
Case Report | DOI: https://doi.org/10.31579/2768-2757/038
1Neurosurgery department, Urumia University of medical sciences.
2Neurosurgery department, Tabriz University of medical sciences.
3Neurosurgery department, Tabriz University of medical sciences.
4Student research committee, Arak University of medical sciences.
*Corresponding Author: Amir Kamalifar, Neurosurgery department, Urumia University of medical sciences.
Citation: A Kamalifa, F Salehpour, F Mirzaii, S Kamalifar. (2022). Delay Onset Radicular Pain Due to Vertebroplasty Cement Leakage. Journal of Clinical Surgery and Research. 3(2); DOI: 10.31579/2768-2757/038
Copyright: ©2022 Amir Kamalifar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 December 2021 | Accepted: 31 December 2021 | Published: 10 January 2022
Keywords: vertebroplasty; cement leakage; neurological deficit
Neurological deficit due to Vertebroplasty cement leakage as an important complications with early sign and symptom but delay radicular pain and muscle weakness presentation was rare and need correct diagnostic approach.
Vertebroplasty as an invasive pain reliving procedure in spinal painful osteoporotic fracture ,neurological deficit due to cement leakage less common but serious problem, neurological deficit mostly diagnosis in time of surgery [1] but we can’t find any report of delay neurological deficit due to vertebroplasty cement leakage we report our patient compliant and our approach to him.
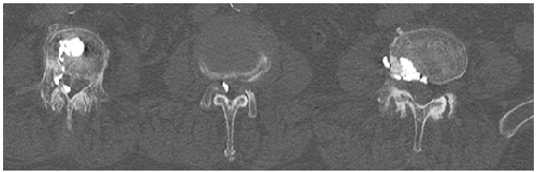
76 years old man visited with sever back pain an evaluated for pain and candidate for vertebroplasty cement injection procedure , no radicular pain and no evidence of root or other neurological involvement , procedure was done under local anesthesia and C- arm fluoroscopy guide in prone position by unilateral transpedicular approach , at the time of surgery patient we can’t find any evidence of cement leakage, patient Paine improve significantly and discharged without any neurological deficit, after 2 month patient return with sever radicular leg pain in left foot and evidence of muscle weakness lower than 4/5 in left foot future MRI showed evidence of root compression in level of L3 look like foreign body other than intervertebral disk , patient go under Ct spiral with thin cut in axial and sagittal reconstruction project showed hyper density particle in spinal canal and foramen( figure 1 ) , density of particle look like vertebroplasty cement density , patient go under standard laminectomy and leakaged cement particle was removed from foramen and spinal canal , patient pain relived rapidly after surgery and muscle strong was improved after 4 month rehabilitation care.
Prior vertebroplasty was done by French radiologist for vertebral hemangioma, after that vertbroplasty was done in many disease but in last decade vertebroplasty turn to main procedure in treatment of painful osteoporotic fracture specially not response to conservative treatment [2], Reported complications of Vertebroplasty include infection, bleeding, transient radiculopathy, spinal stenosis, and pulmonary embolization, cement leakage estimate 30% but neurological deficit was rare( less than 1%) and many of them was diagnosis at the time of procedure [3], delay presentation very rare , but when we diagnosed of leakage additional procedure like open surgery should be considered . golden time of surgery not clearly but many author emphasis on as soon as possible decompression and remove of cement [4], in this specific case patient return with radicular leg pain and muscle weakness after 3 month however open surgery was done and outcome of patient satisfied the surgery team and patient weakness and pain relived completely, correct needle tip location and cement viscosity have major roll in prevent of leakage, experience of surgeon should not be ignored.
Neurological deficit due to vertebroplasty cement leakage rare but seriouse and immediate decompression can improve the prognosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
