
Case Report | DOI: https://doi.org/10.31579/2692-9392/137
*Corresponding Author: Nadia Boudjenah, General Surgeon, Diabetic Foot Surgeon, Diabetic Foot center, Algiers, Algeria.
Citation: Nadia Boudjenah (2022). Diabetic Foot in Algeria Illustration IV – Clinical Case Report. J. Archives of Medical Case Reports and Case Study, 6(2); DOI:10.31579/2692-9392/137
Copyright: © 2022 Jiancheng Zeng, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 July 2022 | Accepted: 11 July 2022 | Published: 18 July 2022
Keywords: diabetic foot; general surgeon; neuropathy
It seemed interesting to us to share this observation because it reflects our management of the diabetic patient with a wound and suffering from a severe disabling Neuropathy.
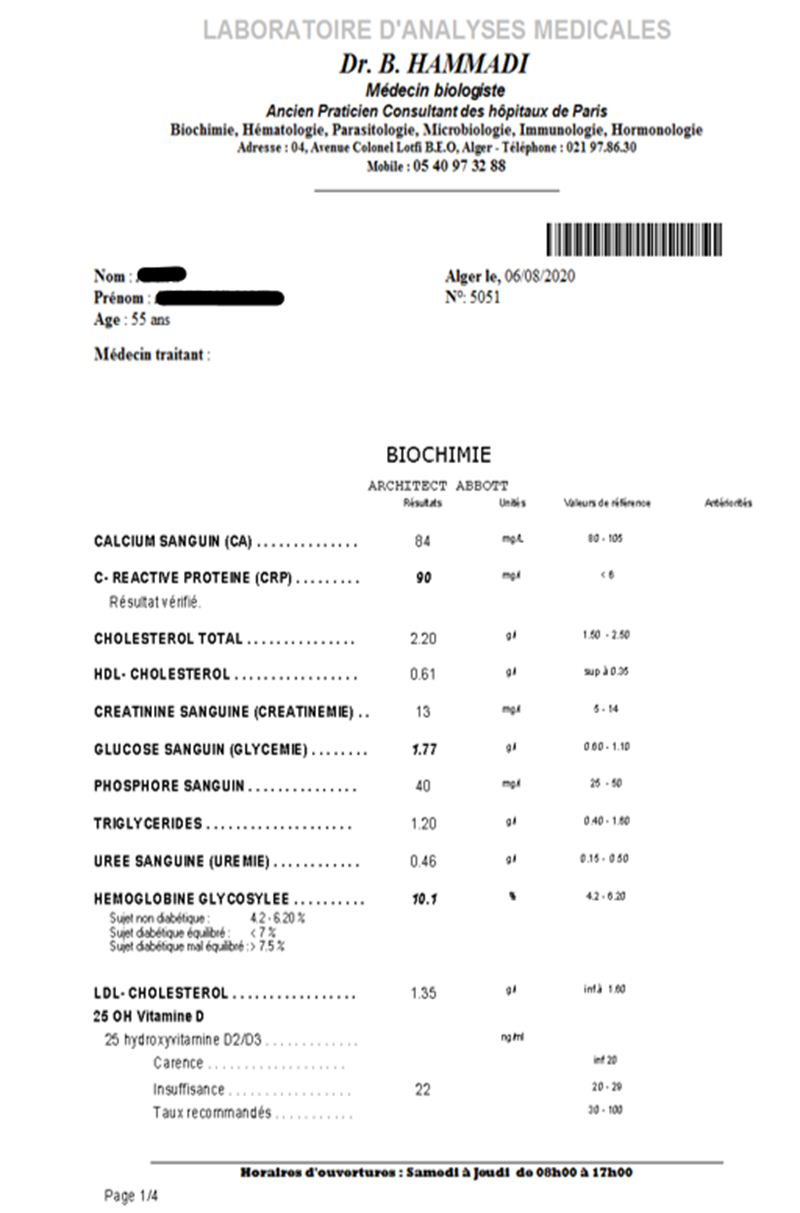
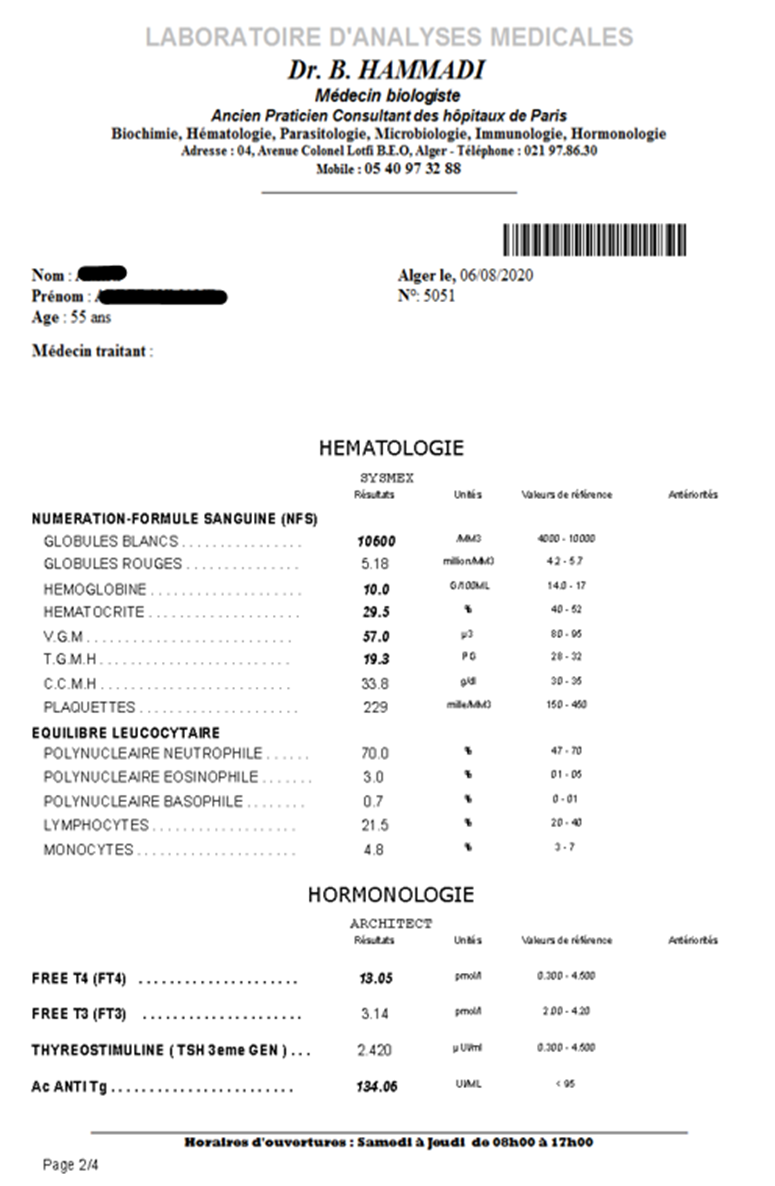
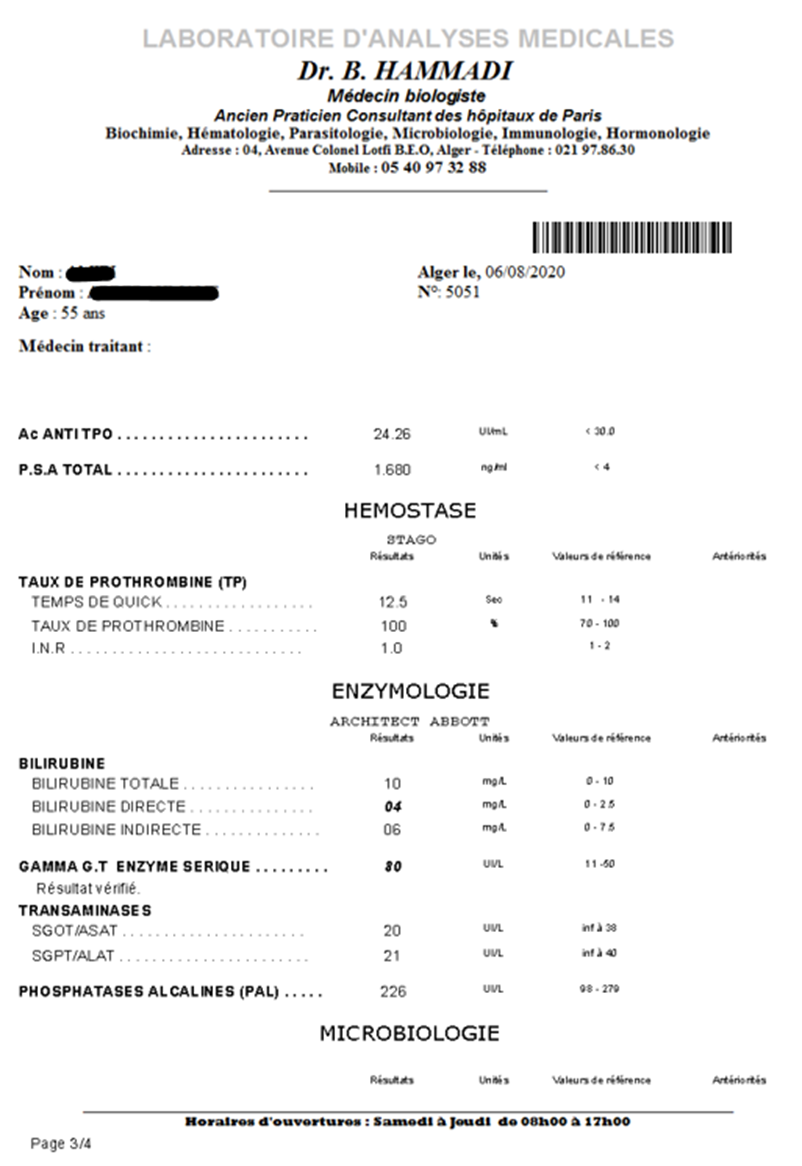
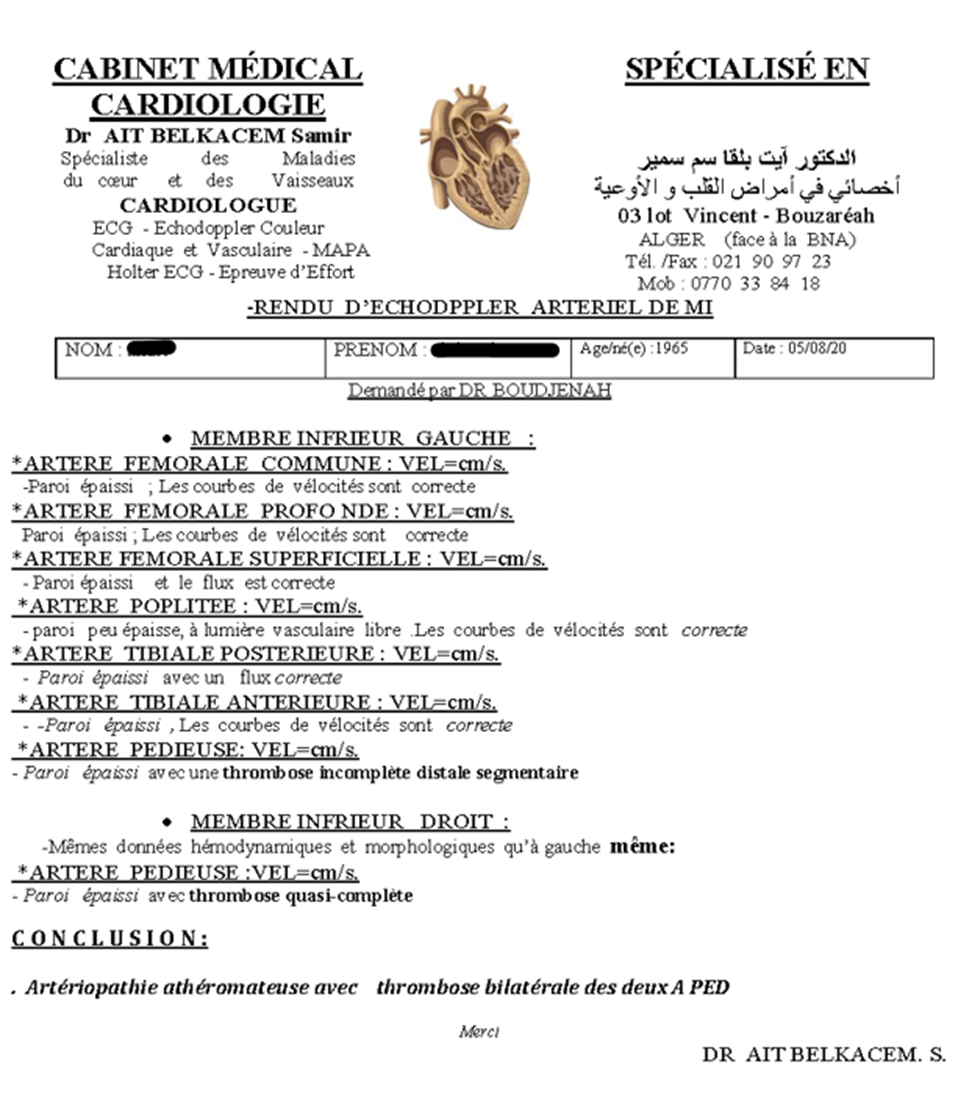
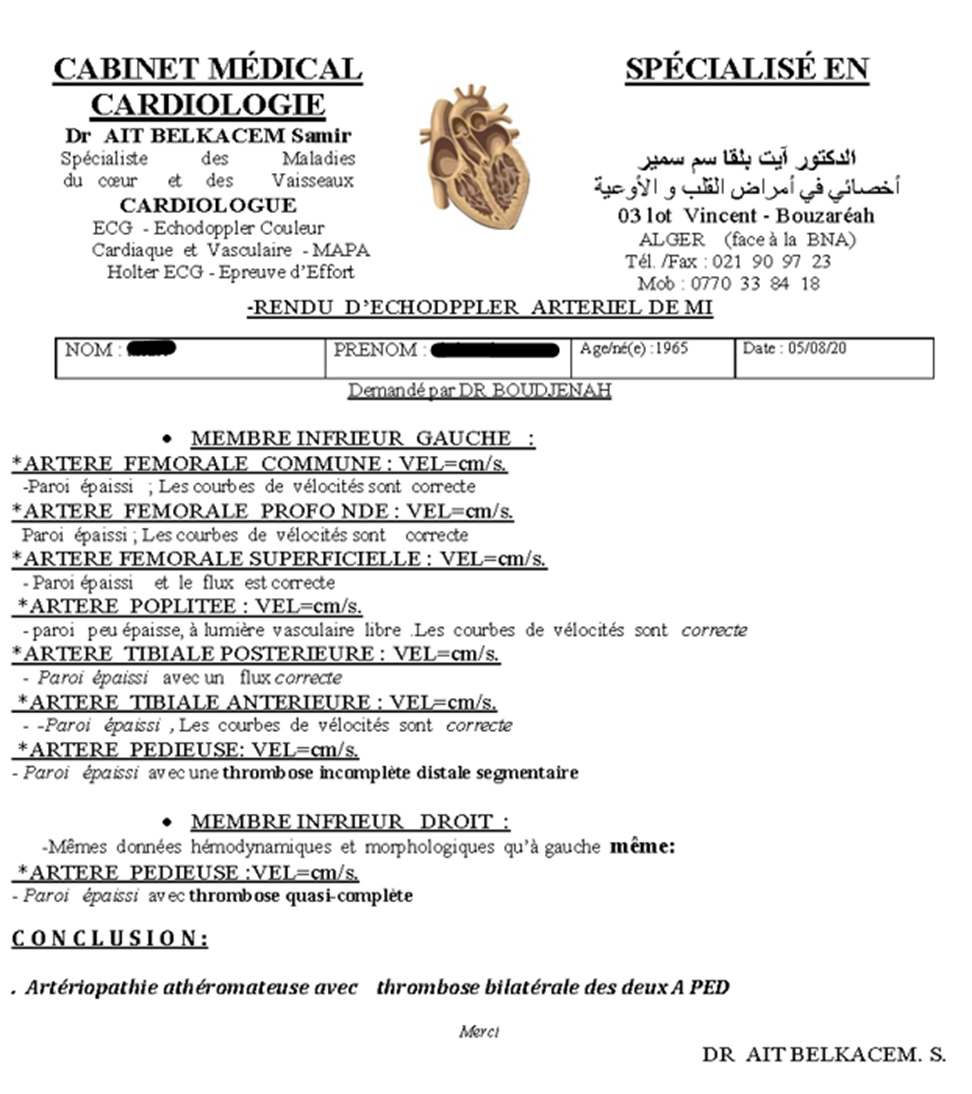
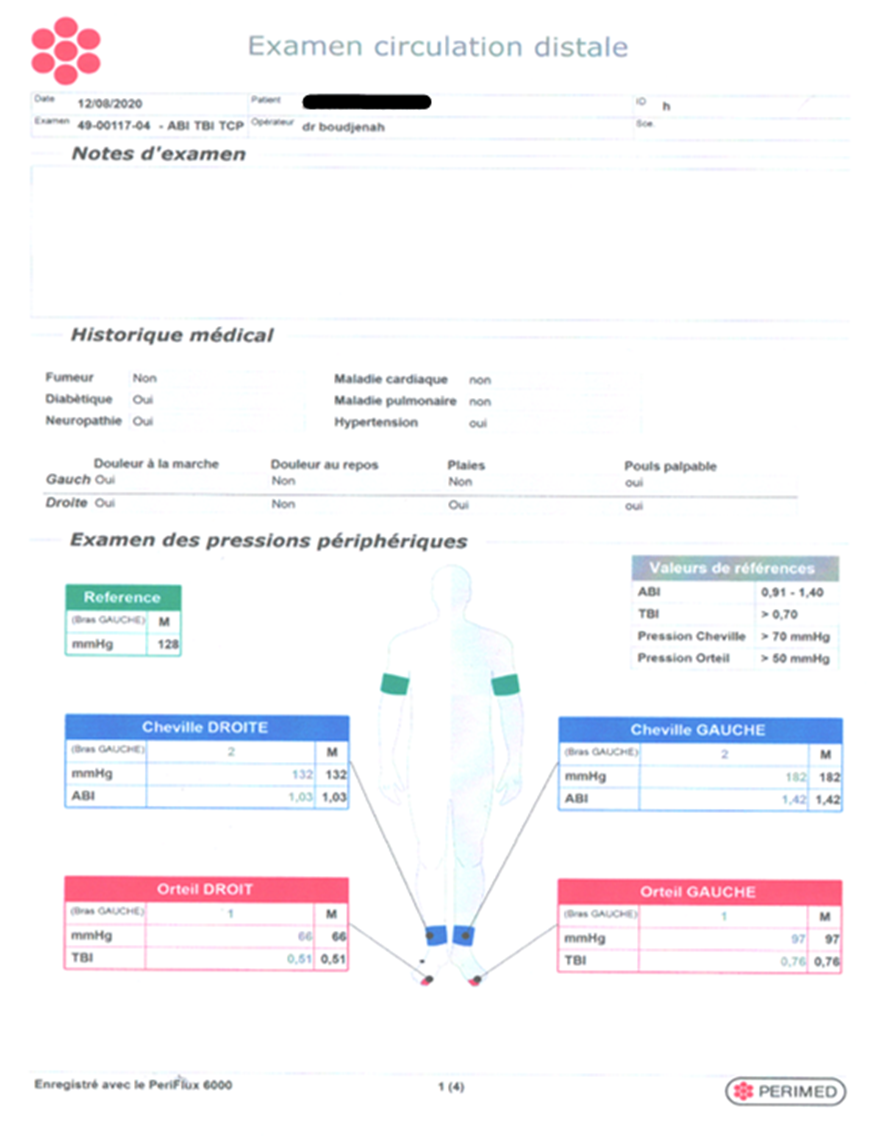
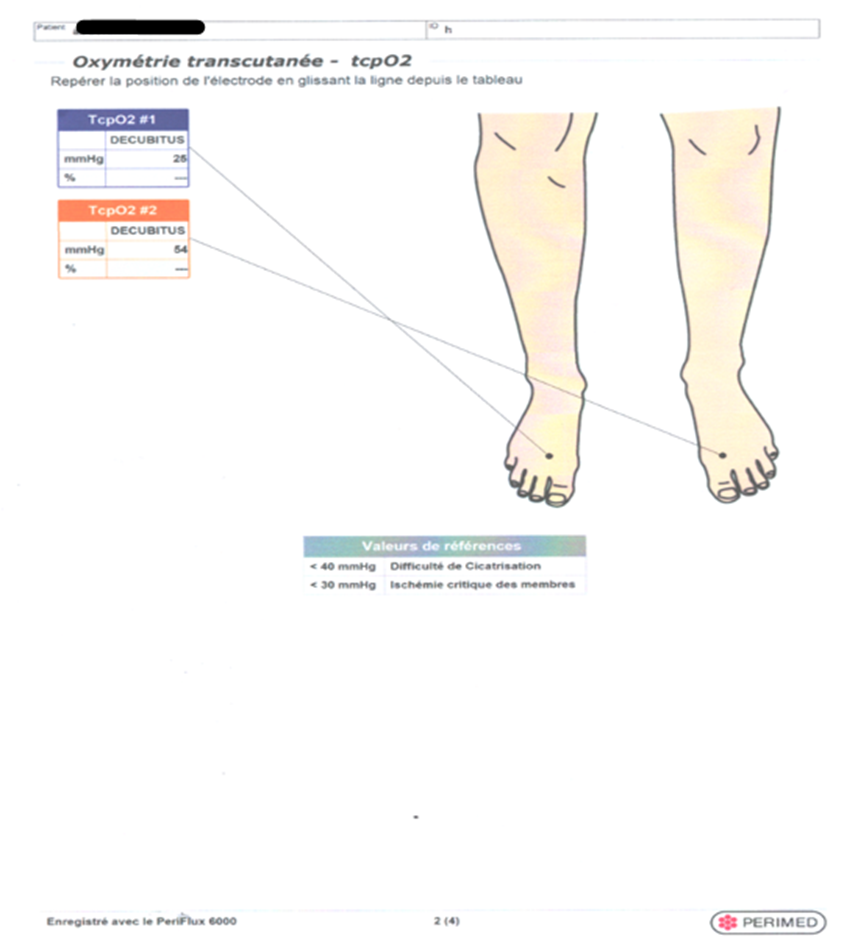
Our clinical case today is a 55-year-old male. A patient with type 2 diabetes, on insulin therapy and oral anti-diabetics and being treated for high blood pressure. He came to our consultation on August 05, 2020, with an infection of the right foot, of which the starting point is the second and third toes. These ones being ischemic
It seemed interesting to us to share this observation because it reflects our management of the diabetic patient with a wound and suffering from a severe disabling Neuropathy.
Our clinical case today is a 55-year-old male. A patient with type 2 diabetes, on insulin therapy and oral anti-diabetics and being treated for high blood pressure. He came to our consultation on August 05, 2020, with an infection of the right foot, of which the starting point is the second and third toes. These ones being ischemic. Picture below.

We also found, apart from foot damage, tingling and unbearable disabling pain of a neurological type on the four limbs with a predominance in the lower limbs.
This patient seemed asleep to us because of heavy medication. He was not feverish and his blood sugar on arrival was 3 g/l. We also found a moderate diastasis of the rectus abdominis.
To assess the patient's condition, we asked for several tests to be done as quickly as possible:


An ENMG revealed a severe and diffuse demyelinating Neuropathy in the four limbs, predominating in the lower limbs, as evidenced by the complement we requested following an ENMG of the lower limbs carried out on 06/22/2020.

However, medical support for the patient is not over. As we have described it, it can last up to 36 months.
Regarding the wound:
1. During the first week, on arrival:
A As local treatment:
B As medical treatment after bacteriological tests:
2. During 2nd week: - local treatment + Maggot Therapy.- Depending on the results of the antibiogram, we put the patient on Ciprofloxacin and Metronidazole, and we continue the anticoagulants. - Once the necrosis had been eliminated, we used Altrazeal powder* once a week to accentuate the budding allowing complete healing after 15 weeks’ time. Figure below:




-Carbomedtherapy (Carbon Dioxide Therapy): 1st session on the first day focusing only on the lower limbs. After obtaining the ENMG results, we started the treatment of the Peripheral Diabetic Neuropathy, therefore upper limbs, and lower limbs.
Diabetes is the main cause of Neuropathy worldwide. More than 50% of diabetics worldwide, whether type 1 or 2, are affected.
Neuropathy is a consequence of microcirculatory damage in diabetics. The damage caused destroys the nerves. It is causedby the aggression of hyperglycemia. Treating Diabetic Neuropathy is a big challenge. As an outpatient clinic specializing in the treatment of diabetic foot, over 95% of our patients have Neuropathy.
Clinical examination of the patient finds the classic Neuropathy signs: tingling, numbness, cramping, pain, electric shock, loss of especially plantar sensitivity, sensitivity disorder otherwise. In the upper limbs, we look for lesions of the carpal tunnel, as well as lesions of the tarsal canal for the lower limbs. In addition, we note the degree of dryness of hyperkeratosis, the existence of a diabetic foot ulcer or a Charcot foot. Amyotrophy is correlated with the severity of the disorder. It can cause paralysis. We have noticed that the first neurological damage is the Oto-Rhino Laryngitis sphere--we noticed a decrease in hearing. The diastasis-recti is a late sign and expresses the severity of Neuropathy. The diagnosis is confirmed by the realization of an ENMG of the four limbs.
So, for this fact and to relieve our patients, we first start by stabilizing the diabetes:
So, what is Carbomedtherapy (Carbon Dioxide Therapy)?
The carbon dioxide therapy is called Carbomedtherapy for diseases, and carboxytherapy for aesthetics. The CDT consists of transcutaneous injections of carbon dioxide.This technic was first practiced, in 1932,by Dr Barrieu, at Royat-Chamalières, France. Initially the indications were purely vascular especially for Raynaud’s syndrome, arteriopathy of the lower limbs, leg ulcers, and of course, in the care of the diabetic foot.
What are the benefits of Carbomedtherapy?
. On the vascular level: An improvement for faster healing of the wounds and improvement of a walking perimeter.
. On the neurological level: Repair of vasa nervorum leads to neurological regeneration which allows a reduction or even disappearance of pain, tingling and numbness.
Carbon Dioxide Therapy indications for diabetics
Diabetic foot: We have two separate tables:
1) Patients with wounds.
2) Patients without wounds, but with vascular or neurological disease. Unfortunately, very often these aspects are simultaneously entangled.
3) Diabesity
What are the Contraindications?
As a precaution, women who are pregnant. By obligation, patients with an imbalance of tares, especially respiratory and cardiac; Patients who had a recent acute stroke; Patients with active cancers and active viral infections; finally, with anaerobic germ infections. These situations can be reversed, however.
What are the side effects?
They are benign and above all reversible. There are superficial micro-hematomas at the injection points, which can sometimes follow a session especially if the patient is frankly de-coagulated. They disappear quickly and are not painful. There is no risk of gas embolism. The CO₂ pressures delivered by this machine are adjusted to avoid this problem even during accidental injection. The risks of infection should not exist. It is a simple matter of hygiene.
How to inject?
We use a device called CDT EVOLUTION. This device delivers heated carbon dioxide during the injections through disposable accessories: 13 mm and 30 G mesotherapy needles, and sterile tubing. The device being preprogrammed, we use the vascular program, the one which delivers 80cc of CO₂ per minute. The injections are transcutaneous and avoid well the vessels. We inject the surface of the 2 lower limbs, from the Scarpa triangle, around and on the wounds, and in the upper limbs in case of neuropathy. It is an outpatient practice. The rhythm of the sessions will depend on the severity of the case: once a week, bimonthly, or monthly
How does it work?
Hemoglobin molecules have 4 oxygen molecules at saturation. When we inject carbon dioxide, an exchange takes place between these oxygen molecules and those of CO₂. This phenomenon is described as BOHR effect (Figure. 1). We were able to record the instant nature of this exchange, by measuring PCO₂ and PO₂, during a CO₂ injection. What we found was that the PCO₂ measurement curve has not been changed while the PO₂ curve recorded an elevation.

Figure 1: Otherwise, CO2 acts as a vasodilator on the precapillary sphincters, transforming silentzones into functional vascular zones. This is what we call false angiogenesis. This action is perpetuated by the repetition of the sessionsby a real angiogenesis. So, there is an influx of blood. At the cellular level, exchanges become more important.
Evolution under Carbon Dioxide Therapy treatment
The evolution under the Carbon Dioxide Therapy treatment follows a scheme described below:
. At the neurological level:
In the first place, the tingling disappears then the cramps--we believe that the correction of the Vit D3 rate is not unrelated to this. The pain gradually decreases as the Carbon Dioxide Therapy sessions progress. It is imperative to obtain a normal HbA1c level from the patient. Hyperglycemia is a real obstacle to healing by maintaining the perpetual attack of the nerves.
The second parameter is ambulation, the resumption of which remains difficult when physical activity no longer exists. Exercises performed by a third party to combat stiffness and muscle atrophy are necessary. The use of a wheeled walker allows confidence to be restored for walking autonomy. We consider the psychological problem linked to the fear that has settled in these patients with multiple histories of falls without counting the effects of the analgesic therapeutic withdrawal that we set up from the start of treatment.
The recovery of especially plantar sensitivity is done from top to bottom from the Scarpa triangle to the sole of the foot. It manifests itself by the appearance of pain during the injections made during the different Carbon Dioxide Therapy sessions.
Before starting the Carbon Dioxide Therapy treatment sessions, an ENMG of the four limbs is performed by an independent neurologist chosen by the patient. The controlis done only after 12 to 24 sessions.
. At the vascular level:
Carbomedtherapy significantly improves vascularity. It repels ischemia and distinguishes necrotic from viable areas. We do not remove the necrosis so as not to deepen the lesions and thus obtain a well vascularized floor.
In conclusion, the Carbomedtherapy is a simple, safe, and efficient technique.
Due to its learning, it is within the reach of any interested doctor. It is carried out externally, which reduces the cost of treatment. It is also within the reach of all patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
