
Research Article | DOI: https://doi.org/10.31579/2693-4779/209
Public Health Consultant, Bengaluru, India.
*Corresponding Author: Suresh Kishanrao, Public Health Consultant, Bengaluru, India.
Citation: Suresh Kishanrao, (2024), Deranged Resistant Blood Pressure- Challenges of Tailoring Medications!, Clinical Research and Clinical Trials, 10(3); DOI:10.31579/2693-4779/209
Copyright: © 2024, Suresh Kishanrao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 May 2024 | Accepted: 20 June 2024 | Published: 02 August 2024
Keywords: antihypertensive agents; blood pressure; clinical protocols; hypertension; hypotension, treatment outcome
Deranged blood pressure is a condition where an individual is hypertensive or Hypotensive. Hypertensive is a person over the age of 18 years with a systolic pressure reading of 140 mmHg or more or a diastolic reading of 90 mmHg or more as suggested by WHO. Similarly, a systolic BP lower than 90 mm Hg or a Diastolic BP of less than 60 mm Hg” is considered as Hypotension. European Society of Hypertension has tried to minimize the differences among multiple recommendations in 2023 and recommended ESH guidelines for management of arterial hypertension based on Hypertension disease staging and other risk factors like i) Hypertension mediated organ damage (HMOD), ii) cardiovascular disease, iii) diabetes and iv) chronic kidney disease. HMOD refers to structural or functional changes in arteries or target organs that can be present in long-standing hypertension but found in never treated patients at the first consultation and diagnosis. Current management strategies are based on the association of Hypertension with the complications identified at the time of first diagnosis, contrary to age old belief of initiating mono-drug therapy initially and adding additional drugs if the response is poor.
Materials and Methods:
This article aims to familiarise the Primary care providers and readers with the evaluation and management of resistant hypertension by discussing a recent patient’s case report of the struggle for last 6 months in author’s care, including consultations with a Nephrologist & a cardiologist, and lessons learnt of the most recent therapeutic approaches.
Treatment Outcome: It has taken more than 9 months from August 2023 till May 2024, to stabilize the patient’s (HTN, CVD &CKD) BP in recommended ranges.
SBP=Systolic Blood Pressure, DBP= Diastolic Blood Pressure Hypertension= HTN = Hypertension, HOT= Hypotension, NFHS= National Family Health Survey, LFT= Liver function Test, KFT= Kidney Function Test. CKD- chronic kidney disease, ACEi= Angiotensin-converting enzyme (ACE) inhibitors, ARB= Angiotensin II Receptor Blockers (ARB), DHP= 1,4-dihydropyridine (DHP), CCB= calcium channel blocker, WHO= World Health Organization, ESH= European Society of Hypertension , ICMR= Indian Council of Medical Research.
Hypertensives (or High Blood Pressure) is defined as persons 18 years of age and over with a systolic pressure reading of 140 mmHg or more or a diastolic reading of 90 mmHg or more, or those taking antihypertensive medications. Between 90-95% of cases are essential hypertension with no identifiable cause. The remaining cases of hypertension are secondary to a distinguishable process and would likely resolve if the underlying condition was treated. According to a 2023 report from the World Health Organization (WHO), hypertension is the most important preventable causes among the leading risk factors for death and disability worldwide. The number of people with hypertension doubled from 650 million to 1.3 billion from 1990 to 2019 globally. In their 2023 report WHO infers that high systolic BP (≥ 110-115 mm Hg) is the single most important risk factor for early death worldwide, causing more loss of life than even high blood glucose and tobacco use. However, of all adults with hypertension, only 54% receive a diagnosis, 42% receive treatment, and 21% have controlled hypertension despite growing numbers of safe, effective treatments. In 2021, it contributed to 10.8 million cardiovascular deaths globally.
Hypertension is widely encountered in family medicine. Despite its prevalence, some people have uncontrolled or difficult-to-control blood pressure. Resistant hypertension is defined as hypertension that is poorly responsive to treatment and requires the use of multiple medications to achieve acceptable blood pressure ranges. Primary Care Physicians use the word “Resistant hypertension “when the blood pressure remains above 140/90 mmHg despite optimal use of three antihypertensive medications of different classes, including a diuretic [1]. Resistant hypertension may be a consequence of secondary hypertension or have no identifiable cause, but it is important to recognise as it places patients at risk of end-organ damage.
Burden of HT in India: The prevalence of hypertension as per the National Family Health Survey Series Five (NFHS-5) was 21% of females aged over 15 years had hypertension compared to 24% of males of the same age range, as estimated in NFHS-5 (2019-2021) [3] as compared to 18.1% in 2015-2016 (NFHS 4) [2]. Empirical calculations using these data show that the number of patients with hypertension in India is currently about 200–250 million. The overall prevalence of hypertension is significantly higher (300–320 million) in the recently reported ICMR-INDIAB study as compared to other nationwide studies {[2] Feb 2024}. In India, 28% of adults (18+) suffer from hypertension, numbering to 250 million, 90% of them don’t get treatment, as 70% of cases are undiagnosed, and about 12% among the treated are ineffective to keep their hypertension within normal range. a recent large-scale study found [4]. Undiscovered and untreated, hypertension significantly increases the risk of developing cardiovascular, brain, and kidney diseases. A considerable number of patients fail to reach target blood pressure ranges despite lifestyle advice and standard medical therapy.
This article aims to familiarise the Primary care providers and readers with the evaluation and management of resistant hypertension by discussing a patient’s case report of the struggle for last 6 months in my care and seeking a Nephrologist and a cardiologist’s consultations and lessons learnt of the most recent therapeutic approach for hypertension management.
S Joshi, a 73-year-old male, sales executive was identified as hypertensive for the first time in January 2022. Due Rheumatoid arthritis of both knees his mobility was restricted since last 5 years, leading to hindering his freelance sales executive work. The wife also retired as private school teacher around 2020 and the family’s financial position was just enough to manage day to day life. She is also a known diabetic for last 20 years. The couple did not have any children which was another cause of psychological tension.
The local practitioner put him on Tab Cardace 2.5 mg {(an 'Angiotensin-Converting Enzyme (ACE) Inhibitors'} once a day in the morning when first diagnosed in January 2022. After 3 months observation the dose had to be increased 5mg per day and again 5 mg Twice day in June 2022. The BP was under control till December 2022, but he noticed a bit of swelling in lower limbs, for which he was give diuretic Tab Lasix (Furosemide a loop diuretic) to treat pedal oedema for about 10 days and then discontinued. For another 6 months he was maintaining the BP. In June 2023 He observed the oedema again and consulted me this time.

I first measured in sitting position, on both arms which were L= 180/110 mm Hg, R= 172/98 mm Hg. Repeated the measurements again after 10 minutes and got similar readings. Considering the arm with the higher systolic BP readings (180/110), I confirmed that the therapy given was not adequate. Ruled out any postural hypertension after measuring BP three times, at 1 min intervals, after 5 min of seated, supine and on standing, using an automated cuff sphygmomanometer. I had put him on 1) Embeta (Metoprolol Succinate with extended release) XR 25 mg once in the morning after breakfast (BF) (Which relaxes the blood vessels, slowing down the heart rate, and reduces the workload on the heart of pumping the blood effectively) 2) Lasix 20 mg in the morning after BF SOS (whenever oedema was noticed) and Tab. Anatensol 1 mg (used to treat depression).
He was doing well but in September 2023 he his oedema over feet increased up to knees. This time I suggested a Nephrologist consultation to rule out chronic kidney disease (CKD). A battery of investigations confirmed CKD.
21 September 2023: Nephrologist Consultation: BP = 175/95, Heart Rate= 95/min,
Tests done Value
(Parenthesis indicate Reference Value)
The Nephrologist’s Diagnoses:
“Hypertension, Renal Dysfunction, Renal Cyst and Vit D Deficiency”
Prescription:
Cardiologists Consultation:
29/08/2023: BP 187/87 & second reading after half an hour= 174/83, Pedal Oedema++,
ECG= Normal,
ECHO-Two-Dimensional Study: a) Valves: i) Mitral valve: PMAC+, ii) Aortic Valve= Calcified, iii) Tricuspid & iv) Pulmonary Valves- normal. b) Chambers: i) Left Atrium= Dilated, ii) Left Ventricle= Shows LVH, iii &iv) Right Atrium & Right Ventricle= Normal. c) Septae: IAS & IVS- Normal d) Great Arteries: Aorta, Pulmonary Artery & IVC- all normal. e) Wall motion abnormalities: Absent. Pericardium -normal, & Vegetation /Thrombus= Absent
Doppler Study: a) Mitral Valve: Grade I LVDD, Mild MR, Aortic Valve- Normal, Tricuspid Calve- Mild TR, Jet Gradient: 30mm Hg, PASP: 38mm Hg. Pulmonary valve- Normal.
Final Impression: Concentric LV Hypertrophy, Dilated LA, NO RWMA of LV at REST, Normal LV Systolic Function, Grade I LV Diastolic Dysfunction and MILD MR, MILD PAH
Ultrasound of Abdomen & Pelvis:
Prescriptions:
1.Tab Dytor 10 mg Once in the morning and second in the afternoon.
2. Tab Silodal D 8mg one in the night
3. Tab Telma Beta 50 mg Once in the morning
4. Met XL 50 mg one in the night (to compensate lack of walking /exercise)
5. Tab Met XL 50mg once in the night 0.2 mg one in the morning
Advised follow-up after 2 weeks.
Follow-up 21/09/2023
Pedal oedema ++, BP= 175/95, HR=95/Minute,
Serum Electrolytes: a) Sodium=144.4 mmol/L (135-145) b) Potassium = 3.97(3.5-5.5) c) Chloride = 104.4 (94-110)
Continued the drug regiment for another fortnight and follow up.
Follo-up 19 December 2023:
Disappointing, BP= 225/113, after half an hour 221/109,
No Pedal oedema.
Repeat Laboratory Report of 18/12/23 showed: Serum Creatinine= 2.06 mg/Dl,
Serum Lipid Profile a) Total Cholesterol= 175 mf /L (<200 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>
That made the cardiologist to suspect if the patient is taking medicine prescribed, both of us queried him. In view of no response to the drugs, terming it as ‘Resistant Hypertension’ he added Tab Minipress XL 5 mg one tablet in the morning and another in the night. Follow-up advised after 2 weeks.
The expenses on consultation fees (Laboratory investigations of INR 2000 every 2-4 weeks added to the financial problem, despite the cost next follow-up was compiled by end January 2024.
Follow-up on 30 January 2024: Despite changing the drugs in the last 2 monthly visits the BP recorded read 209/101 and the cardiologist and me suspected if the drugs are being consumed, However, after due verification learnt that tab. Minipress was not bought due to high cost. A revised prescription included: 1) Tab Dytor once in the morning, 2) Tab Telpres- MT 50 mg (Blocks an enzyme responsible for constricting blood vessels) Once in the morning 3) Tab Starpress XL 50 mg (A betablocker) 4) Tab Moxcent 0.2mg (another Blood vessels relaxant) one tablet twice (M/E) a day, 5) Tab Amlodac 5mg twice a day (M/E) 6) Tab Przaopress XL 5 mg Twice a day (M/E) (addresses BP and Mild BEP) 7) Silodal D (for BEP) one tab. In the night. Thus, 6 drugs combination was prescribed to address the resistant hypertension. I as family physician was bit surprised but assured the Cardiologist to monitor the compliance. Though the cost of treatment went beyond INR 100/day.
Thankfully, the progress was noted in the next 2 months, SBP &DBP coming in the range of 140-150 and 76-90 respectively by 13 March 2024, soon got stabilized by 16 March 2024, but the Diastolic BP came down to 64-70 and signs of postural hypotension were noticed.
Then I started reducing the number of drugs from first week of April 2024. First, I stopped the costliest drug of Prazopress (costing INR 30 daily) By 1 April 24 the BP was stabilized but much lower levels SBP=130-150 and DBP=70-74. By the end April BP remained at acceptable levels of SBP-124-140 and DBP-75-76. In mid-May the SBP= 130-134 and DBP= 57-62. I stopped another drug from 23 May 2024 Tab Telpress and for the last 3 days SBP is around 140 and DBP around 80 mm Hg. I plan to play with drugs choice, keeping in mind the cost and come down to most essentials 3 drugs regiment as recommended globally.
Blood pressure may be defined as the pressure exerted by the blood on the arteries and veins. It is measured by a sphygmomanometer and varies throughout the day, depending on: Body position, Breathing, Food & drink, Medications, Physical condition, Stress, Time of day.
Blood pressure is usually lowest at night and rises sharply on waking. Anxiety, Tensions for varied reasons elevate Blood pressure. Advanced age (50+), Dehydration, Pregnancy, low blood volume, lower BP. Health conditions like Pregnancy, Heart and heart valve conditions, endocrine disorders, Dehydration, Blood loss, Septicaemia), anaphylaxis, lack of nutrients in the diet and use of medications with poor monitoring cause low blood pressure.
According to a 2023 report from the World Health Organization (WHO), hypertension is among the leading risk factors for death and disability worldwide. Resistant hypertension is defined as hypertension that is poorly responsive to treatment and requires the use of multiple medications to achieve acceptable blood pressure ranges. In developing countries like India BP is a vital measurement by Primary care doctors, Nursing staff in major institutions and Trained field workers in community research like NFHS and Screening programs. Accounting that, four big ways-BP measurement can go wrong i) Equipment and the facility, ii) Staff, iii) Preparation of patients and iv) Procedure of measurement, Primary Care Physicians use the word “Resistant hypertension “when the blood pressure remains above 140/90 mmHg despite optimal use of three antihypertensive medications of different classes, including a diuretic. A systolic BP lower than 90 mm Hg or a Diastolic BP of less than 60 mm Hg” is considered as Hypotension. Five types of Hypotension are:
1) Orthostatic hypotension /Postural hypotension (OHT/PHT): is a sudden drop in blood pressure when standing from a sitting position or after lying down, which is defined as a sustained decrease in systolic blood pressure of 20 mm Hg or a decrease in diastolic blood pressure of 10 mm Hg within three minutes of standing compared with blood pressure from the sitting or supine position or by head-up tilt-table testing.
2. Delayed orthostatic hypotension (DOSHT): When sustained blood pressure (BP) drop is after three minutes of upright posture is called DOSHT. Dehydration, long-term bed rest, pregnancy, diabetes & some medications, cause this type of low blood pressure in older adults.
3. Postprandial hypotension (PHT). Blood pressure dropping after 1 to 2 hours after eating. Mostly affects older adults, especially those with high blood pressure or autonomic nervous system diseases -Parkinson's disease. Eating small, low-carbohydrate meals, drinking more water, and avoiding alcohol might help reduce symptoms.
4. Neurally mediated hypotension (NMHT): A BP dropping after standing for long periods, affects mostly young adults & children, due to miscommunication between the heart & brain.
5.Multiple system atrophy with orthostatic hypotension: called Shy-Drager syndrome A rare disorder affects the nervous system that controls involuntary functions such as blood pressure, heart rate, breathing and digestion. It's associated with having very high blood pressure while lying down.
Hormonal problems such as Hypothyroidism, diabetes, hypoglycaemia, some over-the-counter medications and prescription medicines for high blood pressure, depression, or Parkinson's disease and Heart failure may cause Hypotension.
Consequences of Deranged Blood Pressure:
High blood pressure eve if is resistant, damages the vessels when left untreated, it raises the risk of heart attack and stroke and develop heart failure and Aneurism. One can experience chest pain and severe headaches, it often causes kidney damage leading to chronic kidney disease (CKD), Likely to develop vision problems, by damaging blood vessels in the retina, called hypertensive retinopathy. It could lead to developing sexual dysfunction. Of late Hypertension is strongly associated with CVD and death while asleep.
Low BP / Hypotension on the other hand leads to Blurry vision, Confusion, Dizziness, Fainting, Light headedness, Nausea or vomiting, Sleepiness and Weakness. Orthostatic Hypotension is associated with increased odds of falls, increased co-morbidities, number of medicines used, and orthostatic intolerance. Elderly with diabetes, hypertension and cognitive impairment are at a higher odd of having OHT.
Practical implications:
In busy clinical practice, it may appear impossible to do both seated and supine, as well as standing BP. However, if blood pressure is only measured while people are seated upright, cardiovascular disease risk may be missed, as hypertension in supine position on backs is key sign. For patients who had hypertension while supine but not while seated, risks are like those of peers who have hypertension while both seated and supine. These findings suggest people with known risk factors for heart disease and stroke may benefit from having their blood pressure checked while lying flat on their backs. Efforts to manage blood pressure during daily life may help lower blood pressure while sleeping [6].
Blood Pressure Management:
Globally, 2023 Standards update the definition of hypertension for people having more than a systolic blood pressure of 130 mm Hg or diastolic BP of 80 mm Hg. Maintaining BP below 130/80 mm Hg is the recommended strategy for people with hypertension [6]. The practitioners must also keep in mind avoiding hypotension.
The 2023 WHO guideline recommend for the pharmacological treatment of hypertension in adults with a confirmed diagnosis of hypertension and systolic blood pressure of ≥ 140 mmHg or diastolic blood pressure of ≥ 90 mmHg. Latest, from the 2023 ESH guidelines maintain the same BP grade classifications and recommends a threshold of >140/90 mm Hg (grade 1) for the diagnosis of hypertension, whereas the ACC/AHA guideline recommends a lower threshold of >130/80 mm Hg (stage 1 [7].
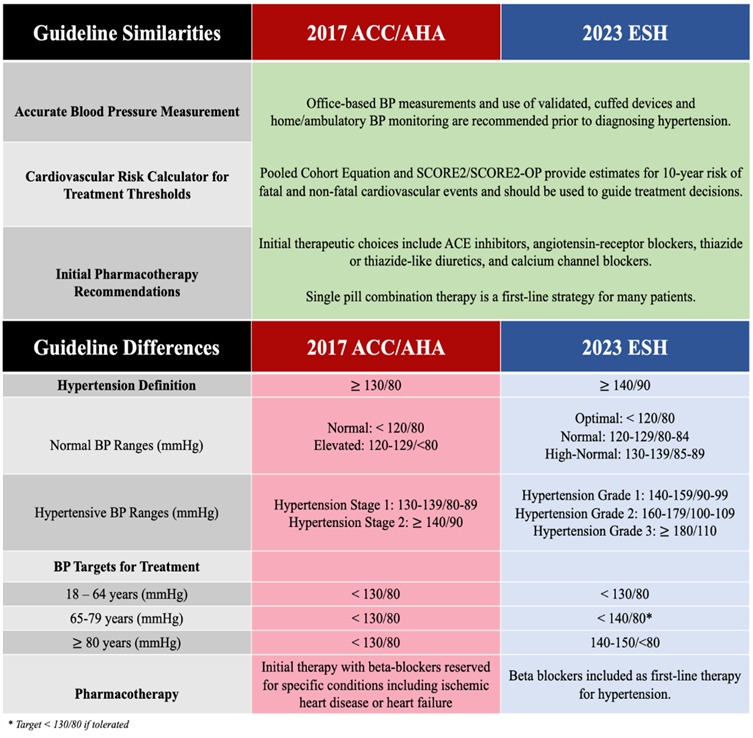
Promotion of lifestyle interventions to prevent, treat, and delay onset of hypertension feature prominently in all guidelines. All the guidelines recommend treatment initiation at higher BP thresholds of SBP ≥140 mm Hg and/or DBP ≥90 mm Hg regardless of calculated cardiovascular (CV) risk or established CVD. For older adults (>80 years of age), the ESH guidelines explicitly recommend drug therapy when SBP is >160 mm Hg. Treatment initiation with antihypertensive agents for patients who have established CVD and BP ≥130/80 mm Hg, and patients who have an estimated 10-year risk of atherosclerotic CVD of >10% should also be started on treatment.

General BP lowering strategy in patients with hypertension:
| Steps | HT with CVD | ||
| 1 | ACEi (ARB if not tolerated) + B blockers- Increase to full dose If tolerated | ||
| 2 | With Angina-Add DHP-CCB | Without Angina add DHP-CB to Diuretic T/TL | |
| 3 | Add further drugs, targeting heart rate<80> | ||
ACEi= Angiotensin-converting enzyme (ACE) inhibitors, ARB= Angiotensin II Receptor Blockers (ARB), DHP= 1,4-dihydropyridine (DHP), CCB= calcium channel blocker
Hypertension being the most risk factor for end stage kidney disease, BP should be monitored and managed with immediate lifestyle management and drug treatment if BP is 140/90 or more, with a primary goal of keeping it under 140/90, if tolerated try to reach 130/80.
Basic approach for OSH/ PHT includes:
Orthostatic /Postural hypotension is common among elderly and diabetic patients. While treating a patient if a practitioner comes across such situations needs to follow:
Neurogenic orthostatic hypotension (nOH):
For nOH Droxidopa (Northera®), orally active synthetic precursor of norepinephrine, is available since 2014.
Hypertension treatment coverage is low in India:
A stepwise simple treatment protocol is lacking and is one of the strategies to improve hypertension treatment in primary care. A study of 281,209 patients initiated on amlodipine 5 mg, 159,292 continued on protocol drugs and came for a follow-up visit during the first quarter of 2022. Of 159,292 individuals who came for the follow-up 70% had controlled BP. respectively, at the first step with amlodipine 5 mg. In the second step with amlodipine 10 mg, the cumulative BP control increased to 75%. A similar 5% (76%–81%) increase was seen in the second step after adding telmisartan 40 mg. Overall, the mean systolic blood pressure (SBP) decreased by 15- 16 from 148 mmHg at the baseline. [5]

India Hypertension Control Initiative (IHCI) Protocol
The reported outcome of the project based on the drug combination was:
| Drugs prescribe in last visit | Follow up Jan-Mach 2022 | % BP Control in recent Jan-March 22 visit | % Cumulative BP Control |
| Amlodipine 5 mg | 146219 | 81.6 | 74 |
| Amlodipine 10 mg | 2617 | 75 | 75 |
| Amlo 5 +Telma 40 | 8492 | 72 | 81 |
| Amlo 5 +Telma 80 | 704 | 64 | 82 |
| Amlo 10 +Telma 40 | 804 | 65 | 77 |
| Amlo 10 +Telma 80 | 347 | 60 | 80 |
| Amlo 10 +Telma 40+Chlo 6.25 | 55 | 69 | 82 |
| Amlo 10 +Telma 40+Chlo 12.5 | 44 | 50 | 79 |
| Amlo 10 +Telma 40+Chlo 25.0 | 10 | 40 | 77 |
Newer drugs:
Aprocitentan is the first endothelin receptor antagonist indicated for treatment of resistant hypertension. It is used in combination with other antihypertensive drugs in adults whose disease is not adequately controlled on other drugs. A dual endothelin receptor antagonist, it inhibits the binding of ET-1 to ETA and ETB receptors. Tab Teveten 600 mg (Erosartan) once daily achieves maximal BP reduction in 2-3 weeks of treatment. Teveten plus (Eprosartan 600 mg + Hydrochlorothiazide 12.5 mg. Research indicate that Aprocitentan is superior to placebo in lowering BP at week 4 (12.5-mg dose, P = .0042; 25-mg dose, P = .0046), with a sustained effect at week 40 (P < .0001). Subgroup analyses in PRECISION showed that the BP-lowering effect of aprocitentan appeared to be consistent irrespective of age, baseline urine albumin-to-creatinine ratio, baseline estimated glomerular filtration rate, body mass index, race, sex, and medical history of diabetes. Researchers also did not observe differences between methods of BP measurement [6].
Ambrisentan, Bosentan, and macitentan are also endothelin receptor antagonists. These agents are indicated for pulmonary arterial hypertension and not for high BP.
A study aimed to analyse the relationship between patients' knowledge and adherence with antihypertensive medication. The researchers found that patient knowledge and understanding of hypertension was associated with improved adherence. A systematic review aimed to investigate the effect of different strategies for medication adherence in patients with hypertension and dyslipidaemia. The researchers found that health education was the most widely used intervention and significantly improved adherence compared with usual care. Other research found that various medication organization strategies were common, but none were associated with improved antihypertensive medication adherence.
Hypertension is defined as a systolic pressure reading of 140 mmHg or more or a diastolic reading of 90 mmHg or more, or those taking antihypertensive medications among persons 18 years of age and over. Between 90-95% of cases are essential hypertension with no identifiable cause. The remaining cases are secondary to a distinguishable process and would resolve if the underlying condition was treated.
Resistant hypertension is defined as hypertension that is poorly responsive to treatment and requires the use of multiple medications to achieve acceptable blood pressure ranges. Primary Care Physicians use the word “Resistant hypertension “when the blood pressure remains above 140/90 mmHg despite optimal use of three antihypertensive medications of different classes, including a diuretic. Globally about 5% of HTN cases are estimated to belong to this category.
The strategies and newer medicines are being tried but no single gold standard is approved as of now. Each approach needs to be given about 3 months’ time to prove efficiency.
Current management strategies include based on the association of Hypertension with the complications identified at the time of first diagnosis, contrary to age old belief of initiating mono-drug therapy initially and adding additional drugs if the response is poor.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
