
Research Article | DOI: https://doi.org/10.31579/2768-2757/075
1 School of Medicine, Guilan University of Medical Sciences, Rasht, Iran Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
2 Faculty of Medicine, Qom University of Medical Sciences, Qom, Iran.
3 Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
4 Student Research Committee, School of Medicine, Shahid Beheshti University, Tehran, Iran
5 School of Medicine, Iran University of Medical Sciences, Tehran, Iran
6 Avicennet, Tehran, Iran
7 School of Medicine, Iran University of Medical Sciences, Shahid Hemmat Highway, Tehran, Iran.
*Corresponding Author: Sepehr Olangian-Tehrani, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Citation: Mohammadyari F., Biabani M., Faaliat S., Ahmadi A., Sepehr O. Tehrani, et al, (2023), Diabetes and Cholecystectomy: Is there a Relation? J Clinical Surgery and Research, 4(2); DOI:10.31579/2768-2757/075
Copyright: © 2023, Sepehr Olangian-Tehrani. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 April 2023 | Accepted: 24 April 2023 | Published: 02 May 2023
Keywords: cholecystectomy; diabetes; gallstone disease; laparoscopic cholecystectomy; gallbladder
The association between diabetes and cholecystectomy is debatable, as diabetes or cholecystectomy may be risk factors for each other. In this review, we look at the incidence rate, mechanisms, and complications of cholecystectomy in diabetic individuals and healthy ones and we also compare cholecystectomy in both to see whether diabetes is a risk factor for cholecystectomy or diabetes might lead to cholecystectomy, or both are contributed.
Over 1500 BC, Hindu scholars recorded the first description of diabetes in their writings [1]. According to the World Health Organization, the number of people with diabetes is increasing day by day; it has increased from 108 million people in 1980 to 422 million people. The increase in the prevalence of diabetes mellitus (DM) increases the awareness of biliary conditions in diabetic patients and thus leads to early diagnosis and improved outcomes.[2]. In fact, diabetes predisposes to the formation of gallstones, and surgery in diabetic patients is riskier than in nondiabetic patients.[3]. There are many diabetic factors that contribute to the formation of gallstones, such as obesity-related diabetes, insulin resistance, high triglyceride levels, and autonomic neuropathy [4]. Another common disease is gallstone disease (GSD), which increases with the increase in the prevalence of obesity [5]. Laparoscopic cholecystectomy is recognized as the gold standard for all symptomatic gallstone disease (GSD) and is more common in diabetic patients than in nondiabetic patients. Diabetics are more prone to infections due to high blood sugar, and this can weaken the patient's immune system and disrupt natural healing mechanisms [3]. Cholecystectomy has long been known as a safe procedure with no harmful effects on the body. However, recent studies show evidence of cholecystectomy with a high risk of metabolic syndrome (MetS) [6] and Also complications in diabetics are significantly higher than nondiabetics [7]. In general, cholecystectomy in diabetic patients shows a higher prevalence than non-diabetic patients[8]. Cholelithiasis and diabetes mellitus have an effect on each other's clinical course, and this led researchers to conduct more research in this regard in the past few decades [5]. Considering the increase in the incidence of gallstones and the use of laparoscopic cholecystectomy, as well as the mutual effects of diabetes and laparoscopic cholecystectomy, more studies should be conducted on postoperative complications in diabetic and non-diabetic patients. As a result, we decided to investigate the risk factors, postoperative complications and the mechanism of action of this treatment method.
Cholecystectomy
Cholecystectomy, the surgical excision of the gallbladder, is a common procedure all over the world with about 1.5 million incidences per year in the US. It is the treatment of choice for cholelithiasis with symptoms mostly biliary colic, acute cholecystitis, obstructive jaundice, or gallstone pancreatitis [9]. Other indications of cholecystectomy are complications of gallstone, that is acute calculus cholecystitis, gallstone in common bile duct, pancreatitis caused by gallstones, biliary dyskinesia, gall bladder polyps larger than 10 mm, cancer probability (calcified gallbladder) [10, 11]. In patients who are considered high risk for general anesthesia, being old or have cardiopulmonary diseases [12], coagulopathy problems, progressive cirrhotic liver or other hepatic diseases, or more risk factors that need open cholecystectomy, and who need extra attention because of the probability of the gallbladder cancer, cholecystectomy is considered as relatively contraindicated. In patients with respiratory or cardiac disease the preferred procedure is laparoscopic cholecystectomy [13], nevertheless if the patient is unable to bear CO2 in peritoneum or suffers from diffuse peritonitis or is hemodynamically unstable absolutely can't have LC [10]. There are two main classes of cholecystectomy: 1) open cholecystectomy: considered when laparoscopic procedure is not applicable for example due to anatomical reasons or cancers or concurrent surgeries on other organs [14] and 2) the minimally-invasive procedures such as the laparoscopic cholecystectomy (LC) which include 80% of surgeries because of fewer complications and the robotic surgery which needs much cost and time [10]. LC has similar morbidity and mortality to open surgery. But it has rapid recovery and less time spent in hospital [14]. New techniques of reduced port or single-port surgery or hybrid NOTES (natural orifice transluminal endoscopic surgery) which is different in earlier return of patient to day-to-day life, are the results of the attempts to reduce injury to the abdominal wall; although they haven’t been approved as they are applicable or safe in comparison to the routine 4-port technique of laparoscopic cholecystectomy [15]. The same consequences of the single-port and the 4-port approach make some authors suggest single-incision cholecystectomy over the traditional one as it has better cosmetic results in short-term [16, 17]; while others suggest the opposite due to lack of significant positive points and higher rate of late incisional hernia [13, 18, 19]. Complications of cholecystectomy include bleeding, surgical site infection, damage to colon or duodenum in surgery, peritonitis, and leak of bile which is rare but can be dangerous [20].
Diabetes
Diabetes implies "to pass through” and there are different types of diabetes such as type 1 diabetes, type 2 diabetes, gestational diabetes, maturity onset diabetes of the young (MODY), neonatal diabetes, wolfram syndrome, alstrom syndrome, latent autoimmune diabetes in adults (LADA), and Diabetes insipidus (DI) which is an endocrine disorder including the antidiuretic hormone and the posterior pituitary peptide hormone (ADH) [21, 22]. Diabetes mellitus (DM) is a gathering of metabolic disarranges that hyperglycemia is its common sign. the eyes, nerves, kidneys, blood vessels and heart can be damaged by Chronic hyperglycemia. “mellitus” comes from the Latin word for nectar or honey (pertain to sweet. Patients with DM are more likely to develop gallstone disease than general population. These maladies are categorized by pathology as gestational diabetes mellitus (GDM), type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM) and some other types. The group “other” made up of plenty complications yet account for 1% or less of the diabetes. Diabetes mellitus type 2 is our main emphasis [21, 23-25]. T2DM is a hereditary condition. Many genes are implicated, the majority of which have yet to be recognized. These genes regulate various chemical processes in β cell activity in pancreas. For each stage in the procedure, a distinct gene is in charge of enzyme manufacturing. A mutation in any of them can impair enzyme synthesis and inhibit insulin action. This inhibition can elevate glucose synthesis in the liver, disrupt glucose consumption by cells, promote triglyceride breakdown, impede fatty acid and glucose penetration to fat cells, and cause a variety of other metabolic problems. Insulin resistance is the most common problem in T2DM, and it develops several years before symptoms appear or growing a blood glucose level high enough to diagnose the disease. Insulin resistance develops in the body's peripheral cells (mostly fat cells and muscle) as well as the liver in obese people [24, 26, 27]. This disease regularly is pertained to as a noiseless executioner cause every year around 18% of all passing’s in the United States within 25-year-old sufferers and older [28].
Mechanism
Cholecystectomy is the most appropriate treatment option for gallstone disease (GD), while this treatment can cause metabolic syndrome through unknown mechanisms [29]. A study by Chen et al to investigate the main role of gallbladder in metabolic homeostasis has shown that the prevalence of metabolic disorders (for example NAFLD, diabetes, etc.) is due to its effect on glucose concentration, lipids, blood pressure and cardiovascular disease is more common in people who have had a cholecystectomy. After this surgery, a significant number of impaired GD functions, reduced intestinal trans-flow, and eventually rapid recirculation of the hepatic intestinal tract BAs, which act as signal molecules, will interfere with the expression of the BAs / FXR and BA / GPBAR-1 axis genes. Also, GPBAR-1 destroys the gallbladder [30]. Another study by Cortés V et al on non-obese Spanish patients with gallstones undergoing cholecystectomy showed that two years after surgery, there was a significant increase in serum insulin levels, the HOMA index. -IR, serum apoB levels and liver fat content were seen. Another study noted that after cholecystectomy, we saw decreased postprandial blood sugar control, increased serum and liver triglyceride levels, and LDL production. In these patients, we see a decrease in the concentration of duodenal BA after food intake, while serum levels of the hormone incretin, glucagon-like peptide-1 (GLP-1) remain constant. Also, the metabolic effects of cholecystectomy increase the concentration and probability of tissue exposure to BAs and the rate of basal metabolism, which can affect glucose and lipid homeostasis and increase the risk of hypertension and cardiovascular disease [31]. Gallbladder (GB) is a physiological pacemaker of BA hepatic circulation [30]. And the main function of the gallbladder (GB) is to absorb water and ions by epithelial cells and store bile. [29] This function is controlled by neuro-hormonal mechanisms [30]. Higher hepatic bile concentration than GB increases the digestibility of hepatic bile. GB also has motor function, which plays an important role in regulating BA flow in the intestinal circulation. This current affects the regulation of body homeostasis, BAs, cholesterol and TGs. After cholecystectomy, hepatic bile is secreted frequently in the duodenal lumen and BA circulates more rapidly, exposing most of the body's organs to this flow [29]. Cholecystectomy also prevents inhibition of cytochrome P450 1A1, an enzyme that limits the rate of bile acid synthesis, and increases the expression of ileal apical sodium-dependent bile acid transporter (ASBT) [31]. A can act as a hormonal signal by interacting with a variety of enteropathic and peripheral receptors. One of these receptors is the X farnesoid receptor (FXR), a ligand-activated transcription factor that responds to BA and is involved in glucose homeostasis. It is also a BA receptor with G protein (GPBAR1 / TGR5) that is expressed in human tissues (especially brown fat and skeletal muscle cells) to increase energy expenditure. BAs regulate glucose homeostasis by modulating this receptor in the small intestine and modulate insulin sensitivity. Activation of FXR protein, which improves insulin sensitivity, decreases PG concentration by decreasing gluconeogenesis, and increases glycogen synthesis, is involved in regulating energy intake, lipid metabolism, and glucose homeostasis [29]. In a study by Amigo L et al, it was shown that increasing the activity of the receptors mentioned above does not help human metabolism. A large part of the BA pool in the fasting person is divided into GB. In people who have undergone cholecystectomy, rapid release of BA into the duodenum does not occur after receiving food, whereas if GB is healthy, it can increase the concentration of BA in the duodenum up to 10 times after a meal. People with cholecystectomy can’t develop an immediate response to control lipid and glucose levels after eating compared to healthy people [29]. Fibroblast growth factor 19 (FGF19) is secreted in high concentrations in bile, which plays a significant role in lipid metabolism, glucose, and regulation of fasting energy levels. It also reduces the concentration of TGs and cholesterol, increases glycogen synthesis and suppresses insulin-induced fatty acid synthesis in the liver. GB mucosa is the site for enterohepatuliary expression of this factor. Studies show that ablation of GB reduces the serum concentration of this factor and increases the risk of metabolic disorders. GB ablation also suppresses Gpbar1 / TGR5 signals on the epithelial bilayer and GB smooth muscle, affecting and disrupting metabolic homeostasis [29].
Incidence
Around 10% to 15% of population of western countries have gallstones. 18.65% of cholecystectomy in diabetic patients in return of 17.15% in non-diabetics shows that diabetes mellitus increases the risk of gallstone diseases and at last the number of cholecystectomies in countries.[8] the result of case-control study with 161 diabetic persons in case and 166 non-diabetic persons for control in Benghazi Libya showed that 40% of diabetic patients have gallstone in return of 17.5% in non-diabetic patients.[32] In the population of China 9.9% of men and 11.6% of women are suffer from gallstone [33]. In Kashmir, India, 6.5 percent of people have diabetes and 5.7 percent have gallstones but diabetes increase the risk of having gallstone disease and 17.7 percent of diabetic patients have gallstone disease. The research of Chapman et al. [34] showed that diabetic people have higher risk of affection of Gallstone Disease. 32.7% of diabetics and 20.8% of non-diabetics have gallstone in population under test.
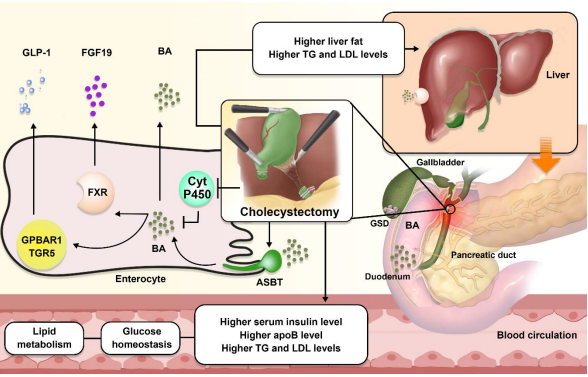
Figure 1: Correlation mechanisms and their role in cholecystectomy and diabetes.
Comorbidities and risk factors
In a study by Ruhl et al. [35] it has been shown that without age consideration, diabetic-related death was over 2.5 times more common in patients with gallstone disease. Also, gallstones were related to diabetes when has been distinguished. In another study it is reported that diabetic patients had a higher risk of disease of bile duct in comparison to non-diabetic patients [36]. While Gallbladder disease has a high risk of developing in patients with higher level of serum insulin after fasting, it can increase the risk of developing diabetes mellitus type 2 [37, 38]. Many studies have demonstrated a relation between cardiovascular disease (CVD) and gallstone disease (GSD). Construction of atherosclerosis plaques is boosted in diabetic patients and patients with lower level of HDL in blood. This procedure may be an important role in CVD and GSD [39-41]. Sludge is another risk factor for gallstone formation. It is demonstrated that higher level of bile cholesterol saturation index and lower level of bile salts can cause gallstone formation. Synthesis of bile salts in liver decreases when HDL level in blood drops. Thus, causing stone formation on gallbladder. HDL and LDL-cholesterol level is associated with type 2 diabetes [38, 41-43]. Lu et al. [44] demonstrated that despite of previous studies which has shown the positive correlation between non-alcoholic fatty liver disease (NAFLD) and cholecystectomy, NAFLD is a risk factor for cholecystectomy instead of being a result. Insulin resistance is a description for the link between NAFLD and T2DM [45]. obesity is another risk factor that rises the incidence of GSD and diabetes. It is associated with high level of insulin, resistance to insulin, over secretion of cholesterol in bile, and gallbladder hypomobility [46, 47]. in a study by shabanzadeh et al. [48] several risk factors have been examined. In male’s high free testosterone increase the occurrence of GSD. In other study it is shown that therapy with testosterone decreases insulin resistance and risk of diabetes type 2 [48, 49]. Vitamin D is necessary for function of smooth muscles in gastrointestinal system. Abnormal gallbladder muscle contraction increases the bile immobility and formation of cholesterol gallstones. In a study conducted by shabanzadeh et al. [50] it is shown that there is no notable relation between gallstone disease and 25-hydroxyvitamin D (25-OH-D). Estrogen is known to have a great impact on formation of gallbladder stones thus there is a higher risk of GSD incidence in women. This is due to the studies that showed higher stone formation during pregnancy and estrogen therapy. Also, it is shown that aging is another risk factor while there are few reports on stone formation in children and infants and higher prevalence above the age 20. Estrogen is known to have a protective effect in the development of diabetes. Estradiol can increase the insulin level which is stimulated by glucose therefore having an impact on glucose metabolism [51-53]. GSD and diabetes are linked to a variety of abdominal symptoms, including cirrhosis, cystic fibrosis, cholangitis, Crohn's disease, and Caroli's disease. These accompanying symptoms have been linked Unconjugated bilirubin calcium salts. For example, in chronic haemolytic diseases secretion of bilirubin can be associated to an elevated chance of calcium bilirubin ate sedimentation. GSD development can also be aided by chronic bacterial infections that effect the bile ducts. This can rise the mixture of calcium and bilirubin which is unconjugated. Bilirubin in an antioxidant which can protect the body from stresses causes by increased level of glucose in blood or diabetes. It also can increase the sensitivity of cells to insulin. [54, 55].
Complication
It is expected that diabetics are more likely to have some abnormal post-operative complications than those who don’t suffer from diabetes melitus [56]. According to Monika Lacka et al. [57] in 2020 the association between diabetes and the acute cholecystitis is independent and diabetic patients experience more frequent complications after cholecystectomy [57]. Of course, it should be noted that some studies have come to the opposite conclusion. A prospective study conducted in 2010 expresses patients with and without diabetes will have similar outcomes following laparoscopic cholecystectomy if careful preoperative preparation, rigorous intraoperative surgical technique, and careful postoperative care be done. Both groups did not experience major complications during the cholecystectomy or pneumoperitoneum procedures. In addition, the study mentions that the only difference between the diabetic and non-diabetic groups was the length of hospital stay, which was 5.6 days for the diabetics and 2.4 days for the non-diabetics [58]. Various studies have been conducted which result in different outcomes. One of discussed complications is about surgical site infection (SSI). An increased risk of SSI was associated with poorly controlled diabetes before surgery [59]. In 2014, a retrospective analysis revealed the probability of developing a surgical site infection is significantly higher in patients with diabetes who delayed their cholecystectomy for more than 24 hours following admission, but not systemic infections, and it was not reported in the non-diabetics [60]. Longer surgery time due to long hospital stays and more frequent complications including more SSI, more norepinephrine need in-hospital time due to cardiac deficiency, more requiring transfer to the ICU because of cardiac arrest in the diabetic are observed [57]. A history of diabetes increases the risk of renal failure, cardiovascular events, and even mortality following cholecystectomy for acute cholecystitis. These consequences and poor outcomes are more at insulin-treated diabetic patients [61]. In addition, increasing risk for pancreatic cancer in diabetics in comparing with without diabetes were noted as cholecystectomy complication at a population-based cohort study [62]. Another issue that has been discussed is postoperative pain. The time to onset postoperative pain was reported about 35 minutes in both groups. Furthermore, 60% of the diabetics experience intense pain while 20% of non-diabetics had it but beginning the post-operative pain was same for both (35minutes) [63]. Regarding the difficulty of surgery, a study in Iran which conducted by Sarmadi et al. [64] demonstrates laparoscopic technique has been more difficult for patients with diabetes [64]. It has been identified as a cause of conversion from the laparoscopic to the open surgery cholecystectomy in some researches and not in others [57]. Generally, most of studies have mentioned different postoperative outcomes between diabetics and non-diabetics and more and severe complications in diabetics for example SSI. But comparison among studies and data shows that results are contradictory. So, more analysis is required for proving definite and more probable complications.
The focus of this study is to understand the risk of developing diabetes after cholecystectomy in patients with gallbladder disease and the need for cholecystectomy because of gallstone disease in patients with diabetes mellitus. Results indicate that patients with diabetes mellitus have a great chance of developing gallstone disease which consequently might need surgical treatments. while some research shows that metabolic disorders like diabetes mellitus are more common in patients who have received cholecystectomy, others suggest that there is no relation between developing DM after cholecystectomy. Due to these contradictory results, more research is needed to show the relation between DM and cholecystectomy.
Ethical Approval and Consent to participate
Cause all data was acquired from clinical records and imaging
systems for normal follow up, us
institution was exempt from institutional review board approval.
Not Applicable
The authors declare that they have no conflict of interest.
This study has received no financial support.
Not applicable.
Not applicable.
F.M. and S.O. designed the study. F.M. organized the manuscript and wrote the manuscript. M.B., S.F., F.T., A.A., H.K., S.J., A.T. and S.O. wrote the manuscript. F.M. revised the final manuscript.
The final manuscript has been read and approved and reviewed by all authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
