
Research Article | DOI: https://doi.org/10.31579/2641-0419/047
*Corresponding Author: Mohamed Wasfy Mohamed, Cardiology department, Shebin El-kom teaching hospital, Menoufia, Egypt.
Citation: Mohamed W. Mohamed., Said S. Montaser., Waleed A. Ibrahim. (2020) Cystatin C in patients with coronary artery disease. J. Clinical Cardiology and Cardiovascular Interventions, 3(5); Doi:10.31579/2641-0419/047
Copyright: © 2020 Mohamed Wasfy Mohamed, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 January 2020 | Accepted: 29 February 2020 | Published: 12 March 2020
Keywords: coronary artery disease; cystatin c.
Background:
Cystatin C, a marker for early stage chronic kidney dysfunction, mediates the pathogenesis of cardiovascular diseases.
Objectives:
To assess the relation between level of serum Cystatin C and severity of coronary artery disease (CAD) in patients without chronic kidney disease (CKD).
Patients and Methods:
In this cross-sectional study, we included 80 patients with CAD divided in two groups (group I with acute coronary artery disease and group II with chronic stable coronary artery disease) 40 patients each and acquired their demographic characteristics, medical histories, and listings of the concurrent medications they were taking. All patients with CAD underwent ECG, echocardiography, coronary angiography, serum Cystatin C level, cardiac enzymes and other routine laboratory tests.
Results:
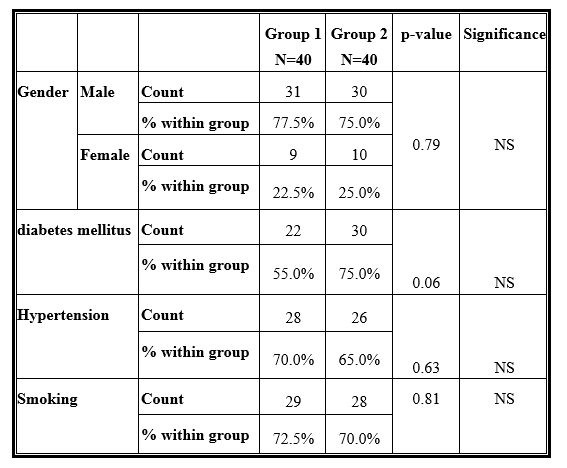
As regard demographic data and comorbidities there was no significant difference between the two groups as regard gender, diabetes mellitus, hypertension or smoking.
Also, As regard level of serum Cystatin C, the mean and SD in 1 vessel affection was 0.92±0.07 while in 2 vessels affection was 1.07±0.13 and 3 vessels affection was 1.41±0.05 with (P< 0.01).
Finally, there was a highly significant difference as regard Cystatin C level with mean and SD 1.21±0.18 in ST-segment elevation MI while mean and SD was 0.96±0.09 in Non ST-segment MI or unstable angina with (P< 0.01). There was a statistically significant correlation between level of Cystatin C and severity of CAD (p < 0.05).
Conclusion:
Serum cystatin C has a significant effect on the severity of coronary artery disease (CAD), being higher in patients with 3 vessels disease and severe CAD.
Atherosclerotic cardiovascular disease is the leading cause of death in both men and women, with an estimated 17.5 million deaths globally in 2012. Further, according to World Health Organization (WHO) estimates, cardiovascular disease as cause of death will increase in both high and low income countries over the next 15 years (1). Within the coming decades it is estimated that the loss of disability-adjusted life years (DALYs) are expected to rise, from 85 million DALYs in 1990 to 150 million DALYs globally in 2020, making it the leading somatic cause of loss of productivity (2).
The main underlying cause of cardiovascular disease, atherosclerosis, and its complications are thus of major importance to public health worldwide.
Risk factors for the development of cardiovascular disease have been thoroughly studied (3) and big efforts and progress have been made in identifying subjects at increased risk. Traditional risk factors such as age, gender, smoking, hypertension, blood lipids and heredity are combined when estimating an individuals’ risk of future cardiovascular disease. However, medical endeavors in recent decades have substantially increased survival in patients with cardiovascular disease, creating a growing elderly population with a high prevalence of established cardiovascular disease and cardiovascular risk factors. Traditional risk factors lose some of their predictive ability with increasing age (4) and their predictive ability in established disease is not as well studied in healthy cohorts. In order to identify new markers to improve risk assessment in elderly persons and in persons with known cardiovascular disease it is of importance to identify new predictive markers.
Cystatin C, first and foremost known as a marker of renal function and considered a better marker of glomerular filtration rate (GFR) than serum creatinine, has been suggested as a possible independent biomarker of cardiovascular disease (CVD) (5). Chronic kidney disease (CKD) and cardiovascular disease share common risk factors and often coexist and therefore the relation between cystatin C and CVD is intricate and causal mechanisms are difficult to study. To study the relative importance of how genetic and environmental factors influence variations in cystatin C, how they influence the development of atherosclerosis, and how they influence the association between cystatin C and CVD, may provide new important new knowledge on this relation.
2.1. Study Design
This is a cross-sectional study, which included 80 adult patients > 18 years of age with CAD divided in two groups (group I with acute coronary artery disease and group II with chronic stable coronary artery disease) 40 patients each to investigate the relation between Cystatin C and severity of CAD.
2.2. Study Population
All patients >18 years of age admitted with CAD (Acute and chronic forms) and not having any of the exclusion criteria were included in the study.
All patients were subjected to informed consent, thorough history taking and clinical examination, with special concern on history of smoking, history of chronic diseases like diabetes and hypertension history of previous coronary angiography or previous PCI, and history of previous myocardial infarction. They were also subjected to ECG, echocardiography, coronary angiography, serum Cystatin C level, cardiac enzymes and other routine laboratory tests.
2.3. Statistical Analysis
Data were collected, revised and edited into a master table using Microsoft Excel 2013. Data were then revised, coded and entered to the statistical package for social science (SPSS) version 22. For quantitative variable, mean and standard deviation were calculated. For categorical variable, number and percentage were calculated. Analytical statistics were performed using independent sample t test to compere between the mean of the quantitative variables and chi square (x2) test used to compare between categorical variables. Differences were considered statistically significant at P value ≤ 0.05.
The study population consisted of 80 patients divided into 2 groups (group I with acute coronary artery disease and group II with chronic stable coronary artery disease), 40 patients each with established CAD whether acute or chronic. In the acute group, 31 (77.5%) of the patients were males and 9 (22.5%) were females while in the chronic group, 30 (75%) of the patients were males and 10 (25%) were females.
Also, in the acute group, 22 (55%) of the patients were diabetics while in the chronic group, 30 (75%) of the patients were diabetics.
As regard hypertension, in the acute group, 28 (70%) of the patients were hypertensive while in the chronic group, 26 (65%) of the patients were hypertensive.
Also as regard smoking, in the acute group, 29 (72.5%) of the patients were smokers while in the chronic group, 28 (70%) of the patients were smokers.
With these findings, there was no significant difference between the two groups as regard gender, diabetes mellitus, hypertension or smoking. (Table 1)
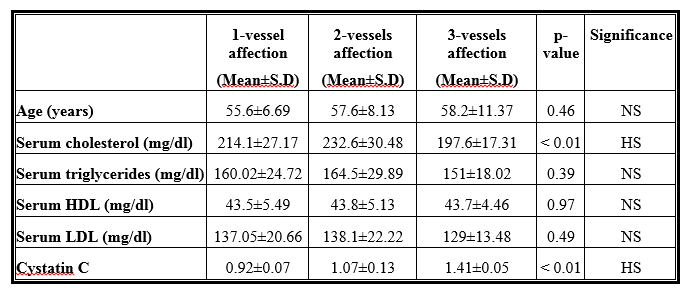
In all patients and according to the number of vessels affected, the mean and SD of the age in 1 vessel affection was 55.6±6.69 while in 2 vessels affection was 57.6±8.13 and in 3 vessels affection was 58.2±11.37 with (P=0.46).
Also, the mean and SD of the level of serum cholesterol in 1 vessel affection was 214.1±27.17 while in 2 vessels affection was 232.6±30.48 and in 3 vessels affection was 197.6±17.31 with (P< 0.01).
As regard serum triglycerides, the mean and SD in 1 vessel affection was 160.02±24.72 while in 2 vessels affection was 164.5±29.89 and in 3 vessels affection was 151±18.02 with (P=0.39).
Also, the mean and SD of the level of serum HDL in 1 vessel affection was 43.5±5.49 while in 2 vessels affection was 43.8±5.13 and in 3 vessels affection was 43.7±4.46 with (P=0.97).
In addition, the mean and SD of the level of serum LDL in 1 vessel affection was 137.05±20.66 while in 2 vessels affection was 138.1±22.22 and in 3 vessels affection was 129±13.48 with (P=0.49).
As regard level of serum Cystatin C, the mean and SD in 1 vessel affection was 0.92±0.07 while in 2 vessels affection was 1.07±0.13 and 3 vessels affection was 1.41±0.05 with (P< 0.01).
(Table 2) (Figure 1)
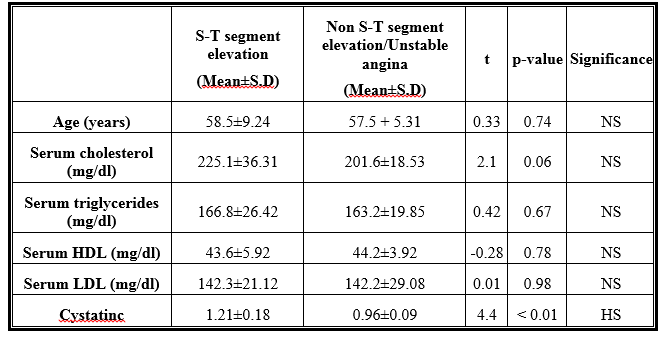
According to the severity of coronary artery disease In group 1 patients by comparison as regard age, serum cholesterol, serum triglycerides, serum HDL, serum LDL and serum Cystatin C, there was no significant difference as regard age, serum cholesterol , serum triglycerides ,serum HDL and LDL , however there was a highly significant difference as regard Cystatin C level with mean and SD 1.21±0.18 in ST-segment elevation MI while mean and SD was 0.96±0.09 in Non ST-segment MI or unstable angina with (P< 0.01). (Table 3)
Coronary artery disease (CAD) is the leading cause of morbidity and mortality worldwide. Asymptomatic patients have a higher cardiac mortality risk than those with symptomatic CAD (6).
An early identification and treatment of asymptomatic CAD patients may significantly improve their cardiovascular prognosis. Unfortunately, the early diagnosis of asymptomatic CAD is always missed or delayed because the typical symptoms of cardiac ischemia are often masked. To date, classic assessment such as Framingham Risk Score (FRS) could not identify asymptomatic CAD effectively. Biochemical markers might play crucial roles on initial assessment of asymptomatic CAD (7).
Recent studies have revealed that cystatin C is not simply regarded as a candidate marker of impaired kidney function. In Prospective Epidemiological Study of Myocardial Infarction (PRIME), cystatin C predicted the occurrence of the first coronary events in men aged 50 to 59 years old, and displayed a strong relation with CAD independent of eGFR (8).
In our study we found no significant difference between the two groups as regard gender .This results are in agreement with Zhao R, 2016(9) who found no effect of gender on prevalence of coronary artery disease .
Also, we found no significant difference between the two groups as regard prevalence of diabetes .This results are in agreement with Qing X et al., 2015(10) who found no effect of diabetes on prevalence of the type of coronary artery disease .
In addition, we found no significant difference between the two groups as regard prevalence of hypertension .This results are in agreement with Erne P et al., 2015(11) who found no effect of hypertension on prevalence of the type of coronary artery disease .
Interestingly we found a significant difference between the two groups as regard number of vessels affected .This results are in agreement with Mirzaie M et al., 2014(12) who found a significant effect of the severity of coronary coronary artery disease on number of vessels affected.
In our study we found no significant difference between the two groups as regard age .This results are in agreement with Erne P et al., 2013(11) who found no effect of age on prevalence of the type of coronary artery disease .
A significant difference between the two groups as regard LDL level was found.This results are in agreement with Mahalle N et al., 2014(13) who found a significant effect of dyslipidaemia as a component of metabolic syndrome on the severity of coronary artery disease.
In agreement with Lodh M et al., 2013(14) who found a significant effect of serum Cystatin C on the severity of coronary coronary artery disease, we found a significant difference between the two groups as regard serum Cystatin C level.
In our study we found a significant effect of Cystatin C level on number of vessels affected. This results are in agreement with Abid L et al., 2016(15) who found a significant effect of serum Cystatin C on the severity of coronary coronary artery disease.
In addition, we found a significant effect of serum cholesterol level on number of vessels affected .These results are in agreement with Khashayar P, 2010(16) who found a significant effect of serum Cystatin C on the severity of coronary coronary artery disease .
Type of MI is dependent on severity of acute coronary syndrome. As a prognostic factor, Cystatin c may be also related to type of MI. In our study we found a direct relation between patients with S-T elevation MI and Cystatin C level which is more elevated in these patients .This results are in agreement with Chen HH, 2010(17) who found a direct significant relation between Cystatin C and STEMI.
Although the number of patients enrolled in our study is relatively small, the results are quite comparable to larger studies. This study was observational and single-institutional in nature, which possibly restricted us from identifying and analyzing all potential confounding factors.
From our study and supporting trials, we found that serum cystatin C has a significant effect on the severity of coronary artery disease (CAD), being higher in patients with three-vessels disease and severe CAD and we found a direct significant relation between Cystatin C and STEMI, so we recommend using serum Cystatin C as a predictor for coronary artery disease especially the acute forms.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
