
Case Report | DOI: https://doi.org/10.31579/2768-0487/130
1University School of Medicine, Department of Pediatric Hematology1, Department of Medical Genetics2, Department of Pediatric Endocrinology3, Ankara, Turkey.
2Pediatrics Residency, Gazi University Faculty of Medicine, Department of Pediatric Hematology.
3Professor of Pediatric Hematology, Gazi University Faculty of Medicine, Department of Pediatric Hematology.
4Assistant Professor of Medical Genetics, Gazi University Faculty of Medicine, Department of Medical Genetics.
5Professor of Pediatric Endocrinology, Gazi University Faculty of Medicine, Department of Pediatric Endocrinology.
*Corresponding Author: Zühre Kaya, Professor of Pediatric Hematology, Gazi University Faculty of Medicine, Department of Pediatric Hematology.
Citation: Nihan Öztürk, Zühre Kaya, Gülsüm Kayhan, Aysun Bideci, (2024), Diagnosis of a sickle cell carrier while investigating the cause of neutropenia in a child with short stature receiving growth hormone, Journal of Clinical and Laboratory Research, 7(2); DOI:10.31579/2768-0487/130
Copyright: © 2024, Zühre Kaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 February 2024 | Accepted: 01 March 2024 | Published: 12 March 2024
Keywords: sickle cell carriers; short stature; growth hormone
Short stature requiring growth hormone treatment is a well-known complication of sickle cell anemia (SCA). Sickle cell carriers can experience a variety of complications similar to SCA; however, short stature has not been documented in sickle cell carriers yet. Diagnosing using a complete blood count in sickle cell carriers is also difficult. Thus, hemoglobin (Hb) electrophoresis is useful in diagnosing these carriers. We present a case in which a sickle cell carrier is identified using Hb electrophoresis while investigating the etiology of neutropenia in a child using growth hormone for short stature.
Sickle cell trait occurs in around 300 million individuals worldwide [1]. The sickle cell trait affects approximately 13.6 percent of the population in Turkey's Mediterranean region [2]. In contrast to thalassemia carriers, sickle cell carriers can develop clinical symptoms similar to sickle cell anemia (SCA) patients; therefore, it is crucial to identify sickle cell trait individuals [3]. However, utilizing a complete blood count (CBC) to determine a sickle cell carrier is difficult. Hemoglobin (Hb) electrophoresis plays a crucial role in identifying sickle cell carriers. Thus, we present a child who was diagnosed with sickle cell carrier by coincidence while examining the cause of neutropenia and receiving growth hormone (GH) treatment for short stature.
A 10-year-old girl was referred to our Hematology department for an investigation into the reasons for neutropenia. Her medical history revealed that she was diagnosed with GH deficiency due to short stature, GH treatment was started at another center three years ago, and neutropenia was found two weeks ago. When she was 7 years old, her height was 107 cm (3P), -3 SDS in specific anthropometric measurements, her annual growth rate was less than 4.5 cm, her bone age was behind according to calendar age, and GH stimulation tests were unresponsive in two different measurements.It was learned that the patient was examined for prolonged jaundice in the neonatal period, her maternal grandmother had gallstones, her father was from Hatay and her mother was from Mersin, but they were not related to each other. Laboratory examination revealed Hb 12.3 g/dL, mean corpuscular volume 80.7 fL, reticulocyte 1.4percentage, and normal erythrocyte morphology in peripheral smear. Hb electrophoresis revealed HbA 53.4percentage, HbA2 2.8percentage, HbS 42.8percentage, HbF 1percentage. Her vitamin B12 level (545 pg/mL), ferritin level (33 ng/mL), folic acid level (13 ng/mL), indirect bilirubin level (0.74 mg/dL), and lactate dehydrogenase level (223 IU/mL) were all within the normal range.
Her family members were tested for CBC and Hb electrophoresis. Although CBC values were found to be normal in her father and brother, the HbS band was detected in Hb electrophoresis (Figure 1).
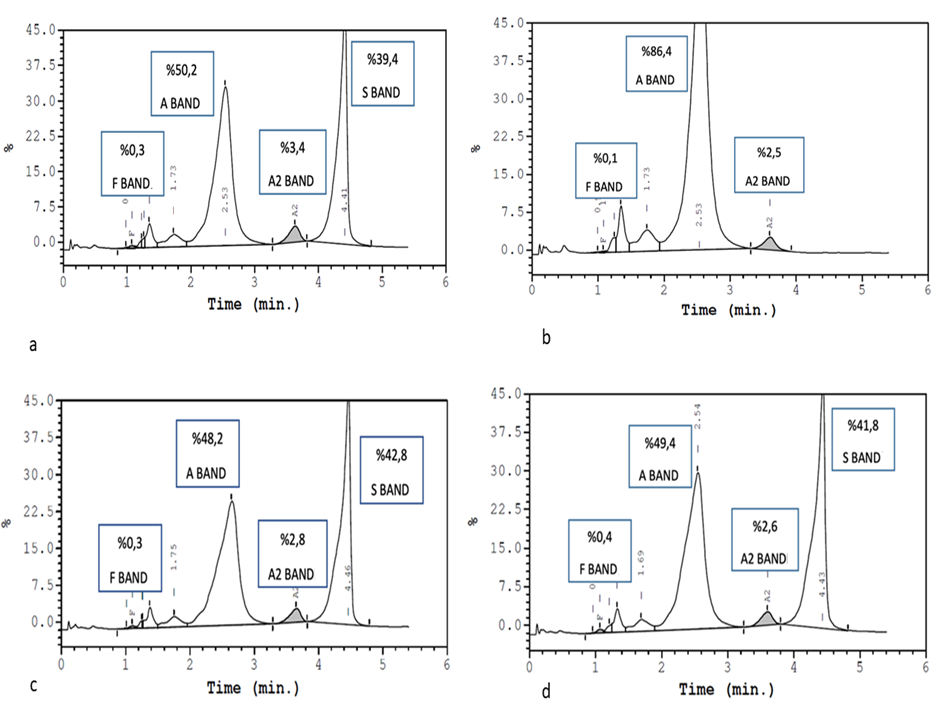
The mother was found to be normal. A pathogenic heterozygous mutation in the HBB gene, c.20A>T(p.E7V) (p.Glu7Val) (HbS), was identified in the patient, her father, and her brother. During the follow-up, the neutropenia improved, and GH continued. It was thought that neutropenia secondary to viral infection developed in the patient Genetic counseling was given for sickle cell carriers.
Thalassemia and SCA are both autosomal recessive hemolytic anemias. Patients with thalassemia or SCA require long-term, regular blood transfusions. The complication of transfusional hemosiderosis may develop over time. Advances in iron chelation therapy may prevent this problem. Allogeneic stem cell transplantation and gene therapy show promise as curative therapy for these patients [4]. However, it is essential to avoid the birth of thalassemia or SCA patients. Before marriage, our country's health officials performed a thalassemia trait test based on CBC levels. Although typical CBC may detect most thalassemia carriers early, sickle cell carriers are more difficult to detect with CBC. The gold standard in both carrier groups is Hb electrophoresis using high-performance liquid chromatography [5]. Preimplantation genetic diagnosis could allow for allogeneic stem cell donation from a tissue-typing matching healthy sibling [6]. Short stature has been reported in patients with SCA due to iron accumulation secondary to transfusion, intense inflammation caused by vaso-occlusive crises, and ischemic causes [7]. Although clinical findings similar to those observed in patients with SCA have been reported in sickle cell carriers, short stature requiring GH therapy has not been reported so far.
Our experience suggests that sickle cell trait can be considered in children with short stature who require growth hormones, and a Hb electrophoresis test may be ordered.
The parents of all participants gave informed consent.
Z.K., N.Ö.; Data Collection or Processing: Z.K., N.Ö., G.K., A.B.; Analysis or Interpretation: N.Ö., Z.K..; Writing: Z.K and N.Ö.
No conflict of interest was declared by the authors.
The authors declared that this study received no financial support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
