
Review Article | DOI: https://doi.org/10.31579/2578-8965/195
Family Physician & Public Health Consultant Bengaluru. India
*Corresponding Author: Suresh K, Family Physician & Public Health Consultant Bengaluru.
Citation: Suresh K, (2023), Diagnostic and Management Challenges of Endometrial Tumours in Developing Countries! J. Obstetrics Gynecology and Reproductive Sciences, 7(7) DOI:10.31579/2578-8965/195
Copyright: © 2023, Suresh K. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 October 2023 | Accepted: 08 November 2023 | Published: 16 November 2023
Keywords: gynaecological malignancies; cross‐disease analysis; endometrial cancer; endometriosis; genome‐wide association study; genetic correlation; role of obesity; party
Gynaecological cancers are among the most common cancers in women and hence an important public health issue in very country. Ovarian, Cervical, and Endometrial cancers contribute the most of Gynaecological cancers in India and worldwide. Endometrial benign tumours like Endometrioid cystadenoma / adenofibroma with endometrioid type glands, associated with endometriosis pose challenges of diagnosis.
Endometrial cancer (EC) is the most common gynaecological malignancy in the West, but in India, the incidence rates are low. National cancer registry project (NCRP) estimated 27,922 cases of EC in 2022 in India. The possible association between cancer and endometriosis varies according to the histologic subtype of ovarian cancer and is focused mostly on endometroid and clear-cell ovarian cancer subtypes.
The only way to diagnose womb cancer for sure is to take a sample of the tissue lining the womb (biopsy) and get histopathology report. However, most of the literate and urban women with ECs present at an early stage due to menorrhagia, abdominal pain or abdominal distension and are associated with a good prognosis. But the situation in rural India is one of lack of diagnostic and management facilities in public sector even at most of the district level. Treatment for endometrial cancer usually involves a hysterectomy, and adjuvant radiotherapy and/or chemotherapy. Surgery sometimes may include the removal of uterus and the fallopian tubes and ovaries, called a Hysterectomy with salpingo-oophorectomy. Adjuvant Radio/Chemotherapy treatment is planned based on final surgical &pathological staging.
Due to the lack of cancer awareness, variable pathology, and dearth of proper screening facilities in most developing countries including India, most rural women report at advanced stages, adversely affecting the prognosis and clinical outcomes.
Materials and Methods: This article is based on a case of adenocarcinoma Stage 1, Type 2 and another case of Endometrioid Cyst clinically and radiologically suspected to be malignant, but histopathology of tissues tested branded it as Endometrioid Cyst Adenofibroma. Relevant literature review of global experiences and good practices of management of endometrial cancers are added.
About five lakh women develop Gynaecological Cancers worldwide every year and more than one lakh new patients are diagnosed in India itself. Gynaecological cancer is defined as uncontrolled growth and spread of abnormal cells that originate from the reproductive organs like uterus, fallopian tubes, and ovaries. Gynaecological cancers are among the most common cancers in women and hence an important public health issue. Due to the lack of cancer awareness, variable pathology, and dearth of proper screening facilities in most developing countries including India, most women (except for urban literate women) report at advanced stages, adversely affecting the prognosis and clinical outcomes. Ovarian, Cervical, and Endometrial cancers contribute the most of Gynaecological cancers in India and worldwide [1,2,3,4,5]. Ovarian cancer (OC) has emerged as one of the most common malignancies affecting women in worldwide and India and has shown an increase in the incidence rates over the years. Ovary cancer (OC) is one of the most common lethal and aggressive gynaecologic cancers. It still is amongst the commoner cancers in India and a leading cause of cancer-related deaths in women [12]. The traditional treatment of OC involves resecting all suspected organs followed by chemotherapy. Cervical cancer (CC) is the second most common cancers of women in India, despite being largely preventable and national Cervical cancer (CC) detection campaigns promoted by GOI. However, cervical cancer is on a declining trend, though it remains the second most common cancer in women after breast cancer [12]. Among 604,100 new cases of CC and 341,831 deaths due to this malignancy detected globally in 2020, India, accounted for 9.4% of all cancers and 18.3% (123,907) of new cases in 2020. The age-standardized incidence rate of cervical cancer decreased substantially by about 40
1.A case of Uterine endometrial Adenocarcinoma:
Roopa aged 56 years, sought a gynaecologist’s consultation for heavy Bleeding per vagina for 6 months, who referred her to a private Oncology Hospital in Mysuru, Karnataka on 18 October 2023. She has a married life of 30 years and has a daughter aged about 26 years. She attained menopause since 2012. Her general condition was fair, but BMI was 32. An USG abdomen with transvaginal Scan done on 16/10 23 showed Bulky Uterus with thickened endogenic endometrium with cystic spaces suggestive of endometrial hyperplasia. CT Scan done of the abdomen prior to coming to this hospital reported to be normal. Her basic investigations included: Hb%=12g/Dl, Urea = 30 mg/Dl, Creatinine= 4.4 mg/dl, Sodium =140 mEq /l, Potassium=4.4 mEq/dl, Chlorine=120 mEq/dl, Total WBC count 10.400/Cu mm, Neutrophils= 86%, Lymphocytes = 12%, Eosinophils=2% and Platelet count+2.41,000/cu mm. 2 D echo reported heart, functions as normal with mild Mitral Regurgitation with 60
Gynaecological cancers are among the most common cancers in women, difficult to diagnose and treat for want of diagnostic facilities in most developing countries. The drudgery of women due to this disease is more due to social stigma as most poor and illiterate women consider the symptoms as normal of aging and delay seeking care despite being almost curable in early stages. Therefore, it is of an utmost public health important issue in very country. Endometrial cancer is common in western women, and the rates are very high probably due to care seeking behaviour and diagnostic facilities. However, in India, the rates are as low as 4.3 per 100,000 adult and elderly women.
Increasing age is the first and most important risk factor as for most cancers. Other risk factors for endometrial cancer include Hormone therapy, Postmenopausal Oestrogenic therapy, Selective oestrogen receptor modifiers, Tamoxifen therapy, Obesity, Metabolic syndrome, Diabetes, Nulliparity, Early menarche or late menopause, Polycystic ovary syndrome, Family history/genetic predisposition, Mother, sister, or daughter with uterine cancer, Lynch syndrome and Endometrial hyperplasia [3].
There are hardly any community-based studies to define incidence or prevalence. A hospital-based study from Mumbai, reported that the endometrial cancer patients with localized disease at diagnosis had a good outcome in India, as the proportions of patients dying above 50 years of age, non-residents and illiterates was higher than their counterparts. Only about half (54.8%) of patients had some form of treatment before attending the hospital. The contribution of tobacco-chewers (4.2%) and family history of cancer (6.1%) was small. Whereas, among the patients a quarter (25.8%) had 3-5 pregnancies (gravida), Nulliparous to Gravidae 1 or 2 were 36.1%, and 38.1% did not even remember the pregnancy history correctly. The 5-year overall survival rate was 92%, which also indicated better prognosis for those aged less than 50 years (97%), with localized disease (93%) and those treated with surgery either alone or as a combination with hormones (95%). [5].
Endometriosis Associated Cancers and Genes Involved:
A review of the literature suggested a link between endometriosis and ovarian and Uterine cancers, but not breast and cervical cancer. Women with endometriosis appear to be more
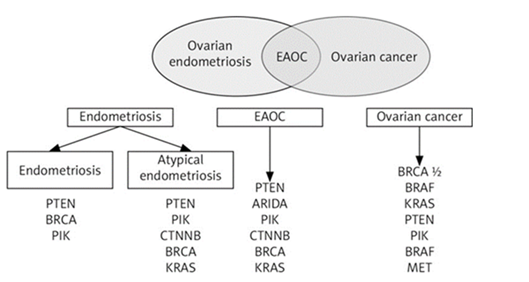
likely to develop, non-Hodgkin’s lymphoma, and brain tumours cancers. Some case reports, indicate the complexity of the endometriosis-cancer relationship. A case of primary endometrioid carcinoma arising from deep infiltrating endometriosis 6 years after diagnosis of ovarian cancer is reported. Somatic mutations of PIK3CA, PTEN, and ARID1A might play a role in the disease progression and malignant transformation. At present, not
a single marker is recommended for diagnosis, or treatment. The issue of how to identify which endometriosis patients develop ovarian cancer remains critical but unanswered [10,11].
The likelihood of developing endometrial polyps and uterine fibroids is higher among postmenopausal women with proliferative endometrium, according to a study published in the December 2023 issue of the journal Maturitas [20].
A cross-sectional study of all women with a tissue-proven diagnosis of endometriosis postoperatively in a tertiary care hospital over a decade between January 1, 2010, and December 31, 2019, reported that out of 800 patients, 104 (13.0%) were found to have coexistent malignancy. Among 104 total cancer cases i) ovarian cancer contributed 50, (6.2%); ii) endometrial cancers 33, (4.1%); iii) synchronous ovarian, endometrial 7, (0.9%); and breast cnacers-14, (1.8%). Postmenopausal status (Odds Ratio-OR= 6.2), duration of endometriosis over 5 years (OR 4.7), and endometriomas larger than 8 cm, increasing age over 50 years (OR 1.13), higher levels of cancer antigen 125 (CA 125 -OR 1.002), were inferred as predictive of coexistent malignancy [6].
A study of a total of 1808 postmenopausal women who underwent endometrial biopsy between January 1997 and December 2008 and followed-up for a comparable duration of 11.9 vs. 11.5 years, respectively., indicated that Endometrial polyps developed twice more often in women with proliferative endometrium (17.3%) as compared to women 9.7% in women with atrophic endometrium (9.7%). On multivariable analysis, 62.1% of women with
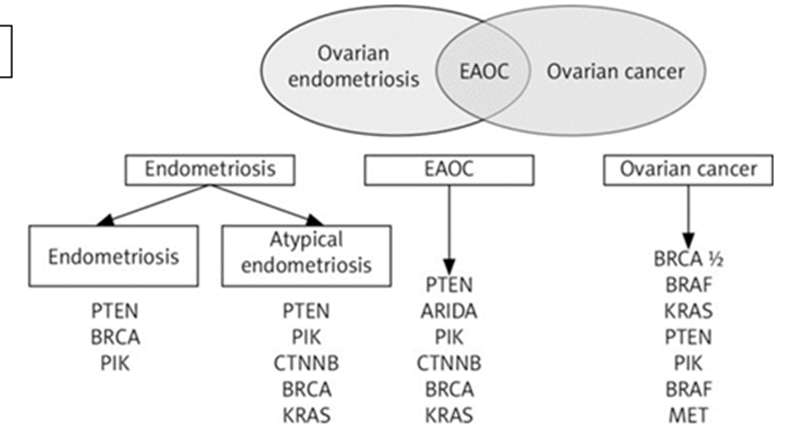
Figure:1 proliferative
endometrium were found to have fibroids on ultrasound compared to 50.3% of women with atrophic endometrium. The risk of endometrial polyps was 2-folds higher among women with proliferative endometrium with adjusted odds ratio (OR) of 1.9. The need for repeat endometrial biopsy was 34.9% in women with proliferative endometrium vs 16.8% in those with atrophic endometrium. Nearly a quarter (26.6%) of women in the proliferative endometrium group required hysterectomy or hysteroscopy as against 16.2% in the atrophic endometrium group. The study inferred that women with proliferative endometrium are at higher risk of malignancy, endometrial polyps, and uterine fibroids. Therefore, the authors recommend medical management to reduce estrogenic activity and associated risks in postmenopausal women with proliferative endometrium [10,11].
Pathological types: Endometrioid cystadenoma / adenofibroma are benign tumours with endometrioid type glands, associated with endometriosis, which is represented by our Pratim’s case, that needs to be differentiated with endometrial cancers only by a pathophysiologic perspective. Endometrial carcinomas have been traditionally divided into 2 types: Type 1: includes endometrioid and mucinous carcinoma and Type 2: includes serous, clear cell, undifferentiated carcinoma and carcinosarcoma. Endometrioid histotype constitutes approximately 80% of all endometrial carcinomas, most of which are low grade (FIGO grade 1 - 2), as was our Case of Roopa was one such report [13]. Surgical treatment for both conditions remains basically the same.
Type 1: These lesions are associated with long term elevated oestrogen levels, which lead to persistent proliferative stimulation of the endometrium. Risk factors leading to hypoestrogenism include obesity, exogenous hormonal therapy (e.g., tamoxifen use for breast cancer), ovarian cortical hyperplasia / hyperthecosis, polycystic ovarian syndrome and hormone producing tumours (e.g., granulosa cell tumour of the ovary). Among others PTEN, ARID1A, PIK3CA, KRAS gene alterations are common. Atypical endometrial hyperplasia / endometrioid intraepithelial neoplasia is regarded as the precursor lesion [2,3,4].
Type 2: These tumours have a lesser association with unopposed oestrogen exposure. Serous carcinoma is characterized by early alterations in TP53. Precursor lesion for clear cell carcinoma has not been identified yet but are faster growing and more likely to spread [10].
Sites involved: Most common site is the uterine corpus - endometrium, endometrial polyps or adenomyosis. Primary cervical endometrioid adenocarcinomas are extraordinarily rare and likely develop from cervical endometriosis. Drop metastasis or contiguous extension from corpus should be ruled out in these cases. Technically, any tissue involved.
All endometrial cancers must perform a complete molecular classification (POLE mut, MMRd, NSMP, p53abn) says the FIGO report of June 2023.
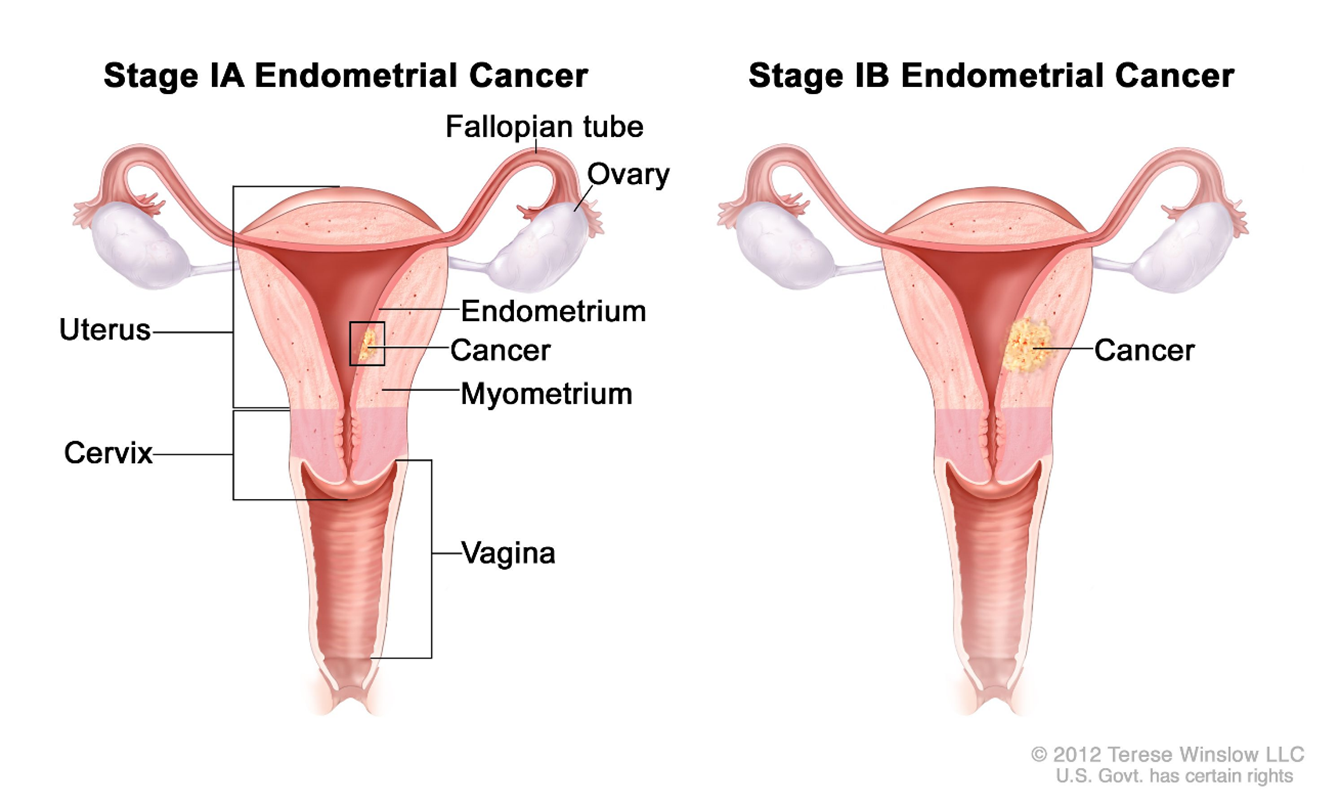
Figure 2: FIGO classification Illustrated:
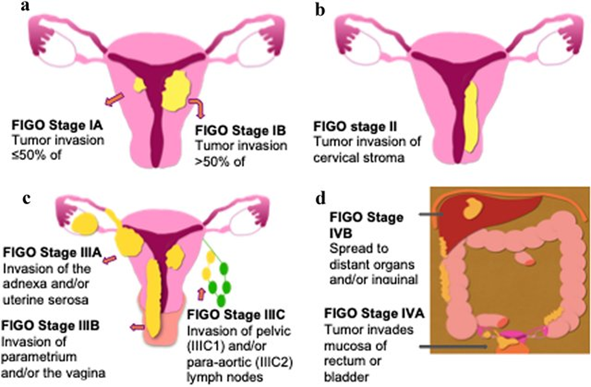
Figure 3: Illustrated FIGO staging system for endometrial Cancer!

Treatment:
Apart from the standard treatment practices for decade listed above Immune checkpoint inhibitors, a type of immunotherapy, have shown promising outcomes in treating tumours that have defects in a specific DNA repair process, called mismatch repair [17].
On July 31, 2023, the Food and Drug Administration approved Dostarlimab-gxly (Jemperli, GlaxoSmithKline) with carboplatin and paclitaxel, followed by single-agent dostarlimab-gxly, for primary advanced or recurrent endometrial cancer (EC) that is mismatch repair deficient (dMMR), as determined by an FDA-approved test. JEMPERLI injection can be imported by patients or government hospitals only in the name of the patients.
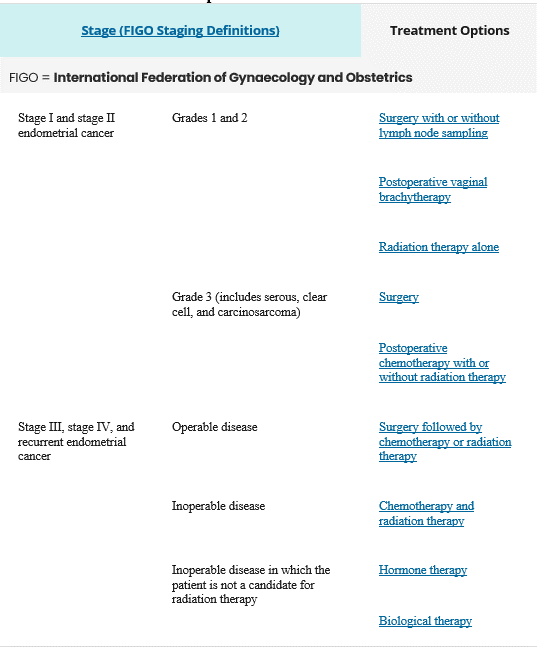
Source: Endometrial Cancer Treatment -Health Professional Version, https://www.cancer.gov/
Treatment Options for Endometrial Cancer
Endometriosis is a chronic disease associated with severe, life-impacting pain during periods, sexual intercourse, bowel movements and/or urination, chronic pelvic pain, abdominal bloating, nausea, fatigue, and sometimes depression, anxiety, and infertility.
It affects roughly 10% (250 million) of reproductive age women and girls globally. In India endometriosis is estimated to bother about 42 million women in their lifetime.
Epidemiological, biological, and molecular data suggest links between endometriosis and endometrial cancer, with recent epidemiological studies providing evidence for an association between a previous diagnosis of endometriosis and risk of endometrial cancer.
Using the proteomics approach, anti-endometrial antibodies (AEAs - tropomyosin 3 (TPM3), stomatin-like protein2 (SLP-2), and tropomodulin 3 (TMOD3)] were detected in Indian women with endometriosis.
From a pathophysiologic perspective, endometrial carcinomas have been traditionally divided into 2 types: Type 1: includes endometrioid and mucinous carcinoma and Type 2: includes serous, clear cell, undifferentiated carcinoma and carcinosarcoma. Endometrioid histotype constitutes approximately 80% of all endometrial carcinomas, most of which are low grade.
The only way to diagnose womb cancer for sure is to take a sample of the tissue lining the womb (biopsy) and get histopathology report.
Treatment for endometrial cancer usually involves a hysterectomy, salpingo-oopherectomy and adjuvant radiotherapy and/or chemotherapy.
Immune checkpoint inhibitors, a type of immunotherapy, have shown promise in tumours that have defects in a specific DNA repair process, called mismatch repair.
Therefore, all endometriosis cases must be subjected to frozen section endometrial biopsy and the extent of surgery be based on the histopathology, report.
Main challenges for improving EC management include early diagnosis, risk stratification, control of recurrent disease, or more appropriate therapeutic strategies integrating mutational profiles.
Given the public health importance the national and provincial governments must strive to make the diagnostic and treatment facilities in rural areas of developing countries.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
