
Research Article | DOI: https://doi.org/10.31579/2692-9562/121
1Department of Pediatric Dentistry and Community Oral Health, College of Dentistry, University of Tennessee Health Science Center, 875 Union Ave, Memphis, TN, 38163, USA.
2Department of Bioscience Research, College of Dentistry, University of Tennessee Health Science Center, 875 Union Ave, Memphis, TN, 38163, USA.
#These authors contributed equally to this work.
*Corresponding Author: Yanhui Zhang, Department of Bioscience Research, College of Dentistry, University of Tennessee Health Science Center, 875 Union Ave, Memphis, TN, 38163, USA. Email: yzhang36@uthsc.edu
Citation: Casey Filbert, Jennifer Lou, Martha H. Wells, et al, (2024) Cytotoxic Effects of Three Dental Cements on Human Oral Cells, Journal of Clinical Otorhinolaryngology, 6(4); DOI:10.31579/2692-9562/121
Copyright: © 2024, Yanhui H Zhang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 April 2024 | Accepted: 02 May 2024 | Published: 10 May 2024
Keywords: dental materials; MTT; cytotoxicity; pediatric; zirconia crown; cement
Background/Aim: Pediatric zirconia crowns require a passive fit, which leads to open margins where dental cement is in intimate contact with tissues of the gingival sulcus. This study assessed the cytotoxicity of three dental cements on human gingival fibroblasts and epithelial cells using the MTT assay.
Materials and Methods: Three cements were tested: 1) BioCem, 2) RelyX Unicem-2, and 3) Ketac Maxicap. Controls were Dulbecco's Modified Eagle Medium (DMEM) (negative control), and 0.1% Triton-X (TX-100) (positive control). 5 mm x 2 mm cement discs were prepared and incubated in DMEM medium for 24 hours at 37°C. GN 23 fibroblasts or SG epithelial cells were cultured in 96 well plates overnight, and then treated with sterilized cement extract for 24, 48, or 72 hours. Then added MTT for 4 hours, solubilized for 1 hour, and the absorbance was measured at 570nm. A two-way ANOVA was conducted, followed by Student-Newman-Keuls Method
Results: Cytotoxicity on GN 23 cells (n=64): 24h: TX-100>Ketac=BioCem>RelyX=DMEM; 48h: TX- 100>Ketac> BioCem=RelyX> DMEM; 72h: TX-100>Ketac>BioCem=RelyX> DMEM. Cytotoxicity on SG cells (n=32): 24h: TX 100>Ketac= BioCem=RelyX=DMEM; 48h: TX-100>Ketac> BioCem=RelyX>DMEM; 72h: TX 100=Ketac>BioCem>RelyX>DMEM. P <0.05 was considered statistically significant.
Conclusions: Ketac showed the greatest cytotoxic effects. BioCem showed no significant difference from RelyX on GN 23 and SG cells at 48h, 72h and 24, 48h, respectively.
As society becomes increasingly concerned with esthetics it has become more common for parents to request esthetic restorations for their children. Pediatric dentistry has responded to these demands with multiple esthetic full-coverage options including composite strip crowns, pre-veneered stainless-steel crowns (SSC), open-faced SSC, and most recently, pre- fabricated zirconia crowns [1]. Zirconia crowns are unlike their stainless- steel counterpart in that they are unable to be manipulated to fit intimately against the tooth surface. Manufacturer instructions require a “passive fit” of the crown on the tooth before cementation which inevitably leads to open margins where the cement is in direct contact with the surrounding tissues [2- 4]. No dental material meets all requirements to be considered an ideal restorative material. A practitioner must weigh the benefits and risks of each restorative material. The evaluation of the cytotoxicity and biocompatibility of a material is as important as its physical or mechanical properties [5-7]. Much of the existing research on the cytotoxicity of dental cements has been performed using mouse L929 standard cell line or bovine cell lines [8]. The purpose of this study was to compare the cytotoxicity of three dental cements on more clinically relevant human gingival fibroblasts and human gingival epithelial cells in vitro. Three types of cements were tested: a traditional glass ionomer cement, a self-adhesive resin cement, and a bioactive cement which is a new material. Traditional glass ionomer cements (GIC) were invented in 1969 and reported in the early 1970s [9]. They are materials made of calcium or strontium aluminoflurorsilicate glass powder (base) that combine with a water-soluble polymer (acid) [10]. When the two components are mixed together, they undergo a setting reaction involving neutralization of the acid group by the powdered solid glass base [10]. One benefit of GIC is the release of fluoride ions during both the setting reaction and for extended amounts of time afterwards [10].
Self-adhesive resin cements were developed as alternatives to the traditional cementation options of conventional resin cement and resin modified glass ionomer cements. Originally, these cements combined technologies from glass ionomer materials, adhesives, and composite cements to create a universal cement appropriate for a long list of indications [11]. Unlike traditional resin cements, self-adhesive resin cements do not require the etch/prime/bond system before cementation. To eliminate the need for etching, priming, and bonding, this material was formulated with phosphoric acid-modified methacrylate monomers, which enable the cement to self- adhere to the tooth surface [11].
The newest of the cements studied are bioactive cements. They were developed to release calcium, phosphate, and fluoride ions. They also have unique bioactive properties that form hydroxyapatite, which is available to integrate with and replenish tooth structure. BioCem (NuSmile, Houston TX), is a hydrophilic resin modified glass ionomer cement that is similar in chemical and structural composition to dentin and contains no HEMA, Bis- Phenol A, BiSGMA or BPA derivatives [12].
Cell Lines
A human gingival fibroblast cell line (GN 23) derivedfrom a healthy patient with non-inflamed gingiva was used in this study [13]. The human gingival epithelial cell line (SG) used in the present study was obtained from F. H. Kasten, East Tennessee State University, QuillenCollege of Medicine, Johnson City, TN [14]. The cells were cultured in complete Dulbecco’s Modified Eagle Medium (DMEM) at 37°C in a humidified atmosphere of 5% CO2 in the air. Complete DMEM is supplemented with 10.
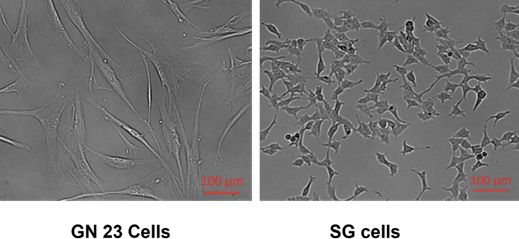
Figure-1: Cell lines used in this study.
Cements
Cements tested for cytotoxicity in this study were: 1) RelyX Unicem (Self- Adhesive Resin Cement, 3M, St Paul, Minnesota) 2) NuSmile BioCem (Universal BioActive Cement, NuSmile, Houston, TX) and 3) Ketac Cem Maxicap (Glass Ionomer Cement, 3M ESPE, St. Paul, MN).
Preparation and Curing of Cement Extracts
Cement specimens were prepared and then cured following the ISO standards and manufacturers’ recommendations (Table 1) [11,12,16,17].
| Cement | Curing instruction |
| RelyX UnicemUltimate Adhesive ResinCement | Light-cure eachsurface for 20 seconds, for a totalof 40 seconds. |
| BioCem Universal BioActive Cement | Light-cure for 40 seconds |
| Ketac CemMaxicap™Glass Ionomer Cement | Self-cure for 7 minutes |
Table 1: Manufacturer’s Curing Instructions
They were prepared using 5mm diameter and 2mm thick cylindrical molds, seated on a glass plate. Specimens requiring a light cure (RelyX and BioCem) were cured from a single surface using manufacturers’ recommended time intervals with a halogen light (3M ESPE, St. Paul, MN) (Table 1) [11, 12, 16, 17]. Immediately after curing, each disc was removed and placed into a test tube containing 10 mL of complete DMEM. The cement discs in their media were then incubated in a CO2 incubator at 37°C for 24 hours. After 24 hours, the cements’ extracts were then filter sterilized using 0.22 µm filters (Millipore, Billerica, MA) before treating the cells [16, 17].
Exposure of Cells to Cement Extracts
GN 23 or SG cells were counted using a TC 20 cell counter (BioRad, Hercules, CA) and plated into 96-well plates (BD, Franklin Lakes, NJ at a density of 3000 cells/well in a volume of 100µl/well complete DMEM. Cells in the plates were then cultured overnight. Then, the cell culture media was removed and replaced with 100 µl/well of filtered sterilized cements extracts, 0.1% TX-100, or complete DMEM, and incubated for 24, 48, or 72 hours.
MTT Assay
Effects of the cement extracts on cell viability were assessed by determining their effects on the ability of the cells to cleave the tetrazolium salt (3- [4, 5- dimethylthiazol-2-yl]-2,5-diphenyl tetrazolium bromide) (MTT) to a formazan dye, using a kit from Roche (Indianapolis, IN) [16, 17]. Briefly, cells were exposed to the extracts, untreated complete DMEM medium (negative control), or 0.1% Triton X-100 (TX-100; Sigma, St. Louis, MO), a detergent that is widely used to lyse cells, prepared in complete DMEM (positive control). After 24-, 48-, or 72-hours exposure, MTT assay was performed following the manufacturer’s instructions. MTT was added to the cells at a final concentration of 0.5 mg/ml and incubated for 4 hours at 37°C. Purple formazan crystals produced from the MTT by metabolically active cells were solubilized by 1 hour exposure to a solubilization solution provided in the kit, at 37°C.
Statistical Analysis
A two-way ANOVA was conducted, followed by Student-Newman-Keuls method using SigmaPlot 12.5 (Grafiti LLC, Palo Alto, CA). P0.05 was considered statistically significant.
For the GN 23 cells, after 24-hour exposure to the cement extracts, BioCem and Ketac, but not RelyX (P=0.338), caused statistically significant cytotoxicity, compared to the negative control (Figure 2). Ketac had a significantly greater effect on the cells than RelyX, and the effects of BioCem and Ketac were similar to one another (p=0.085). After 48 hours of exposure, all three cement extracts caused significant cytotoxicity (P≤0.001), with Ketac having the greatest effect. RelyX and BioCem had similar cytotoxic effects (p=0.07). A similar pattern was seen at the 72-hour time point.
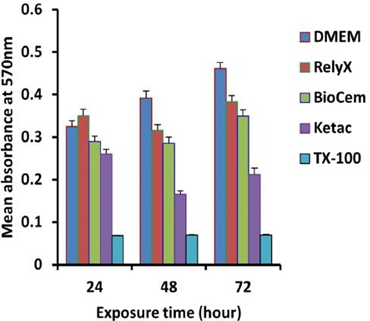
Figure 2: Cytotoxic effects of cements on human gingival fibroblasts (GN 23). Cells were plated at a 3000 cells/well density in 96 well plates. Each data point represents the mean ±SE, n>9. P0.05 was considered statistically significant.
For the SG cell line, after 24-hour treatment the three cements were similar to one another in that none caused significant cytotoxicity (P=0.107 and 0.851) (Figure 3 A). At 48 hours, however, all three cements caused significant cytotoxicity compared to the negative control (P≤0.001). At this time point, RelyX and BioCem had similar effects (P=0.566) and they were both less cytotoxic than Ketac (P≤0.001) (Figure 3 A). At 72 hours, all three cements caused statistically significant toxicity compared to the negative control (P≤0.05) (Figure 3 B). BioCem and RelyX both were significantly less toxic than Ketac (P≤0.001), and RelyX was significantly less cytotoxic than BioCem (P=0.034). SG cells were seeded at a 2000 cells/well density instead of 3000 cells/well density for the 72 hours treatment to avoid over confluent (Figure 3 B).
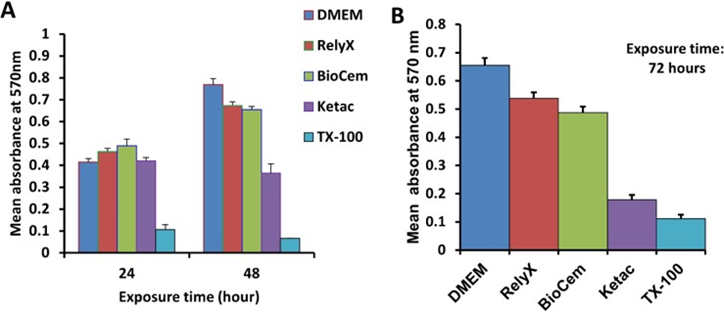
Figure 3: Cytotoxic effects of cement on human gingival epithelial cells (SG). A. SG cells after 24 or 48 hours of exposure cells were plated at a 3000cells/well density in 96 well plates. B. SG cells after 72 hours exposure; cells were plated at a 2000 cells/well density in 96 well plates. Each data point represents the mean ± SE, n>9. P0.05 was considered statistically significant.
When a primary tooth requires a full coverage crown, parents may request an esthetic option. In the past, the esthetic options included open-faced stainless-steel crowns, pre-veneered stainless-steel crowns, and strip crowns [1, 18, 19].
Prefabricated pediatric zirconia crowns were commercially introduced in 2008, and have become an increasingly popular option. Traditionally, SSC call for an intimate fit of the crown margins around the cervical portion of the tooth. When seating a SSC, the ideal fit is a fit such that the crown “snaps” on the tooth and the margins sit close against the tooth, ideally under a small undercut to help aid in retention of the crown [20, 21].
A seated SSC should be difficult to remove even without dental cement applied. When the dental cement is applied, the cement is held between the crown and the tooth. The dental cement is theoretically not in contact with the surrounding tissues. Zirconia crowns cannot be manipulated by the dentist and must fit passively over the prepared tooth with no stress-inducing contact between the crown and the tooh. This leads to a crown that has a sizable gap around the margin and will not stay in place without cementation. This gap is filled with dental cement and the surrounding tissues are exposed to the cured dental cement for the lifetime of the crown. Contact of these cements with gingival tissue could cause harmful effects to the surrounding periodontium. Much of the existing research on cytotoxicity of dental cements has been performed using mouse or bovine cell lines. The human cell lines used in this study may be better for predicting the cytotoxicity of a material in clinical situations since mouse and bovine cells may be more sensitive to insult, and could over-estimate the effect [22, 23].
Theoretically, if fibroblasts were negatively affected by exposure to dental cements, degradation of the periodontal ligament or other supportive structures could occur, perhaps resulting in tooth loss. Likewise, if gingival epithelial cells were affected in a similar way, this could lead to a loss in surrounding gingiva and result in both an esthetic concern and further loss of support. Therefore, it is beneficial for the dental provider to know the relative cytotoxicity of the dental products utilized. There are several cement options for a pediatric pre-formed zirconia crown. The three types of cement used in this study fall into three categories: self-adhesive resin cement (RelyX Unicem), bioactive cement (BioCem) and conventional glass ionomer cement (Ketac Maxicap.) Previous studies have shown that resin- based materials have toxic effects on human cells [24-27]. Studies have also shown that this cytotoxicity decreases over time until it is not detectable after 6 weeks [24, 27, 28].
In the current study, all extracts were made directly after curing of the cements occurred, which likely leads to results that give the highest level of toxicities that the cements would have on oral cells during their “lifetime” in the mouth. Further studies of cells exposed to cement extracts for longer periods should be conducted to determine their long-term toxic effects. While this study shows trends of differing cytotoxicity, it must be stated that, long term, these cements have the potential to have similar levels of cytotoxicity. The cytotoxic effects of the glass-ionomer cements were also found in previous studies [7, 24, 29-35]. Most studies show that leachable components of the dental material are responsible for the adverse effects to cells [7, 34]. The GIC used in the present study was the only “self-cured” cement studied. This “self-cured” cement consistently caused greater cytotoxicity than the other “light-cured” substances. This finding is similar to previous studies in which the light activation lessened cytotoxicity of certain cements [27, 36].
The theoretical implications of the cytotoxicity of cements could have important consequences on the supporting structure for primary teeth. However, pediatric dentists have been placing crowns with open margins (i.e. pre-veneered SSCs) with various cements with little clinically detectable long-term effect. This is likely due to the aforementioned finding that material cytotoxicity decreases with time. However, the higher cytotoxicity of GIC may be a possible contributing factor to some of the cases of inflammation that can be seen for several weeks post-cementation of crowns, especially when the crown is well-contoured and well-fitting [29]. This inflammation may resolve over time, allowing the gingival cells to proliferate and replace the cells that were injured or killed by the initial application of the cement. An additional clinically relevant finding is that the cytotoxicity of BioCem is less than that of GIC which has been used for many years in pediatric patients. Given that BioCem is a new material which has just recently come to market, practitioners can be confident in using this material in terms of cytotoxicity.
The findings from this in vitro study may not completely reflect the situation in vivo or long-term consequences in the clinic. For example, saliva in the oral cavity and the host immune response may affect the cells’ cytotoxicity responses. However, this in vitro cytotoxicity study is a relatively quick, inexpensive, and sensitive biocompatibility test compared to in vivo assays or clinical trials.
All dental cements tested had some cytotoxic effect on both the fibroblast and epithelial cell lines. Ketac Maxicap displayed the greatest cytotoxic effects when compared to BioCem and RelyX Unicem. BioCem was not significantly different from RelyX in its toxic effects on GN 23 cells at 48h and 72h, or on SG cells at 24 and 48h exposure. Further studies are needed to test if these differences in cytotoxicity continue over time, or if they occur in vivo.
This research was supported by the University of Tennessee Health Science Center College of Dentistry Alumni Endowment Fund and the Tennessee Dental Association Foundation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
