
Short communication | DOI: https://doi.org/10.31579/2640-1045/085
*Corresponding Author: William Pereira Valadares, Department of Pharmacology, Institute of Biological Sciences, Belo Horizonte, MG, Brazil.
Citation: William P Valadares, D L Almeida, I D G Duarte, S H S Santos, T R L Romero. (2021). Diabetic Neuropathic Pain has Endogenous Modulation Depending on the Intensity of Physical Exercise: A Brief Communication. Endocrinology and Disorders. 5(5): DOI:10.31579/2640-1045/085
Copyright: © 2021 William Pereira Valadares, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 August 2021 | Accepted: 25 August 2021 | Published: 06 September 2021
Keywords: aerobic exercise; continuous exercise; opioid antagonists; opioid system; painful diabetic neuropathy; peripheral nervous system; physical exercise
The opioidergic systems play a key role in endogenous modulation of neuropathic pain, given that Naloxone, a nonselective opioid receptors antagonist at a dose of 100 µg, reverted the antihyperalgesia caused by physical exercise demonstrated in our previous study. Due to the lack of relates regarding the control variables of physical exercise and endogenous modulation in neuropathic diabetic pain, we investigated if such modulation is exercise intensity dependent.
Background
The opioid system is classically known to participate in pain modulation acting mainly upon µ opioid receptors, and several drugs are used in clinical practice to control pain symptoms [1]. Physical exercise can activate the endogenous opioid system given that the non-selective opioid receptor antagonist Naloxone can revert analgesia promoted by physical exercise, systemically [2] and peripherally [3]. Among the variables that control physical exercise, the intensity is a factor that can directly modulate the opioid system altering the antihyperalgesic response observed in our previous studies. The aim of this study was to investigate whether different intensities of aerobic physical exercise on a treadmill can modulate differently diabetic neuropathic pain in an animal model.
The protocols used to induce diabetes and diabetic neuroaphy, calculation of maximal intensity exercise, mechanical sensibility test and the pharmacological approach can be accessed in our previous work [3].
In this work we used Progressive-maximal physical exercise protocol until fatigue to quantify the 80% and 40% of maximal speed used in the protocols of continuous exercise of this study (Different intensities of continuous treadmill exercise). Further clarification about the protocols in different intensities can be seen in [4].
To match different physical effort intensities, we used the calculus of Work (τ), where animals developed different speeds and times but with the same final physical effort. The calculus of work was performed in each physical exercise protocol through the formula τ= F.Δs, to calculate parallel forces to displacement, due to the fact that the protocols utilized in this work did not predict inclination (0% inclination).
τ = Work
F= Animal Weight
Δs= Distance Traveled
After the progressive-maximal exercise until fatigue utilized in a first moment, we calculated the maximal speed of 80% and 40% to perform continuous exercises in these velocities. After a 7-days interval, animals were submitted to the velocities described above and performed the physical exercise in continuous speed until the work matches the obtained progressive-maximal exercise work.
The drug used was Naloxone (Sigma, EUA) a non-selective opioid receptor antagonist was kept in the freezer on a stock solution dissolved in physiologic saline. Immediately before injections, the initial solution is dissolved in saline to be administered in a dose of 100μg per paw in a final solution volume of 20μL. Dosage mentioned was administered with a 100 unit’s insulin syringe by means of intraplantar injection in the right hid paw.
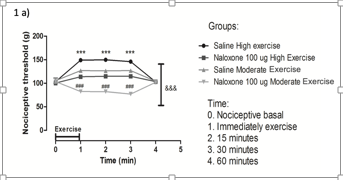
In the group shown in figure 1a (control group), higher intensity exercise induced a greater analgesic effect on neuropathic pain than moderate exercise when saline solution was administered.
The analgesia presented lasted 30 minutes after performing the exercise protocols, returning to the basal level (0). When Naloxone 100 μg was administered, there was a reduction in the analgesic response induced by high-intensity physical exercise in animals, however, the dose of naloxane described above was not sufficient to completely oppose the analgesic effect of the exercise protocol. In the moderate exercise protocol, when the same dose of Naloxane was administered, the action of this drug was completely opposed to the endogenous modulation of pain previously observed, as we observed a reduction in the nociceptive threshold and a consequent naloxone-induced hyperalgesia.
In the neuropathic group (Figure 1b), the same response profile was observed, in which high-intensity exercise induced a significant increase in the nociceptive threshold compared to moderate-intensity exercise in mice injected with saline.
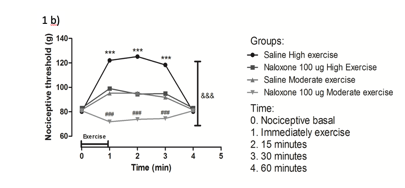
The analgesia lasted for 30 minutes after the completion of the exercise protocol. When mice were injected with 100 µg Naloxone, it was also observed a reduction in the nociceptive threshold induced by high intensity exercise but the dose of Naloxone was not sufficient to oppose the analgesic effect of the physical exercise protocol. The same dose of Naloxone injected in mice submitted to continuous moderate exercise was able to completely oppose the endogenous modulation of pain, given that we observed a reduction in the nociceptive threshold and a consequent hiperalgesia induced by Naloxone.
Both groups, control (Figure 1a) and neuropathic (Figure 1b), showed similar responses to different exercise intensities. We observed in our results that the endogenous analgesia caused by the physical exercise protocols used in this study was intensity dependent. Naloxone was able to reduce the analgesic response in continuous moderate exercise causing hiperalgesia in both groups, control and neuropathic (Figure 1a and 1b). However, the hyperalgesia was not observed in the continuous high intensity exercise in either groups, causing only a lesser analgesic response.
It is known from the literature that the opioid system has a crucial role in the modulation of nociceptive stimuli that ascends from the periphery, and physical exercise can stimulate the liberation of endogenous opioids in the central nervous system. With the data collected from the experiments of exercise intensity we can hypothesize that the endogenous liberation of opioids, at least in the peripheral tissues, is directly dependent on exercise intensity and, the analgesia observed in mice after exercise is related to the amount of exercise induced endogenous opioids release.
It can be concluded that the intensity of aerobic exercise plays a fundamental role in the endogenous modulation of animals with diabetic neuropathic pain, and the opioid system plays an important role in the peripheral control of painful impulses that ascend from the periphery.
This work was supported by the laboratory of Pain and Analgesia, ICB/UFMG and our fellow researchers and advisors.
Profile nociceptive threshold responses for exercise intensities in control and neuropathic groups. Figure 1a: Control group. Figure 1b: Neuropathic group. (&) indicate significant difference between groups; (*) significant difference between times (High exercise) and (#) significant difference between times (Moderate exercise).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
