
Mini-Review | DOI: https://doi.org/10.31579/2692-9406/028
*Corresponding Author: Muhammad Shariq Mukarram, Department of Internal Medicine, Jinnah Medical College Hospital, Karachi, Pakistan.
Citation: Muhammad I Ghauri, Muhammad S Mukarram, Jibran S Muhammad. (2020) Debate on the Effectiveness of Hydroxychloroquine for Treatment of Coronavirus Disease 2019 (COVID-19). Biomedical Research and Clinical Reviews. 1(5); DOI:10.31579/2692-9406/028
Copyright: © 2020 Muhammad Shariq Mukarram, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 October 2020 | Accepted: 14 November 2020 | Published: 18 November 2020
Keywords: sars-cov-2; covid-19; hydroxychloroquine; rheumatic diseases
The recent outbreak of Coronavirus disease (COVID-19) caused by novel SARS-CoV-2 has raised global health concerns putting many lives at stake. Such condition calls for an urgent demand for effective, available and affordable drugs to control the viral illness. Several different therapies are under study and no definite treatment has yet been approved. Hydroxychloroquine, an antimalarial agent with immunomodulatory and anti-viral properties, remains the hot topic of discussion. The drug has demonstrated potent in vitro activity against SARS-CoV-2. This article presents a review of published literature from the year 2020 (Jan-Apr). This aimed article aimed to review the effectiveness of Hydroxychloroquine in treating patients with COVID-19. Based on the available literature, we recommend the use of this agent in treating patients with active SARS-CoV-2 infection.
The first case of the Coronavirus was reported in Wuhan, the largest metropolitan city in China’s Hubei province on 30th December 2019. Prompt measures were taken by the Centre for Disease Control and Prevention (CDC) and the Chinese health authorities. This illness was temporarily named as the 2019 novel Corona-virus (2019-nCOV) by the World Health Organization (WHO). After the release of the first whole-genome sequence on the 10th of January 2020, researchers were quickly able to identify the viral illness in patients using reverse-transcriptase polymerase chain reaction (RT-PCR). Before this, the initial cases were classified as “Pneumonia of unknown origin”. Researchers found that this virus belongs to the beta coronavirus group, similar to SARS Coronaviruse. On February 12th 2020, the WHO named this pathogen as SARS-CoV-2 and the disease caused by it as Coronavirus disease 2019 (COVID 2019). Unfortunately, on 11th March 2020, COVID -19 was recognized by WHO as a pandemic spreading to over 150 countries [1-2].
We used the MeSH terms “Pandemic”, SARS-CoV-2” and “COVID-19” with “Hydroxychloroquine” and “rheumatic diseases” to search the scientific databases such as SCOPUS, PubMed and Google Scholar. A total of 12 studies were included in the review.
Structure of Coronavirus
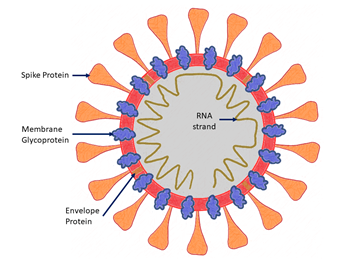
Coronaviruses are single-stranded RNA viruses. SARS-CoV-2 is classified under the beta Coronaviruses group. The genetic framework of the virus consists of a 5’-untranslated region (UTR), a replicase complex encoding non-structural proteins (NSPS), a spike protein (S) gene, an envelope protein (E) gene, a membrane protein (M) gene, neucleocapsid protein (N) gene, 3’-UTR and multiple unidentified non-structural open-reading frames (figure 1a). Owing to the presence of its spike glycoprotein on the envelope, it has a crown-like appearance on electron microscopy [1-3].
Transmission
Human to human transmission of the virus has well been established with the symptomatic population being the most frequent source of the spread. The possibility of transmission of the disease before the development of symptoms seems to be infrequent. The incubation period varies between 3 to 7 days and may prolong up to 2 weeks. Data from the first cases from Wuhan and investigations conducted by CDC china showed that the viral illness doubled every 7 days, whereas the basic reproduction number is 2.2. Close contact is necessary for the spread of SARS-CoV-2 and therefore, family members and health care workers are at higher risk. This is why; the use of isolation has been suggested as the best way to contain the ailment [2].
Besides that, SARS CoV-2 can also infect the human gastrointestinal tract, therefore fecal-oral spread is likely to occur from the viral disease [4].
Clinical features and diagnosis
Common clinical features of COVID-19 include fever (80-90%) along with respiratory symptoms; dry cough (48-76%) and shortness and breath (30-55%). Other frequent characteristics include loss of appetite, productive cough, less commonly headache, diarrhea, nausea and vomiting [4].
Clinical diagnosis is based on symptomatology and exposure history, along with chest image findings. Definite diagnosis requires the detection of the virus using the PCR technique. The virus can be found in the upper respiratory tract in nearly all patients therefore, nasopharyngeal and oropharyngeal swabs are preferred samples [4].
Treatment options
Searching for effective therapies for COVID-19 infection is a complex process. No drugs have been approved for the prevention or treatment of COVID-19. Numerous agents are being investigated as potential therapies. Amongst these, few are those that were previously used to treat SARS and MERS outbreak [5-6].
Chloroquine and Hydroxychloroquine:
These agents have a long-standing history in the treatment and prophylaxis of malaria and the treatment of chronic rheumatic diseases [7]. Chloroquine and hydroxychloroquine block the entry of the virus into cells by inhibiting glycosylation of host receptors and endosomal acidification, as discussed in detail ahead [8-9].
Lopinavir/Ritonavir:
This is an oral combination, approved by the US food and drug administration, used to treat HIV infection. It has demonstrated in vitro activity against other novel coronaviruses through inhibition of 3-chymotrypsin like protease [10-11]. However, no published data exists for Lopinavir/Ritonavir with in vitro activity against SARS-CoV-2 [12].
Ribavirin:
Ribavirin is a guanine analog that inhibits viral RNA-dependent polymerase. It is also active against other novel coronaviruses. Itsin vitro activity against SARS-CoV-2 is very limited and required very high doses (1.2-2.4g every 8 hours) to inhibit the viral replication. Adverse effects including hematologic and hepatotoxicity were common [5].
Oseltamivir:
Oseltamivir is a neuraminidase inhibitor approved for treatment in Influenza. Unfortunately, this agent has no documented in vitro activity against SARS-CoV-2 [13].
Umifenovir:
This anti-viral agent targets the S protein/ACE2 interaction and inhibits the membrane fusion of the viral envelope. This unique mechanism of action makes it a promising drug for the treatment of COVID-19 and is currently under different trials [14].
Remdesivir:
Remdesivir is a monophosphate pro-drug that undergoes metabolism to C-adenosine triphosphate, an active analog. Due to its low EC50 and host polymerase selectivity against the Ebola virus, the first clinical use of Remdesivir was for Ebola during the Ebola virus outbreak [15-16]. Owing to its broad spectrum and potent in vitro activity against several novel coronaviruses including SARS-CoV-2, this agent is a promising potential therapy for COVID-19 [17-18]. Successful case reports have been reported, describing the use of Remdesivir in the treatment of COVID-19 [19-20].
Molecule and uses of Hydroxychloroquine
Hydroxychloroquine is a derivative of Chloroquine and is a 4-aminoquinoline with three distinct properties: immunosuppressive, anti-autophagy, and anti-malarial activities. This drug suppresses the immune system by interfering with the processing and presentations of antigens and cytokine production. It also raises the pH within the lysosome, impairing the autophagic degradation of the protein. It alters the assembly of macromolecules in the endosomes and post-translation modification of proteins in the Golgi apparatus. Furthermore, it is highly active against the erythrocytic stage of Plasmodium Vivax, Malariae and most strains of Falciparum. Hydroxychloroquine is now most often used as an anti-rheumatological agent in Systemic Lupus Erythematosus (SLE) and Rheumatoid arthritis [21].Hydroxychloroquine, apart from being less toxic than Chloroquine is also more soluble owing to the presence of its N-hydroxyethyl side chain instead of N-diethyl group which is present in Chloroquine [22].
Anti-viral property of Hydroxychloroquine
The spike protein of SARS-CoV-2 interacts strongly with the human ACE2 receptor [1]. The virus uses this receptor to enter the cells. Hydroxychloroquine is known to be a weak base that elevated the pH of intracellular organelles, as discussed above. It inhibits the entry of SARS-CoV-2 by modifying the glycosylation of the ACE 2 receptor and spike protein [23-24].Increased levels of Interleukin 6 and Tumor Necrosis Factor-alpha have well been documented in different viral infections like Hepatitis C virus, Hepatitis B virus, Influenza virus, Chikungunya virus and most importantly the Severe acute respiratory syndrome virus (SARS-CoV-2) [25-28]. Hydroxychloroquine has a regulatory effect on activated immune cells. It reduces the production of cytokines, Interleukin 1 and Interleukin 6, through macrophages by down regulating the expression of Toll-like receptors, inhibiting T and B cell receptors [22, 29, 30]. This pro-inflammatory status has provided the rationale for the use of Hydroxychloroquine as a potential treatment option in COVID-19.
Importantly, the lung is the major organ affected in COVID-19. Hydroxychloroquine has a wide distribution in the lung where the drug concentration reaches a hundred times more than that in blood. Due to this property, enough concentration can be achieved for its inhibitory effects on the lungs [41].
Treatment of COVID-19 with Hydroxychloroquine
The first study on the effect of Hydroxychloroquine on CIVID-19 was conducted by Philippe Guatret where patients were given the drug in a dose of 200mg thrice a day. There had been a rapid fall of the nasopharyngeal viral load. The study indicated that Hydroxychloroquine might be effective against COVID-19 [31]. However, it is reported to have several limitations; a small population with only 2 patients who received Hydroxychloroquine (6 of whom received Azithromycin), the observation period of 6 days was very short, no randomization was done [32]. The viral clearance was superior in patients receiving Hydroxychloroquine plus Azithromycin (100%) compared with Hydroxychloroquine monotherapy (57%) [33].
The second French study conducted by Guatret was relatively larger but it lacked a control group. These patients were given Hydroxychloroquine 200mg every 12 hours. The overall clinical outcome was similar to that of patients with COVID-19 who did not get any treatment [32, 34].In a trial of 30 patients carried out by Jun Chen and his colleagues, the efficacy of Hydroxychloroquine was compared to local standard care. No major difference was found in the nasopharyngeal viral carriage on the 7th day of the trial [35].
Hydroxychloroquine (200mg every 12 hours) in a randomized control trial of 62 patients was associated with a shorter recovery time in patients suffering from a milder form of the disease [36].
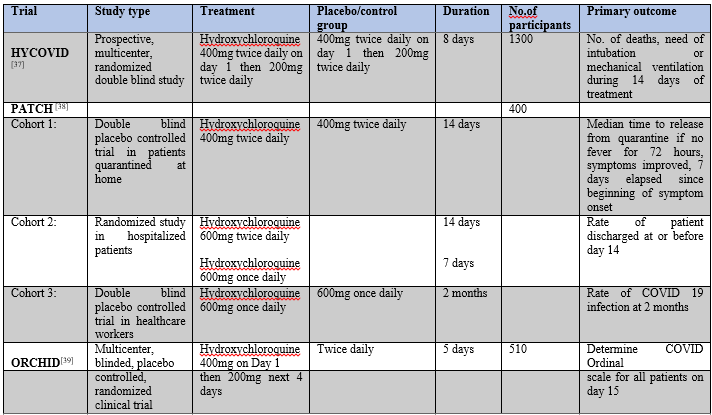
Interestingly, a physiologically based pharmacokinetic modeling study has recommended a treatment regimen of Hydroxychloroquine in COVID 19 in a loading dose of 400mg twice daily on day 1 followed by 200mg twice daily [41]. Few large scale clinical trials are planned and registered for evaluating the efficacy of Hydroxychloroquine in COVID-10; HYCOVID trial (NCT04325893) [37], PATCH trial (NCT04329923) that consists of 3 cohorts determining the role of the drug in COVID-19 positive patients quarantined at home, hospitalized and health care workers [38], ORCHID trial (NCT04332991)[39] (Table1a)
Old aged patients with multiple comorbidities are at a higher risk of acquiring the SARS-CoV-2 infection. In A case report of a 72-year old patient with a heart transplant who was receiving immunosuppressive therapy tested positive for the disease. He had interstitial pneumonia at the time of diagnosis. The patient was commenced on Hydroxychloroquine therapy with no further declination in his clinical status. After 12 days of hospitalization he tested negative for SARS-CoV-2 and was completely asymptomatic [40].
Yao et al tested the effect of Chloroquine and Hydroxychloroquine in vitro. Their study was divided into two groups; treatment and prophylaxis. They compared the half-maximal effective concentration, EC50, of these two drugs at different time intervals. In the treatment group, the EC50 values of Chloroquine were 23.9µM and 5.47µM at 24 and 48 hours; while those for Hydroxychloroquine were 6.14µM and 0.72µM at 24 and 48 hours, respectively. Based on these marked differences between the EC50 values, they concluded that Hydroxychloroquine is more effective in vitro than Chloroquine for the treatment of COVID-19 [41].
Safety profile of Hydroxychloroquine
Treatment with Hydroxychloroquine is generally well tolerated by patients and the adverse effects are usually dose and duration related. Common side effects include mild dermatological, gastrointestinal and neurological features. Less common adverse effects include retinopathy and cardiac arrhythmias (prolonged QT interval) [42]. With the usual dose (≤5mg/kg) retinopathy occurs in up to 3.5% of patients taking Hydroxychloroquine [43].
Although not frequent, a case of severe hepatotoxicity resulting from the use of Hydroxychloroquine has been reported in a patient with severe SARS-CoV-2 infection. After the commencement of the therapy, serum transaminase levels raised 10 times that of normal, which declined rapidly after the withdrawal of the drug [44]. Nevertheless, as proven by various studies, the overall toxicity and side effect profile of Hydroxychloroquine is quite less, making it a relatively safer drug to use. Jun et al reported adverse events in 4(26.7%0 patients who received 400mg of Hydroxychloroquine per day and in 3 (20%) patients in the control group [45]. In another study as reported by Chen at el, 2 patients experienced very mild reactions in the treatment arm after being treated with Hydroxychloroquine (400mg/day) for 5 days [36]. Guatret et al, reported mild side effects that included blurring of vision in 1.2%, diarrhea in 5% and vomiting in 5% of patients [31].
COVID-19 in patients with Rheumatic diseases
Hydroxychloroquine has been famous as a potential treatment option in different rheumatic diseases, mainly Rheumatoid arthritis and Systemic Lupus Erythematosus (SLE). Hence, the relationship between the occurrence of COVID-19 in patients with rheumatic diseases in an interesting topic, especially for the rheumatologists.
A case series conducted in Lombardy Italy, on patients with chronic rheumatic diseases (rheumatoid arthritis and Spondyloarthropathy) who were being treated with targeted synthetic disease-modifying anti-rheumatic drugs (DMARDs) and biological DMARDs. Information was collected from 320 patients. Out of these, 4 were confirmed cases of COVID-19 diagnosed through nasopharyngeal swab, and 4 were highly suggestive of COVID-19 on clinical grounds. Overall, 5 patients were on previous treatment with Hydroxychloroquine. DMARDs, except Hydroxychloroquine, were withdrawn from all patients with symptoms of the illness. None of the patients developed respiratory complications or died except for 1 patient who required low flow oxygen for a few days. Nevertheless, in 3 of 8 symptomatic patients who were taking Hydroxychloroquine, it did not seem to the prevent occurrence of infection in these cases [46]. No definite conclusion can be drawn from such a small population of patients regarding the incidence of COVID-19 in patients with chronic rheumatic diseases taking Hydroxychloroquine, a high surveillance with a strict follow up is required. However, the preliminary experience shows that patients treated with DMARDs, mainly Hydroxychloroquine, do not seem to be at a high risk of respiratory or life-threatening complications from SARS-CoV-2 when compared to the general population.
Little evidence can also be taken by the fact that there is no case of SLE identified with COVID-19, as stated by Joob in a comment [47]. Even so, this might only be a matter of time researchers learn about SLE patients with COVID-19. Nonetheless, corroboration otherwise is also available. A 61-year old female who has been a known case of Rheumatoid arthritis for last the 3 years and achieved disease remission with Leflunomide and Hydroxychloroquine was positive for COVID-19. Her only initial symptoms were myalgia and fever for 4 days. Her symptoms worsened 3 days after her admission and she developed pneumonia. The patient later improved after discontinuation of her conventional DMARDs (except Hydroxychloroquine) and the addition of anti-viral agents [48].
Interestingly, a recently published paper explains the mechanism of epigenetic dysregulation that could not only put patients with SLE at an increased risk of COVID-19 but also cause a severe form of the disease, regardless of the immunosuppressive therapy these patients are taking. There are hypomethylation and overexpression of ACE 2 in patients with SLE, which encodes the receptor for SARS-CoV-2 spike protein. This potentiated the entry of the virus into the cells. Furthermore, viral infections induce oxidative stress that would exacerbate the DNA methylation defect, perpetuating the mechanism. Similar modifications to interferon regulated genes would also exacerbate the immune reaction to SARS-CoV-2 in such patients [49].
The preventive role of Hydroxychloroquine in patients with rheumatic diseases taking the drug chronically is a currently unresolved issue that needs an extensive and detailed evaluation.
Conclusion and recommendations
After analyzing the current literature and available studies, we concluded that the anti-viral properties of Hydroxychloroquine have demonstrated in vitro activity against SARS-CoV-2 with promising results. In our opinion, the use of this agent in treating SARS-CoV-2 infection is safe. Considering the potential efficacy, low priced, easy availability, and reduced risk of toxicity, we recommend the use of Hydroxychloroquine in patients with COVID-19. The results of the clinical trials reviewed here showed that Hydroxychloroquine is efficacious in the treatment and supportive care of COVID-19 patients. However, to obtain the highest grade of evidence results from large, multicenter, double-blinded studies are required
Conflicts of interests
None declared by any of the author
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
