
Case Report | DOI: https://doi.org/10.31579/2690-4861/076
MS General Surgery, MBBS, B.Y.L Nair Charitable Hospital.
*Corresponding Author: Jayashri S. Pandya, MS General Surgery, MBBS, B.Y.L Nair Charitable Hospital.
Citation: R Ramteke, Swanit H. Deshpande, R Chiranjeev, Jayashri S. Pandya. (2020) Cystic Variation of Schwannoma in the Neck: A Rare Presentation. International Journal of Clinical Case Reports and Reviews. 4(3);DOI: 10.31579/2690-4861/076
Copyright: © 2020 Jayashri S. Pandya, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 October 2020 | Accepted: 09 November 2020 | Published: 13 November 2020
Keywords: schwannomas; neck swelling; radiological examination
It is uncommon for schwannomas to present as neck swellings. This case presented as painless, cystic and slow growing neck swelling which was excised. Histopathology proved it to be cystic schwannoma. Cystic change occurs in only 4% of all schwannomas. The cystic change renders the schwannoma to mimic second branchial cyst on clinical and radiological examination. Although modality of treatment remains the same which is extracapsular excision, the follow up differs in terms of recurrence.
Common differential diagnoses for benign neck masses are branchial cyst and necrotic cervical lymphadenopathy. Benign cystic lateral masses that can mimic branchial cleft cyst include thyroglossal cyst, carotid body tumours, ectopic thymic cyst, lymphangiomas, dermoid, cystic schwannoma epidermoid cysts and cystic nerve sheath tumours. [1]
Schwannomas are capsulated, slow growing, benign tumours arising from schwann cells of myelinated nerves, commonly called as neurilemmomas. They may arise from any peripheral, cranial or autonomic nerve. More than 25 % Schwannomas are found in head and neck region. [2] Schwannoma of neck is a relatively uncommon tumor. [3] Origin of the schwannoma in the neck is more commonly from vagus and very rarely from cervical sympathetic chain. Cervical vagal Schwannoma constitute 2-5% of neurogenic tumours.
There are two types of tissues in schwannoma viz Antoni A and Antoni B. The layering with fluid levels is caused by hemorrhages. Usually Antoni B undergoes cystic change and hemorrhagic degeneration. The cystic variants comprise of 4% tumours. [1, 4, 5] The cystic Schwannoma grows more rapidly than non-cystic type.
Most common cystic mass in the neck is branchial cleft cyst. Branchial cleft cyst most common congenital cyst arising anterior to sternocleidomastoid.
This case is a rare presentation of cystic schwannoma demonstrating the classic location and CT signs of a branchial cyst in a 36-year female patient with left sided neck mass. Tumour was excised and histopathology revealed the tumour to be cystic schwannoma.
Case Presentation
Thirty six years old female presented with solitary painless cystic swelling over left side of the neck, which was insidious in onset and gradually increasing in size over the past five years. The swelling caused no change in voice, neurological deficit like numbness, pain, dysphagia, weakness or facial nerve palsy.
Patient has history of pulmonary tuberculosis in her childhood for which she took complete treatment. Patient had no other co-morbidities.
On local examination, there was a left sided 4*3cm single cystic fusiform swelling arising from lower 1/3rd of anterior triangle of neck at the level of cricoid, crossing middle 3rd of sternocleidomastoid muscle and reaching postero-superior boundary of posterior triangle of neck. It was 1cm below left mastoid tip.

Oral examination showed normal tonsillar fossa. There was no evidence of internal opening or sinus tract. No obvious bulge or displacement of peritonsillar structures was seen. Uvula was central in position. Gag reflex was present.
70 degree scopy revealed bilateral vocal cords free and mobile. Para-pharyngeal space examination was normal.
Investigations
Ultrasound neck report revealed a well circumscribed hypoechoic soft tissue lesion with internal vascularity along antero-lateral aspect of internal and external carotid arteries and closely abutting internal carotid artery. USG Doppler of neck revealed fairly well defined, oval, anechoic cystic lesion with smooth walls measuring 55*47*30 mm. The lesion had multiple internal septations. The lesion was located in the left carotid space anterior to left sternocleidomastoid. It was suspected to be compressing superior 1/3rd of internal jugular vein (IJV) posteriorly. Distal and mid 1/3rd of IJV showed normal course, caliber and colour flow.
CT scan showed a well differentiated multi-septate predominantly cystic lesion with a few enhancing solid components at periphery of approx. 65*42*30 mm in left carotid space. No evidence of any lymphadenopathy. The lesion was located in the left carotid space anterior to left sternocleidomastoid.
Fine needle aspiration cytology (FNAC) of the lesion showed benign cystic lesion and was inconclusive.
Differential Diagnosis
On clinical history, examination and investigations, the primary diagnosis was branchial cyst from 2nd cleft with differential of cystic Schwannoma.
Treatment
Decision was taken to surgically remove the tumour. Extracapsular enucleation of tumour was done. Curvilinear skin incision was taken. A cystic swelling 3.3*2.1*0.9cm in subplatysmal plane was visualized. The tumour had irregular surface with extension behind sternocleidomastoid. It was abutting the adjacent soft tissues and blood vessels. The cystic tumour was separated and extracapsular enucleation was performed. Swelling was related anteriorly to sternocleidomastoid, medially to internal jugular vein and vagus nerve, supero-posteriorly to marginal mandibular nerve. It was found arising from vagus nerve.
Marginal mandibular nerve was flush to swelling in its superior-posterior aspect.
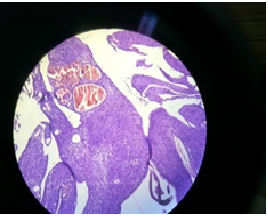
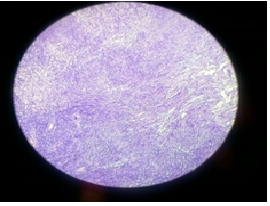
On microscopic examination the tumour was well circumscribed. It showed large cystic areas and cystic spaces, lined by spindle tumour cells which were arranged in bundle in streaming fashion. Individual cells had moderate eosinophilic cytoplasm with elongated wavy nuclei which at places showed Varocay body formation. Some of these foci showed increased intervening matrix, representing Antony B areas. Some areas showed crowding of cells representing Antony A areas. There were well distributed dilated and congested spaces. Vascular channels were seen. No mitoses or areas of necrosis were identified. [Fig 2, 3] These findings confirmed the diagnosis of schwannoma with cystic change.
Outcome and Follow-Up
The histopathology confirmed diagnosis of Cystic Schwannoma arising from Vagus nerve.
Patient had minimum post-operative deviation of angle of mouth, mild ptosis of left eyelid, marginal mandibular nerve paresis and features suggestive of First bite syndrome. Patient recovered completely with physiotherapy in two weeks after surgery.
There was no vocal cord paralysis. Patient was asymptomatic after 2 months follow up.
Discussion
The clinical and radiological examination by virtue of the location of the tumour makes branchial cyst as the first differential diagnosis. Schwannomas rarely recur. In cases of branchial cyst, a long term follow-up is necessary as it tends to recur.
Varocay first reported Schwannoma in 1910. Schwannnomas are nerve sheath tumours which arise from cells of neural sheath. They may arise from any central, peripheral or autonomic nerve. Schawannoma can arise from all cranial nerves, most common being 8th cranial nerve.[2] However in approximately 10-40% cases origin of nerve remains unidentified. The most common location of schwannomas of head and neck is parapharyngeal space. Schwannoma of neck is a relatively uncommon tumour. Cervical vagal schwannoma constitutes 2-5% of neurogenic tumours. Other locations include submandibular space, paranasal sinuses, cheek and oral cavity which are rare.
When arising from parapharyngeal space, they present as asymptomatic, slow growing neck masses. Pre- operative diagnosis is difficult as most patients do not have neurological deficit. Hence, other common neck swellings may be considered as differential diagnoses ahead of schwannomas. More common neck swellings are branchial cyst, paraganglioma, lymphoma and metastatic cervical lymphadenopathy.
Schwannomas often present as solitary, painless, slow growing mass of variable size. Cystic Schwannoma grows more rapidly than non-cystic Schwannoma. Hoarseness is the most common presenting symptom. Elicitation of paroxysmal cough on palpation of mass is a specific but rare clinical sign seen in vagal Schwannomas.
The diagnostic difficulty may be further compounded by marked cystic changes which is present in only 4% of cases. The cystic change is attributed to necrosis, mucinous degeneration, and hemorrhage and microcyst formation.
The first documented case of a cystic Schwannoma of neck masquerading as branchial cyst clinically and on ultrasonography was reported by Buchanan et al. [4]
In our patient on clinical examination, it was difficult to differentiate between branchial cyst and cystic schwannoma as both can present with painless slow growing mass without any symptoms in lateral neck. [2, 5]
On Ultrasound examination, Branchial Cyst shows variable echogenicity but no internal vascularity. Schwannomas on colour doppler show internal vascularity. [6] In our patient the ultrasound did document internal vascularity.
Fine Needle Aspiration Cytology (FNAC) was inconclusive. Usually in Schwannoma due to hemorrhagic aspirate or inadequate cellular material
Decision for surgical excision was taken and extracapsular enucleation was done. It was found intraoperatively arising from vagus.
Learning Points/Take Home Messages
• Although Branchial Cyst is more common but while dealing with cystic swelling of neck, the possibility of schwannoma should also be considered.
• Cystic schwannoma can present as branchial cyst radiologically and clinically but meticulous surgical dissection, tracing the site of origin of the mass and final histopathology report are guides towards correct diagnosis.
• It is important to look for signs and symptoms of neurological deficit in the post-operative period.
• Complete surgical excision is treatment of choice in symptomatic cystic schwannomas.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
