
Case Report | DOI: https://doi.org/10.31579/2690-1919/295
1 Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
2 Radiology Department, Federal Medical Center Bida, Niger State.
*Corresponding Author: Sule Muhammad Baba. Radiology Department, Usmanu Danfodiyo University Teaching Hospital, Sokoto.
Citation: Shamaki AMB, Gusau AA, Sule MB, Erinle SA, Dada MA. (2023). Cystic Brain Lesion in A Child Most Likely Hydatid Cyst: The Computed Tomographic Findings and A Case Report. J Clinical Research and Reports, 13(2); DOI:10.31579/2690-1919/295
Copyright: © 2023 Sule Muhammad Baba. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 January 2023 | Accepted: 24 January 2023 | Published: 01 February 2023
Keywords: hydatid cyst; child; brain; computed tomography
Hydatid disease of the brain is a very rare disease entity, and accounts for about 1-2% of all Echinococcus granulosis infections.
This is a fifteen-year-old male child that presented from a peripheral health facility for an enhanced computed tomography of the brain on account of a six-month history of recurrent headaches, feeling of heaviness in the head and repeated convulsions.
The enhanced computed tomography demonstrated a non-enhancing multiple cystic area with a central solid area with no surrounding edema but causing erosion, areas of irregularities and discontinuity of the adjacent skull vault.
The CECT findings with the patient’s clinical history rose a suspicion of hydatid cyst of the brain, currently the patient is placed on medical treatment and been prepared for surgical excision of the cystic lesion.
Hydatid disease is a rare disease and endemic in Middle East, Southern Europe, Australia, New Zealand and South America [1]. The disease is caused by infestation of the larvae of Taenia echinococcus, with brain involvement been rare and about 1-2% [1-3].
Cerebral hydatid disease is very rare, and could either be primary or secondary, the primary is entirely caused by direct infestation of the brain without concomitant involvement of other organs. The primary disease is most probably from patient’s immune incompetence, patent ductus arteriosus, patent foramen ovale and special brain architecture [3,4].
Hydatid disease basically involves mainly the liver and lungs, with involvement of the brain very rare and in about 1-2% of cases. The cerebral disease is most commonly seen in childhood and often solitary causing varying neurologic manifestations, some of which are seizures and paralysis [1-6].
Hydatid disease of the brain may be located in any part of the brain, but most often times seen in both hemispheres along the middle cerebral artery territory with the parietal lobe of the brain the most frequently involved site of affectation [1,6 ,7].
Imaging plays a vital role in diagnosing hydatid cyst of the brain; the imaging modalities are mainly computed tomography and magnetic imaging resonance of the brain [1-8]. Histopathological examination is however the gold standard in its diagnosis [2,8].
The treatment for intracranial hydatid cyst is mainly by surgical removal of the cyst following the Dowling’s technique with pre and post administration of Albendazole prophylactically and to reduce the rate of occurrence of the cyst [1-9].
This is a fifteen-year-old male child that presented from a peripheral health facility for an enhanced computed tomography of the brain on account of a six-month history of recurrent headaches, feeling of heaviness in the head, multiple swellings in the fronto-parietal skull vault and repeated convulsions.
The patient was conscious and oriented, not dehydrated, not pale, anicteric and acyanosed. The neurological assessment was normal. The cardiovascular assessment also was normal for the patient’s age. Serological examination to rule out the possibility of infestation of the abdominal organs with hydatid disease was negative.
The enhanced computed tomography demonstrated a huge non-enhancing multiple cystic area with a central solid area with no surrounding edema but causing erosion, areas of irregularities and discontinuity of the adjacent skull vault. These findings are demonstrated on figures 1-5.
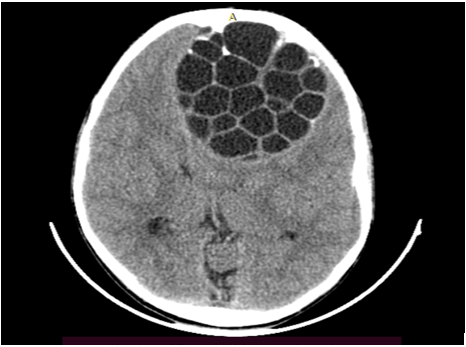
Figure 1: Non-enhanced computed tomographic image of the brain at the level of the lateral ventricles anteriorly demonstrating multiple well demarcated and non-communicating cysts having a honey-comb pattern.

Figure 2: An axial contrast enhanced computed tomography of the brain demonstrating a huge mass with a central non-enhancing nodule and multiple non-communicating thin-walled cysts having a spoke-wheel appearance. Erosion and defects of the adjacent skull vault is also demonstrated.
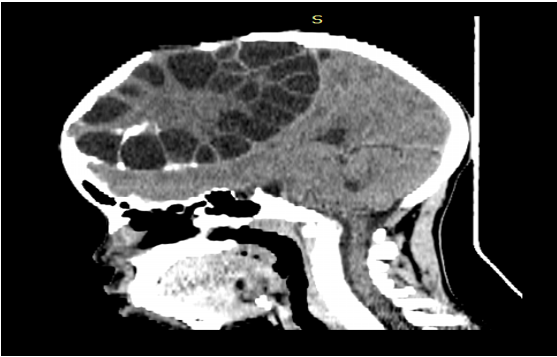
Figure 3: A sagittal contrast enhanced computed tomography of the brain demonstrating a huge mass with a central non-enhancing nodule and multiple non-communicating thin-walled cysts having a spoke-wheel appearance. Erosion and defects of the adjacent skull vault with compressive effect on the posterior horn of the lateral ventricle are also demonstrated.

Figure 4: A reconstructed coronal non-enhanced computed tomographic image of the brain at the level of the lateral ventricles anteriorly demonstrating multiple well demarcated and non-communicating cysts having a honey-comb pattern. No surrounding edema is demonstrated.
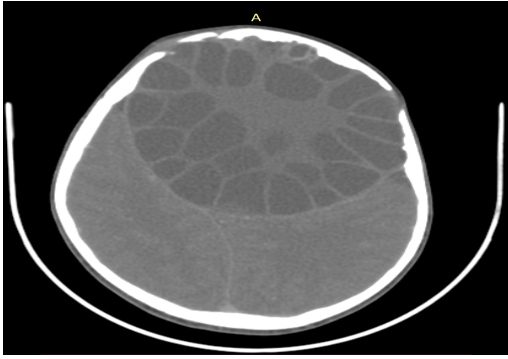
Figure 5: An axial tomographic image of the brain on bone window demonstrating areas of cortical discontinuity in keeping with skull defects and areas of undulation, erosions and irregularities due to pressure effect of the cystic mass.
The CECT findings with the patient’s clinical history rose a suspicion of hydatid cyst of the brain, currently the patient is placed on medical treatment and been prepared for surgical excision of the cystic lesion.
The medical treatment given to the patient is oral albendazole 15mg per body weight twice daily and open currently without duration, this will continue after the surgical excision to prevent recurrence and systemic involvement.
Hydatid disease is a rare disease and endemic in Middle East, Southern Europe, Australia, New Zealand and South America1. The disease is caused by infestation of the larvae of Taenia echinococcus, with brain involvement been rare and about 1-2% [1-3]. The case under review does not live in an endemic area and has involvement of the brain primarily most likely following infestation of the larvae of Taenia echinococcus.
Hydatid disease basically involves mainly the liver and lungs, with involvement of the brain very rare and in about 1-2% of cases. The cerebral disease is most commonly seen in childhood and often solitary causing varying neurologic manifestations, some of which are seizures and paralysis [1-6]. The index case is a child and had a cerebral disease which came out to be solitary on imaging. The patient also presented with history of seizures and weakness involving the upper limbs, thereby conforming to these literatures.
Hydatid disease of the brain may be located in any part of the brain, but most often times seen in both hemispheres along the middle cerebral artery territory with the parietal lobe of the brain the most frequently involved site of affectation [1,6,7]. The index case had involvement of both hemispheres and in the parietal region anteriorly, thereby conforming to these literatures.
Imaging plays a vital role in diagnosing hydatid cyst of the brain; the imaging modalities are mainly computed tomography and magnetic imaging resonance of the brain [1-8]. The case under review was diagnosed mainly following computed tomographic examination of the brain, thereby conforming to these literatures.
The main findings from imaging are that of a solitary mass with multiple non-communicating cysts with non-enhancing solid nodule most often in the parietal lobe with no surrounding edema [1,3,5,7]. The case under review was not an exception, a solitary huge mass with multiple non-communicating cysts and non-enhancing solid nodule with no surrounding edema in the parietal lobes was demonstrated thereby conforming to these literatures.
The treatment for intracranial hydatid cyst is mainly by surgical removal of the cyst following the Dowling’s technique with pre and post administration of Albendazole prophylactically to reduce the rate of occurrence of the cyst [1-9]. Similar treatment options were suggested for the index case, currently taking oral albendazole and been prepared for surgical removal of the cystic mass, thereby conforming to these literatures.
Patients with suspicion of cystic lesions of the brain should have be imaged either by computed tomography or magnetic resonance imaging to rule out hydatid disease, this will also give room for early institution of management to prevent associated morbidity and mortality associated with the disease.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
