
Case report | DOI: https://doi.org/10.31579/2690-4861/747
1 Szabolcs-Szatmár-Bereg County Hospital, Radiology Department, Hungary.
2 Szabolcs-Szatmár-Bereg County Hospital, Interventional Radiology Department, Hungary.
3 Szabolcs-Szatmár-Bereg County Hospital, Gynecology Department, Hungary.
4 Szabolcs-Szatmár-Bereg County Hospital, Radiology Department, Hungary.
*Corresponding Author: István Levente Kui, Szabolcs-Szatmár-Bereg County Hospital, Radiology Department, Hungary.
Citation: I.L. Kui, G. Ráski, B. Molnár, A. Lakatos (2025), Detection and Management of a Cesarean Scar Pregnancy, International Journal of Clinical Case Reports and Reviews, 24(5); DOI:10.31579/2690-4861/747
Copyright: © 2025, István Levente Kui. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2025 | Accepted: 28 March 2025 | Published: 03 April 2025
Keywords: ectopic pregnancy; cesarean scar pregnancy; uterine artery embolization
The management of a scar ectopic pregnancy with intrauterine and systemic methotrexate and bilateral uterine artery embolization.
Cesarean Scar Pregnancy (CSP) is a form of uterine ectopic pregnancy defined by full or partial implantation of the gestational sac in the scar of a previous cesarean section. It has high morbidity; the recommendation has been termination of pregnancy in the first trimester but several cases progress to viable births1. We discuss management strategies for this pathology that have been developed but no standardized treatment is available. We discuss the progress of a case report with CSP at our institution.
Clinical History:
A 30-year-old patient presented with abnormal uterine bleeding and lower abdominal pain at a gynecological emergency. Her further medical history includes 2 cesarean sections out of 4 pregnancies.
Elevated b-HCG was present.
Management of the case
The Trans Vaginal Ultrasound Reported: Gestational Sac: 27, Yolk Sac: 3,8 mm, CRL:10 mm.
There is present one living embryo in the lower part of the Uterus.
The chorionum frodosum is under the line of the cesarian scar. Peripheral Doppler sign is present under the cesarean scar. The Cesarean Scar pregnancy is probable, for this reason, further, MRI examination is needed.
On the MRI the uterus is 107 x 60 x 64 mm.
At the level of the previous operation, ventrally, the myometrial muscle is missing for 18 mm. Within the proliferating endometrium, approximately a 27-mm egg sac with a 13-mm signal-poor, irregularly shaped area is depicted. The cervix is intact. A cyst of 24 mm and a smaller cyst of 16 mm can be seen in the left ovary. The walls of the smaller cysts are unevenly thick, but bleeding is not shown in them.
There is no free abdominal fluid.
The bladder is not full, its wall is intact.
Opinion: Cesarean scar pregnancy. There is a complex cyst in the left ovary.
After these findings, the gynecologist decided to end the pregnancy. The first line used the extra-amniotic methotrexate, but the bHCG didn’t decrease significantly, so systemic methotrexate was administrated, without improvement of the analysis. bHCG remained high.
The next procedure was the interventional embolization of both uterine arteries.
The embolization was performed due to scar pregnancy affecting the ventral myometrium of the lower third of the uterus, also confirmed by MRI—two from the right and one from the left. The right dominant branch and the left artery were selectively catheterized (using a microcatheter on the right side). Embolization was performed with 355–500-micron PVA. The right subdominant branch is technically unsuitable for catheterization. The femoral puncture was compressed for a long time, then a compression bandage was applied. The patient received NSAID. We did not detect any complications.
A control MRI was performed. There are no ovules in the uterus now. According to the location of the removed ovum, a low-signal area with a maximum diameter of 50 mm can be observed with all sequences, which can be coagulum. The appearance of the myometrium is unchanged.
No significant amount of fluid is shown in the pelvis.
According to the left ovary, the cystic structures previously seen can still be observed, such as status items in other respects.
Review: Post. Op. Status.
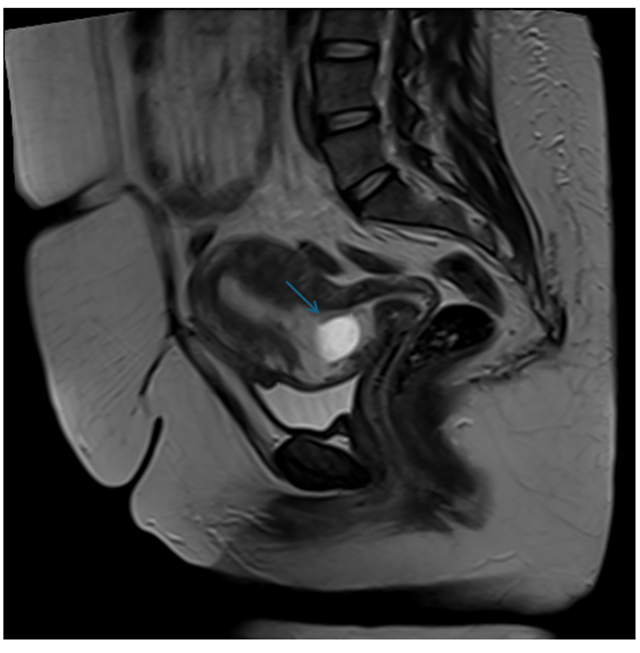
Figure 1: MRI, T2 TSE sagittal image.
Description: blue arrow showing the gestational sac in the lower part of the uterus.
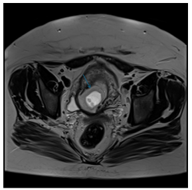
Figure 2: MRI, axial T2 TSE image.
Description: showing the gestational sac in the lower part of the uterus.

Figure 3: Embolization of the right main uterine artery.
The blue arrows show branches of the right Uterine artery, occluded with micro PVA.
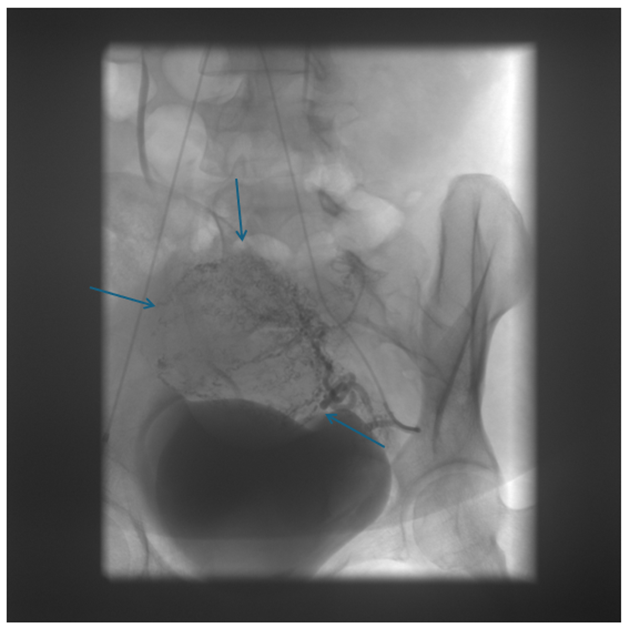
Figure 4: Embolization of the left uterine artery. The blue arrows show branches of the left uterine artery, which were partially occluded with PVA.
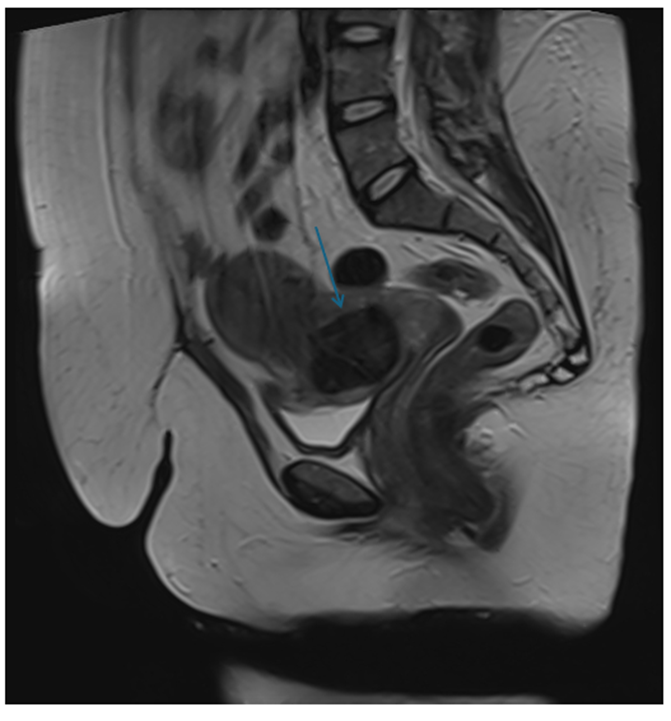
Figure 5: T2 TSE sagittal view on MRI
Description: big coagulum in the place of the gestational sac(blue arrow). (47 mm low signal lesion in the lower part of the uterus).
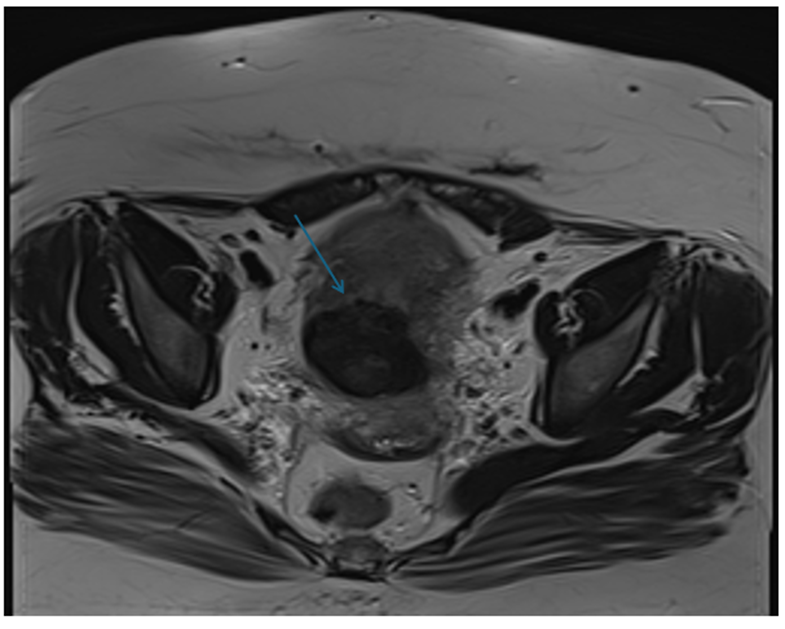
Figure 6: T2 TSE axial view. The blue arrow shows: the coagulum in the place of the prior gestational sac (47 mm low signal lesion in the lower part of the uterus).
A Cesarean Scar Pregnancy (CSP), in most of the published articles (CSP), is a form of uterine ectopic pregnancy defined by full or partial implantation of the gestational sac in the scar of a previous cesarean section.
The continuous increase in Cesarean Deliveries is causing a parallel rise in CSP and its complications. Considering its high morbidity, the most usual recommendation has been termination of pregnancy in the first trimester; however, several cases progress to viable births.1.
Several management strategies for this pathology have been developed in the last few years, but no standardized treatment is available.
In other centers, studies showed that the management was 1. expectant management, 2. medical management with methotrexate (MTX), 3. surgical treatment without removal of the CS niche, and 4. surgical treatment with removal of the CS niche.2.
In our case, after admission, pre-dilation was performed, and intra-amniotic methotrexate was administered under ultrasound control. A series of bHCG and ultrasound tests were conducted; the bHCG values persisted, and pregnancy showed early signs, so she received systemic methotrexate treatment. During observation, he received regular psychological care. In addition to decreasing HCG, active chorionic reaction persisted, therefore, interventional embolization of uterine arteries on both sides was performed. After ultrasound-confirmed chorionic demarcation, pre-dilation, and ultrasound-guided vacuum aspiration were performed in uterotonic protection, with tamponade of the uterus and vagina. Control laboratory tests showed no significant blood loss, the tampon was removed the next day without incident. Control ultrasound showed no abnormality, and bHCG values decreased significantly.
In the case of a cesarean scar pregnancy because of the high mortality rate is feasible to end the pregnancy with the combination of the local, systemic methotrexate, and bilateral uterine artery embolization. It has a good patient outcome.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
