
Case Report | DOI: https://doi.org/10.31579/2578-8949/076
1 Médico residente. Instituto Mexicano del Seguro Social, Hospital General Regional #45 Guadalajara Jalisco, Mexico
2 Endodontist, Endodontic department, Universidad Autonóma de Baja California.
3 Oral Surgeon, Oral Surgery department Universidad Autonóma de Baja California
*Corresponding Author: Daniel Jiménez Zaragoza MD, Médico residente. Medicina Interna, Instituto Mexicano del Seguro Social Calle Monte Olivos 7316, Lomas Conjunto Residencial. Tijuana BC Mexico
Citation: Daniel Jiménez Zaragoza, Jorge Paredes Vieyra, Francisco Javier Jiménez Enríquez (2021) Dermatological Aspects of Infections Caused By Endotoxins In Teeth With Necrotic Pulps And Apical Periodontitis. Journal of Dermatology and Dermatitis. 6(1); Doi:10.31579/2578-8949/076
Copyright: © nez Zaragoza, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 May 2021 | Accepted: 27 May 2021 | Published: 04 June 2021
Keywords: acute apical abscess; cellulitis; phlegmon; impetigo
Aim: To report an uncommon case of an extraoral sinus tract of the facial region caused by a tooth with an acute apical abscess in the mandible.
Case report: Established on oral examination and radiographic examination, an Acute Apical Abscess (cellulitis/phlegmon) of tooth 47 was diagnosed, which had resulted in a cutaneous sinus tract. The continuous purulent discharge of the sinus tract in the facial right region ceased after drainage and extraction of tooth 47.
Conclusion: It is challenging to diagnose and identify a cutaneous draining sinus tract of dental origin. Thus, treatment of skin lesions of the face (impetigo), and neck odontogenic infections should always be considered. Clinical and radiographic dental examinations can identify the tooth involved.
Chronic periapical inflammation drains along the path of least resistance, which commonly terminates in the form of a sinus tract, intraorally vestibular to the affected teeth [1]. However, depending on the relation between the localization of the periapical lesion and the facial muscles and fasciae, sinus tracts may drain by facial tissues [2]. Maxillary teeth drain extra orally when the infection is localized above, and in the mandible when the infection is localized below the muscle and fascia attachments [1].
The microorganisms that generate cavities, cause manifestations that if the patient does not attend soon, become chronic or aggressive and can generate problems in gums, bone, and facial tissues [3]. Therefore, this type of injury should be avoided, seeking the maximum elimination or reduction of microorganisms so that the treatment avoids damage to the surrounding tissues [4]. Reducing microbes and their by-products from the tooth prevents them from entering the apical area and draining into soft tissues of the face [5, 6].
Gram-negative anaerobic bacteria are the producers of lipopolysaccharides (LPS), called endotoxins [7]. Endotoxin is made up of polysaccharides, lipids, and proteins, where lipid A can generate its toxic consequences in soft tissues. LPS is released during or after the death or reproduction of bacteria [8, 9]. This clinical condition is present in a case of Acute Apical Abscess (cellulitis/phlegmon).
Endotoxins stimulate the discharge of competent cells, causing directly biological and immunological events, leading to an inflammatory process of apical bone resorption [10].
The reduction of bacteria and biofilms is achieved by treating the dental lesion or radically extracting the tooth [11]. A sinus tract or fistula is an abnormal canal that originates or ends in an opening. An orofacial fistula is a pathological communication between the cutaneous surface of the face and the oral cavity [6,7].
Tracts occur more frequently due to periapical lesions caused by mandibular teeth with pulp problems with a high incidence than those observed in the maxilla [12].
This pathway can go from an internal cavity or organ to the surface of the body.
Sinus tracts of dental origin can be a diagnostic problem for the clinician due to their appearance and opening in the skin and, occasionally, asymptomatic in their onset.
Dental infections, salivary gland injuries, neoplasms, and developmental injuries have been reported to cause oral skin fistulas, neck fistulas, and intraoral fistulas [2,3].
The possible differential diagnosis of a cutaneous draining sinus tract includes infected cyst, deep fungal infection, skin lesions such as furuncles [8], congenital fistula [13], salivary gland fistula [14], traumatic and iatrogenic lesions [15-16], osteomyelitis [17], tuberculosis [18], neoplasia [19-20], and actinomycosis [21].
The presented case reports an uncommon event of an extraoral sinus tract of the facial region caused by a tooth with an acute apical abscess in the mandible.
Anamnesis and medical history
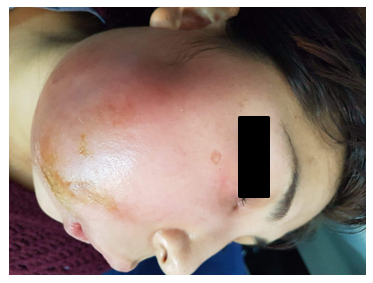
The 36-year-old woman attended the Specialized Dermatology Clinic for a persistent skin lesion located on the right side of the cheek. The patient claimed that the lesion had been present for at least 7 months.
Skin biopsies and histopathological examinations were performed twice. The tentative diagnosis of lymphadenoma was disproved and no signs of malignancy were detected. A different diagnosis of ‘mechanical manipulation’, was proposed. The patient was referred to the Department of Oral Surgery of the Dental School to examine for a possible dental infection.
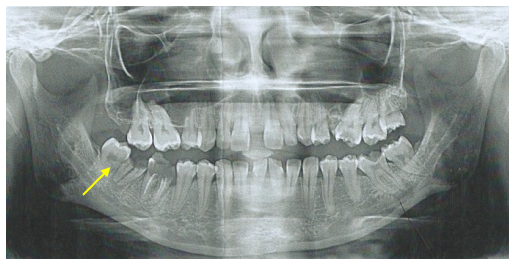
A panoramic radiograph revealed deep destruction and a periapical radiolucent area on tooth 47. The sinus tract was active with drainage of pus associated with severe pain. The patient presented acute symptoms of pain and tension in the skin in the area due to the gradual enlargement of the lesion. The skin lesion was associated with a considerable increase in temperature.
The salivation of the submandibular gland was regular. The patient was referred to the Oral Surgery Department to solve her problem. Oral inspection revealed insufficient glass ionomer cement restoration on tooth 47.
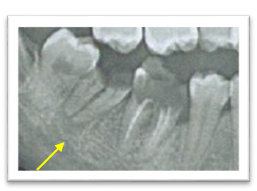
The panoramic radiograph taken revealed a considerable periapical radiolucent area associated with tooth 47. The periapical radiograph on the right side showed the sinus tract through a gutta-percha cone. The radiograph of tooth 47 showed deep interproximal caries (Figure. 1 and 2).
Biopsy of the area revealed some Streptococcus species, moderate numbers of Prevotella species, and Bacteroides capillosus.
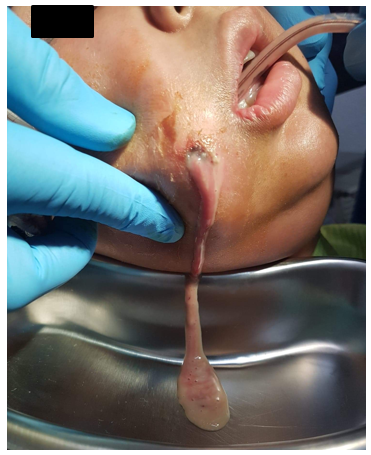
The patient was suffering from an asymptomatic Acute Apical Abscess (AAA, Cellulitis/Phlegmon) with suppurative apical periodontitis and a cutaneous sinus tract emanating from tooth 47 (Figure. 3 and 4).

The clinical protocol for this case of AAA was a drainage of the cavity through the skin on two occasions, first: to give relief to the patient due to the pressure on the area (Figure. 5).
The patient was received and treated with extreme limitation in her oral opening.
After the first appointment, 1gr of Ceftriaxona was administered every 24 hours for three days, Ixoprofeno of 60 mg every 8 hours for four days, and Ketorolaco 10 mg every 8 hours for four days [1, 5, 6].
In the second session, the phlegmon was drained and metronidazole of 500 mg was administered every 12 hours for 7 days, as well as clindamycin of 350 mg every 8 hours for seven days [6,7].
About a week later, the sinus tract was inactive. The patient confirmed a healing trend with a noticeable improvement in her mouth opening and the traces of the skin infection was improving. Once the patient was able to open her mouth, the oral surgeon extracted tooth 47. Tooth 47 was pulled out and the sinus tract orifice healed. Radiograph revealed diminishment of the periapical lesion and thereby revealed some healing was occurring.
In this clinical case, the cause of the cutaneous sinus tract was caused by extensive deep caries and an acute apical abscess. The complication for the patient was the development of an acute apical abscess also called cellulitis or phlegmon.
Persistent acute apical periodontitis led to the formation of a sinus tract. The evolution of the infection made that the tissues that surround the mouth and the cheek did not allow him to have a mouth opening to be treated orally. It is up to weeks after the cutaneous abscess was drained and the infection and pressure of the tissues reduced, plus the administration of drugs, allowed him to reduce his pain and inflammation [2].
In cases of an alarming odontogenic cutaneous sinus tract, patients usually consult a physician or dermatologist initially due to the absence of dental symptoms but with facial edema and increased temperature. It is very important to consider the dental reasons for inflammatory and persistent processes in the skin area of the face and neck. The unnecessary biopsies in the present case were performed twice and caused a delay in therapy and scars, so the patient should consult a trained dermatologist for their solution. Unfortunately, mistreatments in such cases are common [22, 23].
Correct diagnosis of a cutaneous sinus tract of dental origin can be detected by adequate oral diagnosis. The results of the histological examination of the odontogenic cutaneous sinus tracts were uneven [24]. The epithelial lining of the entire sinus tract is rarely produced, but it is frequently present in the skin openings. Most of the sinus tracts were not epithelialized and were only bordered by granulation tissue. It is commonly assumed that an epithelial lining can cause healing complications [24]. The therapy of cutaneous sinus tracts of dental origin consists of the removal of the infection source. After elimination of the reason for the infection by extraction of the tooth 47.
When the infection is eliminated by the extraction of the tooth, immune systems act automatically, and the skin lesion will be accomplished with a dermatological or corrective procedure.
It is challenging to diagnose a cutaneous draining sinus tract of dental origin. Thus, treatment of skin lesions of the face (impetigo), and neck odontogenic infections should always be considered. Clinical and radiographic dental examinations can identify the tooth involved.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
