
Case report | DOI: https://doi.org/10.31579/2578-8949/071
1 Sector of Dermatology. Santa Teresa Hospital. Santa Catarina State Secretary for Health.
2 Faculty of Medicine. Universidade do Sul de Santa Catarina.
3 Anatomical Pathology Post Graduation Program. Faculty of Medicine. Federal University of Rio de Janeiro.
4 Sector of Dermatology. Polydoro Ernani de São Thiago University Hospital. Santa Catarina Federal University.
*Corresponding Author: Gustavo Moreira Amorim. 135 Duarte Schutel Street, ap 402, Downtown, Florianópolis, Santa Catarina, Brazil.
Citation: Gustavo M Amorim, Ingrid R Paul, B Molozzi, Elisa R Dannebrock1, Timotio V Dorn, Roberto Moreira A Filho. (2020) Dermoscopy’s contribution for the diagnosis of folliculotropic mycosis fungoides. Journal of Dermatology and Dermatitis.6(1); Doi:10.31579/2578-8949/071
Copyright: © Gustavo Moreira Amorim, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 April 2021 | Accepted: 06 May 2021 | Published: 08 May 2021
Keywords: mycosis fungoides; dermoscopy; cutaneous t-cell lymphoma; cutaneous neoplasms
Folliculotropic mycosis fungoides (FMF) is one of the three recognized variants of mycosis fungoides. FMF predominates in men over 50 years old. Often it takes a long time for the definitive diagnosis after the onset of skin lesions. Dermoscopy today represents almost an extension of the clinical dermatological examination, with its application being expanded day after day in medical literature. The authors demonstrate the dermoscopic findings recently described in the context of FMF (follicular accentuation / white halo around the follicles), in a case of typical clinical presentation, with a diagnosis confirmed by the clinical-dermatological correlation.
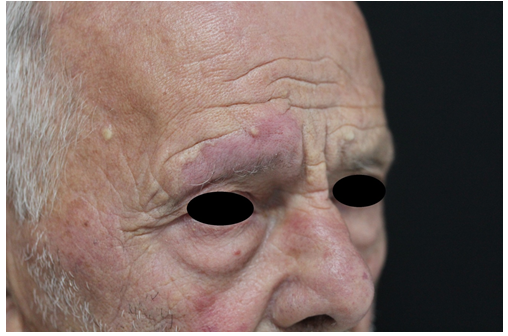
80-year-old male patient, farmer, born and raised in Antônio Carlos (rural area), with systemic arterial hypertension, with a previous history of ischemic stroke, with motor sequelae in the right hemibody; was referred for evaluation of a skin lesion on the face. He referred its appearance at least 2 years ago, with progression in size and number of lesions slowly and progressively. He complained of itching associated with the lesions.
Upon examination, 3 lesions were identified. The one of greatest importance and clinical expression was found in the right supraorbital region. It was an infiltrated erythematous plaque, with well-defined edges, showing a follicular accent. Especially when compared to the contralateral eyebrow, it showed hair loss associated. In parallel, there was two erythematous nodules in the malar region, ipsilateral to the supraorbital lesion.
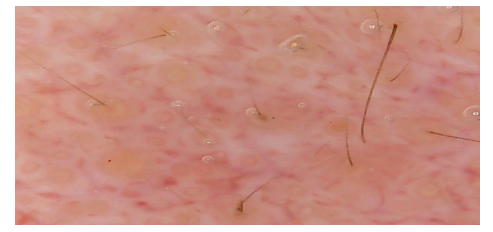
Dermoscopy revealed multiple yellow spots and white perifollicular halos, on a pinkish orange background with fine telangiectasias.
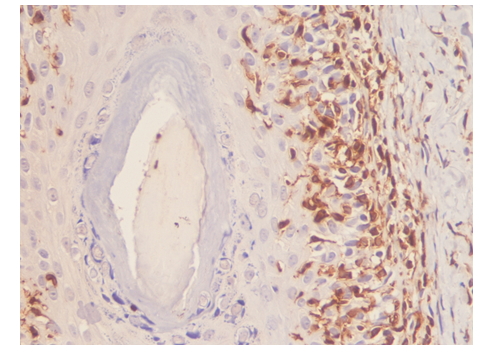
Histopathological examination of the lesional skin showed perifollicular lymphocytic infiltrate, predominating in isthmus and infundibulum, associated with folliculotropism. The presence of a discrete perivascular infiltrate and the presence of eosinophils were also observed. The interfollicular epidermis was preserved. Associated follicular mucinosis was identified. Immunophenotyping by means of immunohistochemistry determined the positivity of mature T lymphocyte antigens in the cells that permeated the follicular epithelium.
Clinical, histopathological and immunohistochemical findings allowed the diagnosis of folliculotropic mycosis fungoides.


Mycosis fungoides (MF) is the most prevalent primary cutaneous T-cell lymphoma. Folliculotropic MF (FMF), according to the current classification of the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC), is one of the three variants of classic MF (or Alibert-Bazin), along with pagetoid reticulosis and loose granulomatous skin [1-4].
FMF has as a fundamental aspect of its clinical-pathological definition: the marked presence of exocytosis of atypical T lymphocytes in the follicular epithelium (folliculotropism), associated or not with follicular mucinosis. Its first description is attributed to Giovannini et al., In 1906. This subtype of MF seems to be the most common among the “atypical”, representing up to 12% of cases in some cohort studies. It predominates in men, from the 5th decade of life [3-5].
The characteristic manifestations of classic MF are also the most common clinical findings associated with FMF - patches, plaques and tumors may occur. However, FMF presents with follicular accentuation, and plaques exhibit alopecia, comedones and erythematous follicular papules. Cysts and milia may also be found. Head and neck are the most frequently involved areas, and involvement of the eyebrows is highly characteristic. Pruritus is a common symptom that is often difficult to manage [4, 5].
The diagnosis of FMF is a challenge, given its polymorphic clinical presentation. The clinical-pathological correlation remains the “gold standard” for diagnosis. However, in general, the time between the onset of the condition and its definitive diagnosis is usually prolonged, averaging 24 months [6].
Dermoscopy is a non-invasive, low-cost and widely available method that allows visualization and characterization of colors, determination of vascular patterns and structures. It is incorporated into dermatological propaedeutics, making its use go beyond its initial objective in pigmented lesions. In addition, extensive literature supports its correlation with histopathological examination.
A pilot study seeking to characterize the dermoscopic findings of cutaneous lymphomas identified the presence of comedone-like structures in dilated follicular ostia (follicular pseudo-openings, classically described in seborrheic keratoses), surrounded by areas of peripheral stress [7]. Such an area of perifollicular accentuation, seen as a white halo around the follicles, would be a representation of the lymphoid infiltrate permeating the follicular epithelium, being an early finding of folliculotropism [8]. Its intensity is variable, according to the intensity of the lymphoid infiltrate and, sometimes, its visualization would be dependent on digital dermoscopy instruments [8]. As a tool for decision making, dermoscopy here would guide the biopsy exam, in order to surprise the finding of folliculotropism.
Possible findings in the context of FMF are described as the absence or reduction of terminal hair, an opaque or matte / copper red background, thin linear vessels and, less commonly, the spermatozoa-like vessels (similar to sperm) described in classical MF [7].
White areas without structure are a finding to be taken into consideration also in the evaluation of FMF, especially in more advanced lesions, since these would be the representation of fibrosis in topography of the follicular unit destroyed by the neoplastic process [7, 9, 10].
We demonstrate the dermoscopic representation of a case of typical clinical presentation of FMF, confirmed by clinical-pathological correlation, seeking to reinforce the method as an extension of dermatological semiology, contributing to decision making and guiding a “better” histopathological sampling site, possibly shortening the time between symptom onset and definitive diagnosis. We emphasize that the literature on this subject is still scarce and based on small series of cases, and the validity of these criteria presented in prospective studies with a larger sample should be tested.
The authors declare having followed the protocols in use at their working center regarding patients’ data publication.
Obtained.
All authors report no conflict of interest.
No funding. Authors were responsible for the minimal costs involved in this article.
We are grateful for the contribution of dermatopathologist Gabriella Di Giunta Funchal, PhD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
