
Research article | DOI: https://doi.org/10.31579/2642-9756/105
1Professor, Department of Community Health Sciences, University of Manitoba, Winnipeg, MB, Canada.
2Assistant Professor, Department of Epidemiology and Biostatistics, KLE University, Belgaum- 590010, Karnataka, India.
*Corresponding Author: *Corresponding Author: Shiva
Citation: Shiva S. Halli and Rajeshwari A. Biradar (2022). Declining Son Preference among HIV Infected women in Northern Karnataka, India. J. Women Health Care and Issues. 5(2); DOI:10.31579/2642-9756/105
Copyright: © 2022 Shiva S Halli, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 December 2021 | Accepted: 06 January 2022 | Published: 10 January 2022
Keywords: women living with Hiv/Aids; son preference; karnataka; india
The study examined the sex preference among women living with HIV/AIDS (WLAHs) in Karnataka, India using a representative random sample of 633 women belonging to the age group 15-29 years since a large proportion of the women in India complete their family size before 30 years. The profile of the respondents indicates that the mean age was slightly over 25 years, was largely residing in rural areas and about a half of them were illiterate. There was a very high level of son preference prior to HIV infection. Though the percent of women desired to have a boy or daughter increased after being HIV positive, the results indicate a significant reduction in son preference after being tested positive compared prior to having any child and HIV negative. This could be due to a significant proportion of the WLHAs refine their desired family and sex preference possibly because of the fear of transmission of HIV virus to their child. The WLHAs desire could be healthy children irrespective of sex of the child so that the children do not have to suffer stigma and discrimination if they are HIV positive.
A large number of studies tried to understand the association between HIV status and fertility intentions and fertility outcomes. Lower fertility among HIV-infected women has been observed in women in Zaire, Uganda and Rwanda (Ryder et al., 1991; Allen et al, 1993; Sewankambo et al., 1994) although the studies have generally been too small to yield statistically significant results. Significantly reduced rates of pregnancy were however observed in HIV-infected women in a cross-sectional study carried out in Rakai district, Uganda (Serwadda et al., 1997). Whilst lower fertility rates have also been described in HIV infected women in developed countries (Selwyn et al., 1989; Stephenson et al., 1996; De Vincenzi et al., 1997; Thackway et al., 1997); these are unlikely to be applicable to African populations because, unlike most women in developing countries, the women studied knew their HIV status, and modern contraceptive methods and pregnancy termination were more readily available and acceptable.
The reduced fertility observed among HIV–infected women might be due to fear of transmission to their children. However, recent developments of preventing parent-to-child transmission (PPTCT) might have encouraged HIV-infected women to consider childbearing and enjoy motherhood. Unfortunately, not many large-scale quantitative studies are conducted using random samples, and available studies are mostly clinical in nature trying to understand the reproductive effect of HIV/AISDS on ability to conceive and pregnancy outcomes. Hence, there is no good understanding of impact of HIV/AIDS on reproductive health care needs and fertility desires. In case of India, with the exception of study by Biradar et al., (2019) using the same data set that we are using for this study, we come across a qualitative study conducted in Tamil Nadu, India. This study throws some light on fertility desires, intensions and fertility decision making including the barriers women living with HIV/AIDS (WLHA) face in achieving their intended family size. The main barriers mentioned by the women, it seems, lack of family support, stigma and discrimination by the family members, anxiety about child rearing in case of their death and importantly the lack of knowledge about PPTCT (Halli et al., 2016). The authors are aware that their results based on qualitative study may not be generalizable and hence, suggested further research among WLHA in order to assist evidence-based policy development so that WLHA can exercise informed choices to fulfil their desired family size and sensitise health care providers about their needs.
Till date, studies have shown that HIV infection may affect fertility by influencing desires and intentions for having children. On the other hand, studies of fertility intentions among HIV-positive individuals have found mixed results mainly because of socio-cultural contexts and individual factors. It may be easier to the unmarried women to exercise their reproductive choices compared to married women who be pressurized by their husbands (Cooper et el., 2007). Even if there are some studies indicating that there is a relationship between perceived HIV risk and fertility desires among unsure women about their HIV status, however, the nature and magnitude of HIV effect is not clear. In fact, some studies using qualitative or correlation analysis found mixed results about the nature of relationship between HIV risk and fertility (Baylies, 2000; Yeatman, 2009; Moyo and Mbizvo, 2004; Rutenberg et el., 2000). It is also possible that WLHA may be worried that their children may become orphans if they perceive that their children have higher risk of dying because of their HIV infection (Grieser et al., 2001). Grieser et al., (2001) in their study in Zimbabwe also found that even if WLHA perceive higher mortality for their children because of their HIV status, yet they may not want to have more children in order to replace their children who have died. However, Gyimah and Rajulton (2004) in Ghana and Gyimash and Obeng (2004) in Kenya found women living with HIV/AIDS wanting to have more children in order to insure for possible negative impact on their children survival due to their HIV/AIDS status.
Like other women, WLHA have been arguing for their sexual and reproductive rights (Cooper et al., 2003; Sachin et al., 2009); and in their study in Brazil, Segurado and Paiva (2007) observed that HIV positive men may want to have more children and their desire might have been influenced by the prevailing socio-cultural context. Similarly, studies conducted elsewhere including India found that a HIV positive woman cannot decide unilaterally about her family size, and her spouse as well as other family members may be involved in deciding the family size because of cultural norms (Kanniappan et al., 2008; Sachin et al., 2009; Ko and Muecke, 2005; Oosterhoff et al., 2008). Other studies highlight economic factors by arguing children as future resource and economic security (Dyer et al., 2002; Dyer et al., 2008; Speizer & White, 2008; Ujiji 0, 2010). Interestingly, Biradar et al., (2019) observed other factors for deciding the family size by WLHA such as broader health system factors, influence of health care providers as well as stigma and discrimination.
Indians’ preference for sons over daughters is well known phenomenon (Dyson and Moore, 1983). In fact, this was also concern of British empire in India because of sex ratios in favour of males and practice of female infanticides (Miller, 1981). The recent publication of UNFPA on son preference in India include financial and emotional care especially in the old age of parents, burden of daughters because of widespread practice of dowries, family lineage and religious rites (Pande and Malhotra, 2006). This is true of general population in India but does it also apply to the couples who are HIV positive? In particular, how do factors that signal HIV and AIDS status influence the son preference-do HIV infected couples’ preferences become more gender egalitarian or does HIV status offer couples more efficient ways to implement unchanged gender-based preferences? A relevant question to millions of couples living with HIV in India is how they perceive daughters given the culture of strong son preference? An attempt is made in this study to throw some light on sex preference using the specially collected quantitative data on fertility attitudes and intensions in Northern Karnataka, India.
The study is conducted in 2012 in Bagalkot district of Northern Karnataka and it is a cross-sectional quantitative survey of 630 currently married HIV positive women selected using a stratified random sampling method. Since the study focuses on fertility intentions, the sample is limited to women aged between 15-29 years. Because the study is aimed at examining the fertility intentions of women living with HIV/AIDS (WLHA), the population universe consists of the women who know their HIV status. In Karnataka, people test for HIV in government facilities ie., integrated counseling and testing centers (ICTC). While the ICTC data would represent an ideal sampling frame for the study, it is highly confidential and hence not available. However, the large majority of the people who undergo HIV testing and test positive are members of the DIC+ in a district, one such DIC+ is Jeevana Jyothi-DIC+ in Bagalkot district where large proportion of the positives register. Moreover, this is the district, where the HIV prevalence in the state and in the country is highest. As access to the database from Jeevana Jyothi-DIC+ can be obtained for research purposes, the study used the database of DIC+ as a sampling frame.
Since the study population belonged to the most vulnerable group, an ethical clearance was obtained from the WHO’s Research Ethics Review Committee and Institutional Ethical Review Board of St John’s Medical College, Bangalore, Karnataka. Complete anonymity was maintained on the HIV status of the women and interviewers were given only the names and addresses without any mention or reference to the status. The research team kept the list strictly confidential and once the field work was completed, the list was shredded. No mention of names and addresses of the participants was recorded anywhere, including in the data.
The analysis was conducted using IBM’s Statistical Package for the Social Sciences (SPSS) version-20.0. Bivariate analysis was conducted to describe and understand the association of background characteristics with preference for sons and daughters using the model Chi-square. The multivariate logistic regression was used to assess the individual risk of the background characteristics after adjusting for the remaining characteristics.
The study recruited and interviewed a total of 633 respondents keeping in mind the objectives of the study. Appendix 1 is included to provide profile of the respondents. Of the 633 respondents interviewed after informed consent, 27% were less than 25 years with a mean age of about 26 years. Over 71 % were from the rural areas, about half of them were illiterate and 45% of the respondent’s husbands were illiterate too. Most of the respondents were from Hindu religion (94.5%), and 42
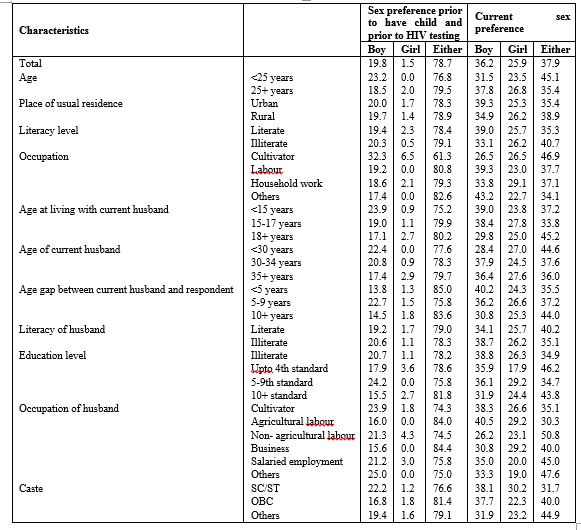
Examining the sex preference by characteristics of the respondents, Table 1 shows that the sex preference increased at present as compared to a time when having no child or not HIV positive. While younger one had a higher sex preference before, at present older respondents prefer to have the sex of the child, particularly boys. Interestingly urban and literate respondents seem to have higher sex preference as compared to their counterparts. Those started living with the husbands at younger age, husbands are older and age gap between respondent and husband is shorter were more likely to have preferred sex compare to their counterparts. The table also shows that the preference for both boys and girls increased as compared to earlier and the gap between percent preferred a boy and girl narrowed at present. The study therefore, suggest that though a large percent prefer both boys and girls, the narrowing of the percent between those preferring a boy and girl indicates that the sex preference probably is reduced since the HIV infection.
The study further assessed the changes in the desired family size at present compared to the time when the respondent was HIV negative and had no child. Figure 3 shows that the mean number of boys preferred reduced marginally, whereas the same increased for girl child. High level of sex preference was noticed prior to have any child and was HIV negative. The sex preference desired was 1.07 boys against 0.77 girls. However, after being tested HIV positive, the sex preference reduced and mean number of boys and girls desired was 1 boy, 0.9 girl child and 0.1 child of either sex. Further the gap between mean number of boys and girls reduced at present further suggest the reduced sex preference among women living with HIV.
The study examined the sex preference among women living with HIV/AIDS in Karnataka, India. The respondents selected in the study were young married women living with HIV and were selected from the district of Bagalkot. The profile of the respondents indicates that the mean age was slightly over 25 years, was largely residing in rural areas and about a half of them were illiterate. Though over 95% had an electrified house, 77% used open areas for defecation and large proportion was engaged in agricultural work. The district is one of the districts with very low Human Development Index in the state, though in the mean household income of the respondents (Rs 7300/-) suggest that the women had much better income as compared to the population in the district.
The number of children ever born among positive women was 2.15, which is more or less same as the reported fertility levels in the district as the mean children ever born to women aged 20-24 and 25-29 years was respectively 1.75 and 2.57 in the state (DLHS-2, 2007-8). The study also showed that about 93% of the children ever born surviving (2.01 children surviving among 2.15 ever born. Overall, 29% respondents had a child death with an average of 1.25 children died suggests that a large proportion of the positive women experience child deaths. The child death is relatively high among these respondents, and possibly the young age at start of living with husband.
There was a very high level of sex preference prior to HIV infection, and boys have been often preferred, though a significant proportion also was undecided on the child’s sex. Though the percent women desired to have a boy or daughter increased at present compared to the desired family size before being positive, the reduced gap between preference of boys and girls suggests a reduced sex preference for boys since tested positive. That is, the study noticed a significant reduction in sex preference among respondents after being tested positive as compared to prior to having any child and was HIV negative. While younger women had a higher sex preference before, at present older respondents prefer to have the sex of the child, particularly boys. Interestingly urban and literate respondents seem to have higher sex preference as compared to their counterparts. Those started living with the husbands at younger age, husbands are older and age gap between respondent and husband is shorter were more likely to have preferred sex compare to their counterparts.
The reduced sex preference among the WLHAs may be due to higher prevalence of pregnancy wastage and child death because 28% of the women started living with the current husband before the age of 15 years and 73% respondents started living with the current husband before they are 18 years. Hence, HIV positive women may just want healthy children irrespective of the sex. Other researchers using the same data have also shown that 17% respondents experienced a still birth or abortions, 37% percent experienced at least 2 still births or abortions, indicating higher rate of multiple pregnancy wastages among the respondents (Isac et al., 2017). Large proportion of the pregnancy wastage was as a result of spontaneous abortion (81%), though 22% and 17% of the respondents respectively experienced pregnancy wastage as a result of still birth or induced abortion respectively. Overall, 29% respondents had a child death with an average of 1.25 children suggests that a large proportion of the positive women experience child deaths. Surprisingly, WLHA living in urban areas and educated have shown higher preference for sons, this seems to contradict UNFPA study showing women’s education as the single most significant factor in reducing son preference (Pande and Malhotra, 2006). Since, the WLHAs are likely to be “afraid of HIV transmission to their children”, it is possible that urban and educated WLHAs may be aware of the PPTCT (prevention of mother-to-child transmission) facilities in the state.
IMPLICATIONS
Despite the risks associated with pregnancy, our data suggest that HIV-infected women are likely to become pregnant to achieve their desired family size. However, like other mothers, it is quite natural among the WLHA desiring healthy babies and prevent vertical transmission. The policy makers should be sensitive to Indian socio-cultural context where childbearing is encouraged and hence, WLHA should have the same rights and privileges like other women. Based on the findings of the study, Biradar et al., (2019) argue that WLHA might be reluctant to discuss fertility intensions with health care providers because of possible negative reactions. Before WLHA’s making any decision about their fertility intensions in including the decision about their sex preference, they should be encouraged to discuss with health care providers. It is possible that prevention of perinatal transmission programs in combination with ART may alter women and men's attitudes in favour of childbearing. The findings of this study seem to suggest the need for explicit policies recognizing reproductive rights and choices of WLHA. The HIV/AIDS policies especially in northern rural districts of Karnataka where HIV prevalence is much higher should have health counselling services informing the available PPTC services and healthier reproductive options. Moreover, decision-making about pregnancy may be complicated for people living with HIV, as other factors play an important role in reproductive decisions. People living with HIV are often stigmatized. Lack of adequate parenting resources may also be common, especially among women with HIV living in poverty and belong to SC/ST and other backward castes.
Declarations
Ethics approval
Since the study population belonged to the most vulnerable population, an ethical clearance was obtained from the WHO’s Research Ethics Review Committee and Institutional Ethical Review Board of St John’s Medical College. Complete anonymity was maintained on the HIV status of the women and interviewers were given only the names and addresses without any mention or reference to the status. The research team kept the list strictly confidential and once the field work was completed, the list was shredded. No mention of names and addresses of the participants was recorded anywhere, including in the data. The data is password protected
Conflict of interests
The authors have no conflicts of interest to declare.
Funding
This study received no specific grant from any funding agency, commercial entity or not-for-profit organisation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
