
Research Article | DOI: https://doi.org/10.31579/2641-0419/482
1National Cardiology Center Nouakchott, Mauritania.
2G. Monasterio Foundation, Tuscany Region, Pisa.
3Cardiovascular Department San Camillo Hospital, Rome.
4Clinical Physiology Institute, CNR, Pisa.
5National Institute of Diabetes and Digestive and Kidney Disease, National Institutes of Health.
*Corresponding Author: Ethmane Sidi Mhamed, National Cardiology Center Nouakchott, Mauritania.
Citation: Ethmane S. Mhamed, Jabeur Nidhal, Marco S. Nazzaro, Francesca Mastorci, Elhadj A. Ne, (2025), CV Risk Factors, Percutaneous Coronary Revascularization and prognosis in CAD Patients in Mauritania, J Clinical Cardiology and Cardiovascular Interventions, 8(11); DOI: 10.31579/2641-0419/482
Copyright: © 2025, Ethmane Sidi Mhamed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 May 2025 | Accepted: 18 June 2025 | Published: 23 July 2025
Keywords: pulmonary artery catheter balloon; embolization; transesophageal echocardiography; cardiac surgery
Objective: To characterize gender cardiovascular (CV) risk profile in Mauritanian rural and urban cohorts of patients with documented coronary artery disease (CAD) undergoing percutaneous coronary revascularization (PCI). Further, we assessed prognostic impact of clinical and CV risk factors.
Methods: We studied prospectively 180 patients (mean age 58±0.6, 150 males) undergoing coronary ngiography and PCI for the following clinical conditions: recent or previous coronary syndrome (n=134), documented ischemia on effort (n=40), acute myocardial infarction (AMI, n=6). At follow-up cardiac and overall death and non-fatal AMI were considered. Clinical variables, including medications and CV risk factors, were collected.
Results: Smoking was more frequent in males in respect to females (p<0.05), whereas obesity was significantly higher in females than in males (p<0.05). The incidence of left ventricular ejection fraction (<40%) was significantly higher in females (p<0.05). There were 127 significant stenosis of left descending artery, 38 of circumflex artery, and 60 of right coronary. The total number of PCI was 243. During follow-up, 22 events occurred: 14 deaths (11 cardiac deaths), 8 non-fatal AMI. At univariate analysis, the only independent variable of the events was the rural/urban location (p<0.05).
Conclusions: In patients with documented CAD undergoing PCI, smoking and obesity are the only CV risk factors with a different gender incidence. The only independent variable of major adverse cardiac events was rural location. As the availability of antiaggregant therapy is critical in rural areas, educational, and prevention plans as well as wide network of operational resources are extremely needed.
Key Messages
What is already known about this subject?
CV risk profile is well known in African population, but it is not diffusely known in Mauritanian population. Furthermore, in our study we delineated CV profile in patients with documented CAD, whereas CV risk profile is generally descripted in the general population
What does this study add?
This is the first study reporting the first experience of percutaneous coronary revascularization in Mauritania. The clinical importance of this report rises up from the evidence that Mauritania is in full epidemiological transition with a continuous increase in CAD incidence
How might this impact on clinical practice?
The clinical impact of this study is linked also to the evidence that rural location has higher probability of cardiac events at follow up. This is an indirect proof that education to antiaggregant therapy and the availability of it are an important practical impact to reduce cardiac events in CAD patients treated con PCI
Mauritania is a developing country included within the Arab word as a low-income country. In these countries, the epidemiologic transition, that is the shift from a predominance of nutritional deficiencies and infectious diseases to the chronic degenerative diseases, is occurring as consequences of urbanization, increased life expectancy and changes in style life [1,2]. With regard to the cardiovascular (CV) field, epidemiological transition means the increase in traditional cardiovascular risk factors, and consequently the augmented incidence of coronary artery disease (CAD) and major cardiac events [3-5]. In the Africa Middle East CV Epidemiological (ACE) study, 92% of adult subjects attending for general practice had at least one modifiable CV risk factor and 53% 3 or more, with the prevalence of smoking in males and obesity in women [4].
Interestingly, the presence of CV risk factors was also present in younger outpatients suggesting the need of screening for early identification and management of CV risk factors [4]. Also, the risk for Acute Myocardial Infarction (AMI) increased with higher income and education in the black African group in contrast to findings in the other African groups [6]. Further, according to the Interheart African study, the modeling of 5 risk factors including smoking, diabetes, hypertension, abdominal obesity, and apolipoprotein B/A-1 ratio, provided a population attributable risk of 89.2% for AMI [6]. The increased CV risk coincided with the evidence that ischemic heart disease was the top cause of death in the Arab world in 2010, contributing to 14·3% of deaths, thus replacing lower respiratory infections, that, however, continues to be the first cause of death in the low income countries [5].
The increase in CV risk factors was confirmed in the WHO report of Mauritania [7]. Therefore, at the light of epidemiological transition, that is becoming to involve Mauritania, the need to acquire expertise in the field of coronary revascularization is mandatory as therapeutic option for treating patients with AMI and symptomatic CAD. In this study, we report the first experience of coronary angiography and percutaneous coronary revascularization (PCI) performed in Mauritania in the period between November 2011 and April 2014, in patients with acute and recent myocardial infarction and with myocardial ischemia on effort. Therefore, the aim of the study was to characterize gender cardiovascular risk profile in a rural and urban cohorts of patients with documented CAD undergoing PCI. Further, we assessed prognostic impact of clinical and CV risk factors.
Patients
We studied prospectively 180 patients (mean age 58±0.6, Male = 150) who were referred to Cheik Zayed Hospital, a section of the Centre Nationale de Cardiologie (CNC) in Nouakchott, to undergo coronary angiography and percutaneous coronary revascularization for the following clinical conditions: recent or previous coronary syndrome, within 6 months the occurrence of the acute event (n = 134), documented ischemia on effort (n = 40), acute myocardial infarction (n = 6). Inclusion criteria included life expectation > 1 year, availability to assume antiplatelet therapy. The clinical variables, including medications taken and CV risk factors, were collected.
Echocardiography was performed in all patients to assess left ventricular ejection fraction according to the Sympson formula. Patients were enrolled between November 2011 and April 2014 when hemodynamic Italian interventional cardiology team went to the Cheik Zayed Hospital, which is the only cardiologic hospital equipped with a catheterization laboratory present in the country (four missions) according to the Italian Government program project AID 9580/ICU/MRT. The study was approved by the local Ethics Committee: the investigation conformed to the principles outlined in the Declaration of Helsinki. All patients gave their informed consent before the study
Coronary angiography and percutaneous orconary angioplasty
The radiographic equipment used was Philips Integris Allura 9, Germany. Cine angiograms were acquired with hand injections, and obtained according to standard guidelines [8]. Standard morphologic criteria were used to characterize the complexity of the lesions at baseline and to identify angiographic complications. They were analyzed by two expert interventional cardiologists and in borderline cases a quantitative coronary angiography analysis was used. PCI has been performed according to the standard practice, including stent implantation and medical therapy (aspirin 100 mg indefinitely, and clopidogrel 75 mg/d for at least 12 months) [8].
Follow up
The events considered at follow up were cardiac and overall death, and nonfatal myocardial infarction. The definition of cardiac death required the documentation of significant arrhythmia or cardiac arrest or death attributable to congestive heart failure or myocardial infarction in the absence of any other precipitating factor. In case of out-of-hospital death not followed by autopsy, sudden unexpected death was classified as cardiac death. Myocardial infarction was defined as a cardiac event requiring hospital admission to the hospital, with development of new electrocardiograph changes and cardiac enzyme-level increases.
The Kolmogorov-Smirnov test was used to assess normality of data. Statistical tests used to compare groups included the Student t test and ANOVA for difference in mean values, the Mann Whitney U and the Kruskal-Wallis H tests for skewed variables, and the X2 test for difference in counts and frequency.
The effect of each potenti3al predictor on cardiac-related and non-cardiac related deaths was assessed by binary logistic regression analysis. A p-value less than 0.05 was considered significant. Data are presented as mean±SD or as median with interquartile range. Analyses were performed using SPSS 21 software (IBM Corp., Armonk, NY).
Clinical and anthropometric characteristics of the study population are reported in Table 1. The large part of patients had 2 or 3 CV risk factors and there was no difference in the number of thembetween male and female (Figure. 1).
| Variable | Total cohort (n=180 | Male (n=150) | Female (n=30) | P value Male vs female |
| Characteristics of patients | ||||
| Age | 57.89±0.61 | 57.21±0.93 | 61.30±2.02 | n.s. |
| Weight (Kg) | 42.40±5.44 | 76.65±0.67 | 80.53±1.68 | p<0> |
| Height (m) | 1.69±0.00 | 1.70±0.00 | 1.68±0.01 | n.s |
| BMI (Kg/m2) | 26.68±0.21 | 26.32±0.23 | 28.48±0.47 | p<0> |
| Current FE | 50.97±0.51 | 51.58±0.52 | 47.93±1.53 | p<0> |
| Race | ||||
| White | 142 (79%) | 120 (80%) | 22 (73%) | ns |
| Black | ||||
| Number of risk factors | 37 (21%) | 30 (20%) | 7 (23%) | ns |
| 0 | 9 (5%) | 8 (5%) | 1 (3%) | ns |
| 1 | 89 (49%) | 76 (51%) | 13 (43%) | ns |
| 2 | 63 (35%) | 51 (34%) | 12 (40%) | ns |
| 3 | 15 (8%) | 11 (7%) | 4 (13%) | ns |
| 4 | ||||
| Single or multi-vessels diseased | 4 (2%) | 4 (3%) | 0 (0%) | ns |
| Single | 127 (71%) | 102 (68%) | 25 (83%) | ns |
| Multi-vessels | ||||
| Follow up (survival) | 53 (29%) | 48 (32%) | 5 (17%) | ns |
| Total events | 22 (12%) | 19 (13%) | 3 (10%) | ns |
Table 1: Clinical parameters across the total cohort and male and female populations.
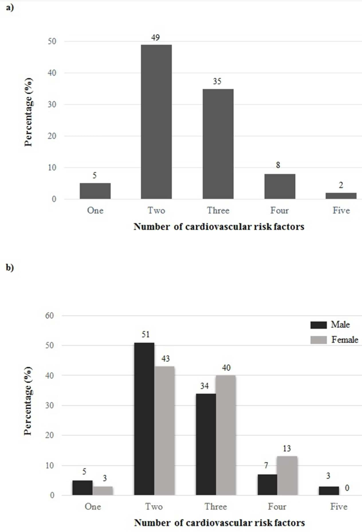
Figure 1: Percentage of outpatients presenting with one or more cardiovascular risk factors in total cohort (a) and by gender (b). Risk factors: dyslipidaemia, smoking, hypertension, diabetes, inheritance, and obesity (defined by BMI≥30 kg/m2) prevalence, abdominal obesity prevalence, diabetes prevalence, and smoking prevalence.
When considering the single CV risk factors, smoking was more frequent in male in respect to female (p<0>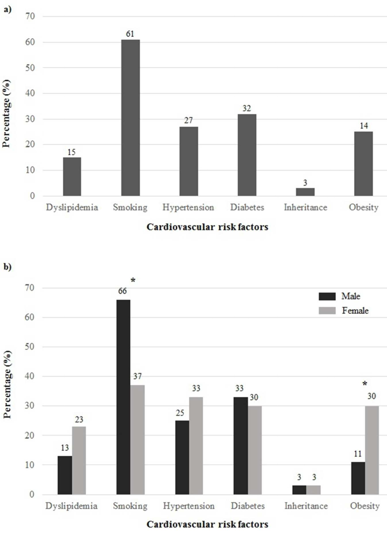
Figure 2: Overall prevalence of cardiovascular risk factors in total cohort (a) and by gender (b) * p<0>
The incidence of hypertension, diabetes and dyslipidemia was similar between male and female. Also, there was no difference in the incidence of CV between rural and urban patients (Figure. 3).
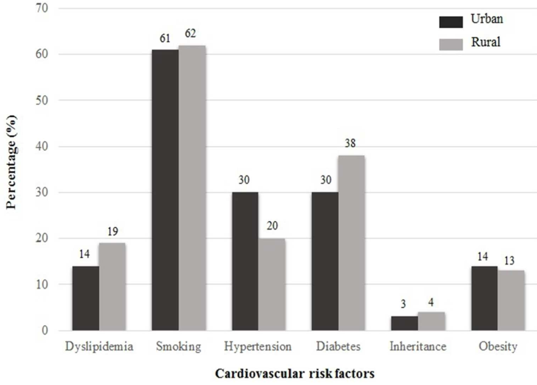
Figure 3 Overall prevalence of cardiovascular risk factors and total events in total cohort by location
In addition, the incidence of left ventricular ejection fraction <40>
Coronary Angiography and percutaneous revascularization.
All patients underwent coronary angiography without major complications. The incidence of single vessel as compared to multi-vessels disease was dominant both in female (83% vs 17%) and in male (68% vs 32%), respectively. There were 127 significant stenosis of left descending artery, 38 of circumflex artery, and 60 of right coronary. There were four stenosis of the left main.
PCI has been performed in all patients. The total number of PCI was 243; multiple PCI have been performed in 55 patients. The re-vascularized vessels were: 133 LAD, 45 CX and 65 DX. There was one death during PCI procedure. The rates of STENT usage were 94%, considering whole the group, without any difference between woman and men.
Follow-up data
Patients were followed up for 24±5 months. During the follow-up period, there were 22 events.
Out of these, there were 14 deaths, of which 11 were cardiac-related deaths and two non-cardiac deaths.
There were 8 non-fatal acute myocardial infarctions.
Total events occurred in 19 males and 3 in female (p=0.686).
When rural or urban location was considered, the number of events was significantly higher in the rural patients.
In the survival analysis, the only significant predictor of the considered events was the rural/urban location (p=0.04) where a rural location was associated with approximately 2.6-higher risk of death as compared to an urban location (OR=2.59, 95% CI:1.05-6.40).
This is the first study conduct in Mauritania in patients with documented CAD underwent PCI and STENT implantation. An important result of this study is that the mean age observed in both genders lines up to other African cohorts, and European and American ones, in which the increase in prevalence of CAD by age is around age sixty [9-11]. With regard to the incidence of CV risk factors, two points have to be underpinned: 1) the high incidence of diabetes and hypertension in the overall cohort; 2) the difference in risk factors incidence between male and female, with smoking higher in male, whereas obesity in female. These data confirm the results of a previous survey focusing on non-communicable disease in Mauritanian general population, committed by WHO, in which both genders showing a 22,4% mean incidence of hypertension, whereas the incidence of diabetes was around 6% [7].
The higher incidence of diabetes in our study in respect to STEP wise one is very likely due to the fact that our patients wereolder and with documented CAD, and thus more severely ill. Accordingly, in a cohort of patients with previous MI, enrolled in Tripoli, hypertension and diabetes were the more frequent risk factors with an incidence of 35% and 30% in male, and 46% and 32% in female. [12]. Furthermore, in the recent ACE Study, a higher percentage of dyslipidemia (about 70%) and hypertension (about 40%) and lower incidence of diabetes (about 25%) have been shown in respect to our data, evidencing specific needs for different subject cohorts living in different African areas [4].
In this context, ethnic heterogeneity, due to the different racial and geographic origins of populations belonging to the Arab North African (more studied) and black sub-Saharan subjects (lack of data), may confer highly variable risk for CV disease. In particular, although specific data for Mauritania are lacking, recent data evidenced that the prevalence of diabetes in the Mauritanian population could be higher respect to other African areas, with an elevated percentage of undiagnosed diabetes [13]. Risk transmission appeared preferentially maternal, as more probands with an affected mother than those who have a father with diabetes were found [13]. Moreover, specific gene variants (KCNJ11 E23K) have been identified, which may explain type 2 diabetes susceptibility in this population [14].
In respect to the lifestyle habits, the higher incidence of obesity in the women confirmed the results ofa recent study that reported the WHO estimates showing significant variations by sex, regions of the world and countries. Accordingly, in general almost 27% of African adults were overweight or obese with notable heterogeneity among countries with obesity being more common in females than in males [15]. Interestingly, the high incidence in African female may be also related to a cultural standpoint in which obesity is seen as a sign of wealth and an important attribute of beauty, in addition to the environmental and social changes due to urbanization, and to high socio-economic status, sedentary occupation and tertiary education. [16-19].
Another important result of this study is that patients living in rural places had higher incidence of events at follow up and, furthermore, living place resulted the only independent variable of considered events. This result may appear in contrast with the epidemiological transition in which disease profiles have been linked to urbanization and developments of societal aspects [20].
Generally, as population move from rural to urban settings, the burden of CV risk factors increase. While we observed a similar prevalence of cardiovascular risk factors in both environmental settings, probably due to the adoption of an “urban” lifestyle by rural communities, the key of the interpretation of a higher incidence of events in this population, may be the low availability of antiaggregants, and, mainly, the low awareness of the utility to assume daily this drug may be resulted determinant in the occurrence of cardiac events in the follow up. To this reason, the impossibility to assume antiaggregant therapy has been an exclusion criterion in this study.
There are several clinical questions raised up in this study. Revascularization procedures, performed by an expert Italian team of hemodynamists within an international cooperative educational program finalized to teach these procedures to Mauritanian hemodynamists, is a mandatory health policy in consideration of the dramatic increase of NCD, such as CAD, in African countries [21,22].
In this context, a recent position paper of the South Africa Heart Association pointed out the need totransform the healthcare system dealing with rapidly expanding epidemic of NCD including heart disease [23]. Therefore, in different African countries diagnostic and therapeutic facilities programmes are developing to deal with CAD patients [9]. This study shows the strength of Mauritanian health system to acquire the state of the art about treatment procedure to optimize cardiac patient care and cure.
In this view, the Mauritanian Government, aware of the magnitude and the public health importance of non-communicable diseases, and concerned about the accelerated increase in the prevalence of NCDs has approved AFRC/RC50/10, strategy of the WHO Regional Committee for Africa. The increasing clinical incidence of the conventional cardiovascular risk factors, in particular diabetes and hypertension, highlitghs the need of diagnostic and therapeutic facilities, and also the need to increase patient’s awareness on the potential CV harms [24-26].
Contexually, to increase support for the prevention, educational programmes are mandatory to defeat against dangerous lifestyle habits. [27]. Further, educational healthy programs should be oriented to genderpersonalization of CV prevention, in particular regarding life-style habits, to diffuse the availability of antiaggregant therapy and also the get patient’s awareness of the need to assume chronically this therapy.
The low number of patients did not provide us to detect independent variables of cardiac events in the follow up. Further, we did not consider variables potentially influencing CV risk profile. This, in particular at the light of a recent study from Uganda in which behavioral and socio-economic variables were included in a novel model framework for cumulative number of non-communicable disease risk factors [28].
Our study points out the strength of the Mauritanian Cardiology to develop diagnostic and therapeutic strategies to control coronary artery disease and its complications. This necessity is linked to the rapid urbanization, with consequent western lifestyle habits, similar to the developing countries, in which traditional risk factors are responsible for 80% of global deaths from CV disease [29,30].
Until recently, health improvement as a co-factor of economic development in Africa, had been perceived more in terms of improving maternal and child health, and controlling the commonest infectious diseases such as malaria, HIV/AIDS and tuberculosis. However, accumulating evidence supports the emergence of NCDs, many of which result from changes in lifestyle, as a major threat to the health of populations and economic development in many African countries.
Africa is a continent of great diversity, extending from highly industrialized cities where people follow an urban westernized lifestyle, to remote rural regions with traditional lifestyles; consequently, populations reflect different stages of the epidemiological health transition across Africa. Specific social, genetic, and life-style factors can affect the risk of CV disease, and must be known to correctly adapt international preventive plans to local needs. The evaluation of these aspects is mandatory to develop and target effectively health strategies and diagnostic screening and to support disease surveillance aimed at quantifying the burden and trends of NCDs, their risk factors, the quality of the management of cases and their major determinants in the Mauritanian population.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
