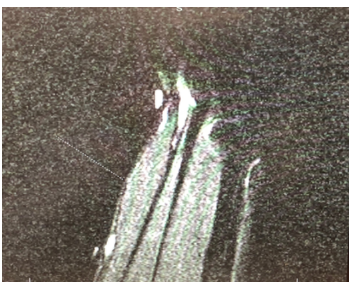
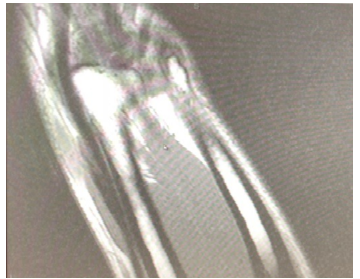
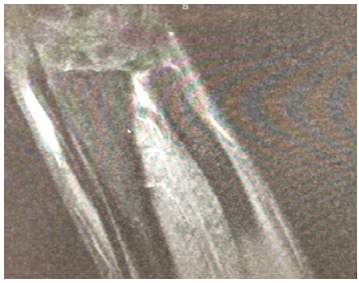
There was no evidence of a focal mass or fluid collection according to the ultrasound report. The patient presented complaining of left wrist swelling, with no pain. There was an unremarkable past medical, surgical, or family history significant to the chief complaint. As far as a differential, the questionable echogenicity within the musculature of the left distal forearm could have been related to a mild non-specific myositis. Moreover, there was no evidence of focal mass or fluid collection, so an MRI was considered to rule out a neoplasm.The patient completed the MRI in 10 days, and then followed up in a week to the clinic. The current status of the patient remained unchanged. The MRI of the patient demonstrated a palpable abnormality secondary to a congenital variation consisting of a PL muscle variant due to an accessory muscle belly volar to the flexor tendons. The signal intensity of this muscle appears within normal limits. This finding was confirmed on the retrospective review of the prior ultrasound. The abnormal muscle variant is displayed in the sagittal view T1 MRI in (Figure. 2), it is displayed in the coronal view T1 MRI in Figure.3, and it is displayed in the coronal view T2 MRI in Figure.
After consecutive diagnostic imaging techniques ruled out anything pathologic including neoplasm, the patient was counseled on the plan. Since the muscle variant was not painful and it did not limit functional outcomes, a non-operative conservative plan was instituted. The patient was informed to follow-up as needed, and if any concerning symptoms arose to schedule an appointment and new measures would be taken for continued care.
In the present case, the PL muscle belly originated at the distal forearm volar to the flexor digitorum profundus and superficialis tendons. The abnormality lied between the soft tissue markers placed at the site of the patient’s complaint of the palpable abnormality.
The standard anatomical origin of the PL is located on the medial epicondyle at the common flexor tendon, and the insertion is the palmar aponeurosis located volarly to the flexor retinaculum [1]. The PL tendon and the palmar aponeurosis are described as two separate entities based on their origin and development [3]. Neurovascularly, it is supplied by branches of the ulnar artery and innervated by branches of the median nerve [4].
This patient is a 28-year-old Caucasian male that presented with a left distal forearm PL muscle variant. Reimann et al. conducted the first major study that looked at 1600 UEs and the incidenc of PL variations, and it showed that there were only three aberrancies of the attachment of the muscle in the 540 consecutive arms [5]. Moreover, Olewnik et al. created a classification system that described nine different types of anatomical presentations of the PL [6]. The patient’s abnormality presented with the muscle belly distally and tendinous portion proximally, which is described as the Type VI variant and is only identified in 2% of cases [6].
The clinical significance of this case is placed on the nervous systems implications. Proximal muscle belly PL variants may predispose patients to median nerve compression [6]. Although it is much less common, compression of the ulnar nerve in Guyon’s canal has been reported as well [7]. Patients may also present with distal forearm edema and inflammation that may result in reduction of hand function due to wrist flexion movements [8].
It is important to understand anatomical variants of the PL and to incorporate into the differential diagnosis list because it plays a crucial role in reconstructive surgeries [9]. It is essential to clinically examine patients that present with an anterior distal forearm mass with suitable diagnostic techniques to avoid inappropriate surgical procedures.
Conclusion
This is a case report of a patient exhibiting symptoms from the reversed PL muscle in the forearm. Anatomical muscle variants should be considered in a differential diagnosis when there is an unknown muscular mass in a patient. Due to the minimal number of case reports on anatomical muscle variation, we suggest that with appropriate diagnostic techniques and proper management of such cases, it can lead to improved patient outcomes and satisfaction.
Clinical Message
With appropriate history and diagnostic techniques, considering anatomic muscle variants in your differential diagnosis can lead to improved patient outcomes and satisfaction.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
