
Case Report | DOI: https://doi.org/10.31579/2693-2156/025
*Corresponding Author: Sule Muhammad Baba; Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule MB, Gele IH, Shirama YB, Ribah MM, Aliyu AZ, et al. (2021). Dextrocardia with Situs Inversus in an 18-Year-Old Nigerian Female: The Computed Tomographic Findings and a Case Report. J Thoracic Disease and Cardiothoracic Surgery, 2(2); DOI: 10.31579/2693-2156/025
Copyright: © 2021, Sule Muhammad Baba, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 June 2021 | Accepted: 27 June 2021 | Published: 15 July 2021
Keywords: dextrocardia; situs inversus; adult, incidental; hemithorax; extracardiac abnormalities
Dextrocardia is a cardiac positional anomaly in which the heart is located in the right hemithorax with its base to apex axis directed to the right and caudad. The malposition is intrinsic to the heart and not caused by extracardiac abnormalities.
Dextrocardia is a rare condition and usually found incidentally and in association with other congenital abnormalities. It has an incidence of less than 1%.
This is an 18 year old Nigerian female who was referred for computed tomography (CT) of the chest on account of prolonged and recurrent cough with a suspicion of diffuse interstitial lung disease.
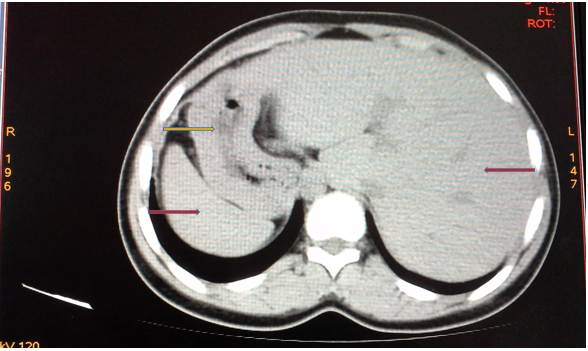
The chest and upper abdominal CT scan showed dextrocardia with a right placed heart, displaced spleen and stomach to the right hemi-abdomen and liver displaced to the left hemi-abdomen; confirming the diagnosis of dextrocardia with situs inversus.
We present this case of dextrocardia with abdominal situs inversus due to its rarity in literature.
Dextrocardia is a cardiac positional anomaly in which the heart is located in the right hemithorax with its base to apex axis directed to the right and caudad. The malposition is intrinsic to the heart and not caused by extracardiac abnormalities [1].
Displacement of the heart to the right by extracardiac causes like right lung hypoplasia, right pneumonectomy or diaphragmatic hernia is termed cardiac dextroposition and should be differentiated from dextrocardia [1-3].
Dextrocardia is a rare condition and usually found incidentally and in association with other congenital abnormalities. It has an incidence of less than 1% [4,5]. Dextrocardia has an incidence of about 1 in 12,019 pregnancies in the united states of America, the true prevalence in Nigeria is unknown [2,6].
Dextrocardia may be associated with variable anomalies; intracardiac and extracardiac anomalies [4,5,7]. The intracardiac anomalies such as discordant atrioventricular connection, univentricular atrioventricular connection, ventricular septal defects and anomalies of the pulmonary artery [4].
Dextrocardia has been classified in to four types; dextrocardia with normal positioning of abdominal organs (situs solitus with dextrocardia), dextrocardia with a reverse in position of abdominal organs (situs inversus with dextrocardia), dextrocardia with undifferentiated cardiac chambers (situs ambiguous) and the fourth type is a normal heart shifted to the right side of the chest (dextroposition) [2,3].
Situs inversus is a rare entity and reported to occur in 1 in 8000-1 in 25,000 patients [8-10]. Situs inversus is usually detected incidentally following presentation of the individuals with usually unrelated signs and symptoms [8,9].
Situs inversus has been divided in to two major types which are situs inversus with dextrocardia (commonest form) and situs inversus with levocardia (rare form) [8,11].
Dextrocardia has no known cause, but maternal diabetes mellitus and maternal cocaine use have been implicated. Factors like Genetics are also suspected with increased incidence found among conjoined twins [8,12,13].
Kartagener in 1933, described the association of sinusitis, bronchiectasis and situs inversus which was referred to as Kartagener’s syndrome [2,14].
This is an 18 year old Nigerian female who was referred for computed tomography (CT) of the chest on account of prolonged and recurrent cough with a suspicion of diffuse interstitial lung disease.
The patient is unmarried and looking well feed but in some form of respiratory discomfort. She is conscious and alert, not pale, anicteric, acyanosed, not dehydrated, not in painful distress, no pedal edema.
The pulse rate was normal and about 72 beats/minute, normal blood pressure of 110/60mmHg, and respiratory cycle of 12cycles per minute.
The chest and upper abdominal CT scan showed dextrocardia with a right placed heart, displaced spleen and stomach to the right and liver displaced to the left; confirming the diagnosis of dextrocardia with situs inversus viscerum (figures 1 and 2).
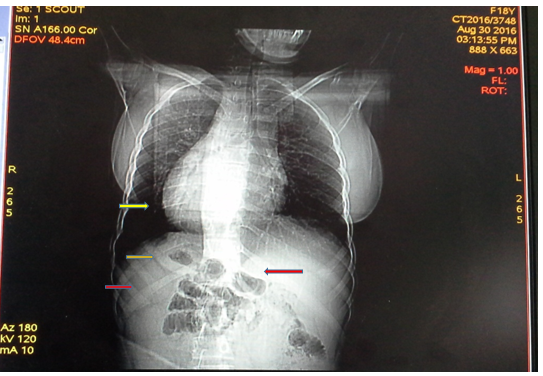
The chest scanogram or scout image showed differential lucencies with hyperinflation of the lungs more in the lower zones bilaterally. There is prominence of the airways; bronchi raising a suspicion of an interstitial lung disease with air trapping most likely bronchiectasis. See figure 1.
Following the above chest and upper abdominal CT scan with clinical presentation and history of prolonged respiratory symptoms we had a high suspicion of Kartagener’s syndrome.
Dextrocardia is a rare condition with presence or absence of situs inversus. Situs inversus which is either associated with dextrocardia or levocardia is also a rare entity; this index case is that of dextrocardia with situs inversus which has a right placed heart with displaced abdominal organs. No any extracardiac cause of displacement of the heart to the right side is demonstrated in this index case.
The commonest presentation of situs inversus are usually extracardiac and often respiratory due to its usual association of sinusitis and interstitial lung disease which was described by Kartagener in 1933; the index case also had prolonged and recurrent respiratory symptoms/complaint which were basically the reason for imaging and clinical evaluation with subsequent diagnosis.
Basic imaging facilities like radiography, computed tomography, magnetic resonance imaging with ultrasonography are reported to play vital role in the diagnosis of dextrocardia with or without situs inversus, our case was diagnosed following a non-enhanced computed tomography of the chest and upper abdomen.
The cause of the dextrocardia was not established in this case, this is similar to that reported in the literatures. The patient denied history of maternal diabetes or use of hard drugs like cocaine. No family history of similar symptoms or cases was documented in this case.
Dextrocardia may be associated with intracardiac anomalies; we were not able to conduct an echocardiography and electrocardiography in this case as at the time of presentation.
Dextrocardia is a very rare entity and maybe associated with abdominal situs inversus. A report of such cases will help in having a record of incidence/prevalence of the entity and may also assist in determining possible causative agents/etiology in our environment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
