
Research Article | DOI: https://doi.org/10.31579/2641-0419/264
1 Republican Specialized Scientific and practical medical Center of Surgery named after academician V.Vakhidov.
2 Bukhara State medical institute after named Abu Ali ibn Sino.
*Corresponding Author: Abdumadjidov H. A, Professor of the department of the Surgical disease and reanimation.
Citation: Abdumadjidov H.A., Buranov H.J., Saidkhanov B.A., Isomitdinov B.Sh. (2022). Diagnostic and Surgical Treatment of Multi-Valve Heart Disease with Infective Endocarditis. J. Clinical Cardiology and Cardiovascular Interventions, 5(7); DOI:10.31579/2641-0419/264
Copyright: © 2022 Abdumadjidov H. A, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 April 2022 | Accepted: 13 June 2022 | Published: 20 June 2022
Keywords: multi-valve acquired heart diseases, complications of infective endocarditis
" Diagnostic and surgical treatment of multi-valve heart disease with infective endocarditis"
Objective: The aim of the study was to analyze our own experience of diagnosis, choice of tactics and execution of multi-valve surgical correction of heart defects in infective endocarditis (IE).
Methods: We retrospectively analyzed data and clinical results of 156 patients with infective endocarditis who underwent the cardiac surgery in our clinic. Among them, 85 were men (56.5%), and women - 71 (45.5%). Age of our patients ranged from 12 to 68 (mean 32.76 (1.6)) years. The patients were divided into 2 groups: group 1, 89 (57.4%) patients who underwent a complex of developed by the author’s antibiotic therapy, surgical treatment and preventive measures and 2-group 67 (42.6%) patients who underwent the traditional surgical treatment scheme. We analyzed electrocardiography, chest X-Ray, transthoracic echocardiography, transesophageal echocardiography, cardiac catheterization and coronary angiography and blood culture analysis.
Results: Intraoperative treatment - preventive measures (TPM) were as follows; mechanical and chemical sanitation of the infected area of the heart; implantation of valves with antibacterial properties; hyperthermic perfusion; antimicrobial therapy, including anti-fungal agents. Application of the above measures reduced mortality in the study group to 5.1%, in the control group - 9.3%. In dynamics, mortality declined to 3.9% in the study group.
Conclusion: Our results of surgical treatment of multi-valve heart defects with infective endocarditis showed the efficacy of developed complex preoperative and intraoperative measures in surgical treatment of IE. This new treatment approach is associated with significant improvement of left ventricular function and low mortality rate.
Infective endocarditis (IE) is common etiological factor in the development of multi-valve heart lesions and has a number of special features in the definition of diagnosis, surgical tactics and postoperative management [1; 2; 3; 4].
Infective endocarditis is a rare, life-threatening disease which may affect heart valves, mural endocardium and cause acute valvular insufficiency and systemic embolic events. It is caused by pathogenic or opportunistic microflora. In the setting of bacteraemia with a pathogenic organism, an infected vegetation may form as the end result of complex interactions between invading microorganisms and the host immune system. Vegetation is composed from fibrin overlay, blood clots, blood cells, damaged heart tissue and microorganisms. According to the last data, the incidence of the infective endocarditis in Russian Federation is about 2 - 6.5 cases to 100,000 population [1]. According to various authors, up to 18% of patients are adults aged from 20 to 50 years [3]. Unfortunately, attempts to treat IE through conservative treatment were unsuccessful. Nowadays, the effectiveness of
surgical treatment over medical treatment is obviously clear. V.P. Polyakov reported that mortality rate in patients who got only conservative treatment was 50 - 90% [5]. R.A. Nishimura claimed that, good early and long-term results of surgical treatment of multi-valve infective endocarditis is clearly depend on the correct definition of surgical tactics. In time and prompt surgical decision will reduce mortality up to 11,2% [4, 10]. In this article, we would like to share and discuss own experiences in diagnostic strategies, management and correct choice of surgical tactics in the treatment of IE with multi-valve lesions.
Statistical analysis of the result was carried out using Microsoft Office Excel 2007 with Statistical Version 6.0 package. Continuous variables are presented as mean and standard error, and categorical data as percentages. Comparison of continuous variables between groups was performed using parametric Student’s (t) test and Chi-square test was used for comparison of categorical variables. The degree of accuracy was determined at the level of significance p<0>
The retrospective material of our research is based on 196 patients who underwent surgery in our hospital from 2014 to 2019 yy for IE with multi-valve lesions. The age of our patients ranged from 12 to 71 (mean 32.76 ± 1.6) years, 105 were men (54.5%), and 91 were woman (45.5%), respectively. In diagnosis, we used the classification criteria of Durack D.T. (2004).
The patients were divided into 2 groups: group 1 consists of 112 (57.4%) patients who got preventive measures, antibacterial and surgical treatment. 2-nd group consists of 84 (42.6%) patients who underwent the traditional scheme of prevention and surgical treatment.
Taking in account the following features valve infective endocarditis (IE):
• High frequency of systemic embolism
• High mortality in the treatment of infective endocarditis (IE)
• The dilemma of the optimal operation period
• Imperfect system of prevention
• Aspects of the antimicrobial therapy
In order to solve these tasks, we developed own comprehensive measures for the prevention and treatment of IE:
1. The elimination of source of infection
2. Correction of hemodynamics.
3. Reliable fixation of the prosthesis
4. Prevention of relapse of IE
Clinical examinations.
All patients are examined by standard protocol: general clinical tests, electrocardiography (ECG),
chest X-ray
, transthoracic echocardiography (TTE) was performed in 40.5% of patients;
coronary angiography and heart catheterization was performed in
12.65% of patients; sampling of blood culture in 38.6% of patients, histology with light electron microscopy (SEM) in 47.5% of patients, respectively. Surgical treatment consisted of an "open" correction of affected valves, with performing complex measures to eliminate intracardiac source of infection and prevention of postoperative septic complications. All patients underwent surgery with cardiopulmonary bypass (CPB) and cardioplegia (CP).
The surgical treatment of multivalvular heart disease associated with infective endocarditis is still challenging. Application of updated by our department complex of medical, surgical and preventive measures aimed to improve the immediate and long-term results of our operations.
The etiology of infective endocarditis associated with valvular heart disease in our patients included rheumatic heart valve disease in 62% of patients, infective endocarditis – 16%, degenerative valvular disease – 13%, and congenital heart disease in 9% of patients, respectively. Interestingly, there were no patients with addiction and substance use.
Types of operations performed in our patients are provided in Table 1. The most commonly performed surgery was mitral valve replacement (MVR) plus aortic valve replacement (AVR) with tricuspid valve (TV) repair. Other types of operations included: mitral valve (MV) repair, aortic valve replacement (AVR), tricuspid valve open commissurotomy (OTC), tricuspid valve replacement (TVR) and mitral valve replacement (MVR). We also used left atrial thrombectomy of in combination with other types of surgery.
Name the Transactions | Number of | Percent |
| MVR+AVR with Pl TC | 98 | 50% |
| TV repair, MV repair, AV repair | 32 | 16.3% |
| MVR with TV repair and AV repair | 26 | 13.3% |
| AVR with TV repair and AV repair | 9 | 4.6% |
| MVR with TV repair | 7 | 3.8% |
| MVR+AVR with OTC | 5 | 2.5% |
| MVR, TVR, AVR | 3 | 1.5% |
| MVR, TVR | 3 | 1.5% |
| Other operations | 13 | 6.6% |
* AV - aortic valve, AVR –aortic valve replacement, MV – mitral valve, MVR - mitral valve replacement, OTC - open tricuspid commissurotomy, TV – tricuspid valve, TVR - tricuspid valve replacement
Table 1: The types of operations performed in patients with multi-valve heart defects with infective endocarditis
Intraoperative treatment and preventative measures were as follows:
1. Mechanical and chemical sanitation of infected heart area
2. Use of antibiotic coated prosthetic heart valve sewing cuffs
3. Hyperthermic Perfusion
4. The antimicrobial therapy, including anti-fungal agents.
Use of specially produced artificial mechanical heart valves can prevent further development or activation of the infection. Antibiotic cuff impregnated in artificial prosthesis retains its activity for 2 weeks, which reduces the recurrence of IE [8]. In addition, we used hyperthermic perfusion in these patients, targeting micro- and macro-organisms, as following: keeping temperature within 38.5-39˚ C for 15-20 min after removal of aortic clamp. This, results in "impact on the macro-organism": restoring the patient immunobiological properties [7]; and "the impact on the micro-organism" - intensifying pathogen metabolism and enhancing effectiveness of antibiotics [6].
Microorganisms | Frequency allocation,% |
Gram (-) negative bacillus | 8,8 |
Gram (+) positive bacillus | 2,5 |
Staphylococcus aureus | 7 |
Pseudomonas aeruginosa | 6,3 |
St.epidermidis | 5 |
5 | |
Klebsiella pneumoniae in total | 4 38,6 |
Table 2: Microbiological examination
Laboratory and microbiological tests are of particular importance to guide antibioticotherapy. Table 2 shows the results of microbiological tests, where in contrast to literature data: in 5% of all patients, we identified fungal lesions of the heart valves - Candida spp. The blood culture was positive in 39.1% of patients, in 8.8% of the cases we detected multidrug-resistant Gram-negative flora, in 7% - Staphylococus aureus, and in 6.3% of cases - Pseudomonas aeruginosa. In remaining 60.9% of patients, the blood culture was negative due to wide-spectrum antibiotic therapy used on pre-hospital state. According to above-mentioned results, we used antifungal therapy in addition to antibiotics.
Echocardiography had a particular importance in adequate definition and choice of surgical tactics for our patients. Transthoracic 2-dimensional and Doppler echocardiography data in addition to the clinical criteria were the basis of indications for surgical correction of multi-valvular defects with IE, preoperative echocardiography data are presented in Table 3. Surgical tactics of the operation were identified taking in account the peculiarities of defect anatomy, disease complications, and presence of comorbidities. At intraoperative stage TEE was carried out aiming at refining the tactics of surgical correction and evaluation of the adequacy of the operation.
Options LV | group I | group II | Overall | Meaning Р1-2 |
М+m | М+m | М+m | ||
EDD (ml) | 5,88+0,15 | 6,16+0,18 | 6,01+0,12 | >0,05 |
EDV (ml) | 181,8+9,81 | 194,55+13,4 | 187,3+8,01 | >0,05 |
ESD (ml) | 3,88+0,12 | 7,05+1,65 | 5,3+0,76 | <0> |
ESV (ml) | 83,64+12,1 | 81,86+6,82 | 82,8+7,44 | >0,05 |
SV (ml) | 111,24+5,9 | 116,45+7,5 | 113,5+4,69 | >0,05 |
EF (%) | 63,21+1,96 | 60,3+1,19 | 61,83+1,23 | <0> |
*LV–left ventricle, EDD – end-diastolic dimension, EDV – end-diastolic volume, ESD – end –systolic dimension, ESV – end systolic volume, SV-stroke volume, EF-ejection fraction
Table 3: Clinical characteristics of patients according to the TT echocardiography preoperatively
Indication for surgical treatment in our patients, in most cases, was progressive heart failure. At the same time, we are sure that lower inflammatory activity may be achieved using a complex of medical and antibiotic therapy. The combination of the preoperative preparation, using the updated therapeutic and preventive measures, subsequently, was the basis to decrease mortality in the short and long periods of observation.
Indications for surgery | Number | percent |
Progressive heart failure | 120 | (61,3%) |
The ineffectiveness of antibiotic therapy | 25 | (12,7%) |
floating vegetation | 17 | (8,7%) |
Embolism | 21 | (10,7%) |
abscess | 13 | (6,6%) |
Total operated | 196 | (100%) |
Table 4: Indications for the implementation of multi-valve defect surgery with infective endocarditis
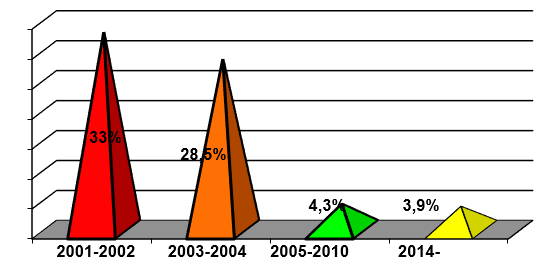
Analysis of the nearest results of our operations in the two groups showed mortality rate of 5.1% in the first group, and 9.3% in the second group. Thus, the overall hospital mortality was 6.9%. With the development of diagnostic criteria for multi-valve defect with IE, choosing the right surgical technique and the use of therapeutic and preventive measures developed in the department, we managed to reduce the rate of hospital mortality and improve cardiac function. We observed in a 3-year follow-up period reduction of cardiac chambers and volumes size (Table 5) and significant reduction of hospital mortality, as compared with previous years (from 33% in 2000-2002 to 3.9% in 2014-2019 periods) (Diagram №1).
Dynamics echocardiographic parameters (p<0>
Diagram :1 Dynamics of hospital mortality data
| Echocardiographic data | The periods of observation | ||
I-group | Before surgery | At discharge | 3 years later |
EDD (ml) | 5,88+0,15 | 5,03+0,13 | 4,65+0,16 |
EDV (ml) | 181,8+9,81 | 133,63+8,12 | 105,4+7,43 |
ESD (ml) | 3,88+0,12 | 3,67+0,11 | 3,3+0,21 |
ESV (ml) | 83,64+12,12 | 67,58+6,56 | 45,4+5,76 |
SV (ml) | 111,24+5,97 | 65,8+2,97 | 60,01+3,32 |
EF (%) | 63,21+1,96 | 51,05+1,48 | 61,45+2,5 |
Р II-group | <0> | ||
EDD (ml) | 6,16+0,18 | 5,34+0,17 | 5,14+0,15 |
EDV (ml) | 194,5+13,39 | 147,13+11,21 | 125,71+8,07 |
ESD (ml) | 5,25+1,01 | 5,1+1,22 | 3,3+0,21 |
ESV (ml) | 81,86+6,82 | 73,16+7,05 | 47,93+5,91 |
SV (ml) | 116,45+7,55 | 73,63+4,95 | 77,6+6,06 |
EF (%) | 60,0+1,19 | 52,34+1,57 | 58,36+3,16 |
Р | <0> | ||
Table 5: Follow-up echocardiography data
*LV – left ventricle,
EDD – end-diastolic dimension,
EDV – end-diastolic volume
ESD – end –systolic dimension
ESV – end –systolic volume
SV –stroke volume
EF – ejection fraction
Our study has certain limitations as being retrospective in design and relatively small numbers of patients. Further prospective studies need to be undertaken to clarify the usefulness of our approach of treatment of IE associated with multi-valvular heart defects.
Our results of surgical treatment of multi-valve heart defects with IE showed the efficacy of updated complex preoperative and intraoperative measures in surgical treatment of IE. Morphological studies found that during the formation of microbial vegetation, in 41.7
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
