
Case Report | DOI: https://doi.org/ 10.31579/2639-4162/041
1 Consultant of Dermatology and Venereology, King Faisal specialized Hospital, Saudi Arabia.
2 Department of Forensic and Toxicology, Ain-Shams University, Egypt.
3 Faculty of Medicine, Ain-Shams University, Egypt.
4 Clinical Laboratory Department, College of Applied Medical Sciences, Taif University, Saudi Arabia.
5 Department of Medical Parasitology, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
*Corresponding Author: Khadiga Ahmed Ismail, Clinical Laboratory Department, College of Applied Medical Sciences, Taif University, Saudi Arabia. Department of Medical Parasitology, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
Citation: Caggiula A, Di Loreto M, Pettinicchio M, Vendrame A, Casu C. (2020) Central Giant Cell Granuloma: A Narrative Review Of Radiological Features And Differential Diagnosis. General medicine and Clinical Practice. 3(3) DOI: 10.31579/2639-4162/041
Copyright: ©2020 Khadiga Ahmed Ismail. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 September 2020 | Accepted: 26 September 2020 | Published: 02 October 2020
Keywords: COVID-19; coronavirus; skin manifestations
COVID-19 has high transmissibility and infectivity among human. On January 30, 2020, the World Health Organization (WHO) in an effort to slow down the global spread of the virus declared the outbreak, “A global public health emergency of international concern". The skin manifestations of the novel coronavirus COVID-19 were not recognized at the early stages of the pandemic but have received much recent attention in scientific journals. Reported manifestations range from pseudo-chilblains to a morbilliform (measles-like) exanthem, urticaria, vesicular eruptions, a dengue-like petechial rash and ovate scaling macules, and plaques mimicking pityriasis rosea.
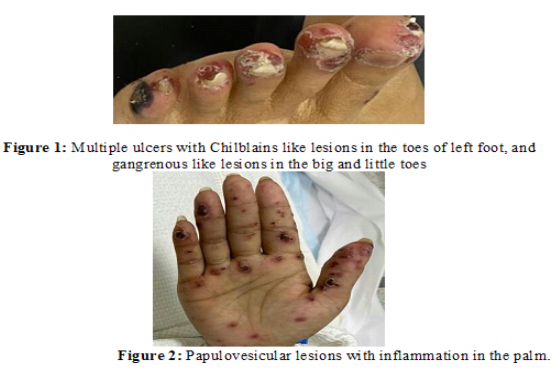
Female patient, 30 years old, presented to the Emergency Department with fever, dry cough, and dyspnea. She gave a history of contact with COVID-19 positive case, she developed maculopapular and vesicular lesions on both hands and feet, some lesions were blackish in color on the third day of admission to the hospital.
On Examination
She was febrile, her temperature was 38.8°C, her blood pressure was 100/70 mmHg with a heart rate of 90 beats/minute, respiratory rate of 27 breaths/minute, and oxygen saturation of 84% in room temperature air. She had maculopapular and vesicular lesions on both hands and feet, some lesions were blackish in color, as shown in figures 1 & 2.
Laboratory Investigations
As regards her complete blood count:White blood cell count (WBC) of 3.57 103/µL (L) (Reference Range:4 – 11 103/µL), with a mild leucopenia, mild relative monocytosis, and moderate absolute lymphopenia. Red blood cell count (RBC) of 3.36 106/µL (L) (Reference Range: 3.8-5.4 106/µL) with a hemoglobin of 10.9gm/dL (L) (Reference Range: 11.5-16gm/ dL), hematocrit of 32.4% (L) (Reference Range: 40-50%). Platelet count of 106 103 /µL (L) (Reference Range:150-450 103/µL).
As regards her chemistry:
Her random glucose of 70 mg/dL (N) (Reference Range: 70-140mg/dL), blood urea of 20.60mq/dL (N) (Reference Range: 20-48mq/dL), creatinine of 1.99 mq/dL (H) (Reference Range: 0.6-1.2mq/dL), SGOT(AST) (30µ/L) (N) (n 0-42µ/L), SGPT(ALT) (14µ/L) (N) (Reference Range: 0-33 µ/L).
As regards her coagulation profile:
Partial thromboplastin time (PTT) was (89.4 sec.) (H) (Reference Range: 26-40 seconds), Thromboplastin time (PT) of (16.60 sec.) (H) (Reference Range: 11-14.5 seconds), and INR of 1.30% (H) (Reference Range 0.8-1.2%).
RT-PCR positive for COVID-19
Discussion
Coronaviruses belong to the family Coronaviradae, order Nidovirales, and can be further subdivided into four main genera (Alpha-, Beta-, Gamma-, and Delta-coronaviruses). Several Alpha- and Betacoronaviruses cause mild respiratory infections and common cold symptoms in humans, whereas others are zoonotic and infect birds, pigs, bats, and other animals. In addition to COVID-19, two other coronaviruses, SARS-CoV and MERS-CoV, caused large disease outbreaks that had high lethality rates (10%–30%) and widespread societal impact upon emergence [1].
Currently in December 2019, a new infectious respiratory disease emerged in Wuhan, China that caused a severe respiratory illness which is now termed coronavirus disease discovered in 2019 or COVID-19 for short [2].
COVID-19 rapidly spread in china. This novel coronavirus is similar to SARS-CoV in their genetic information and it’s termed as SARS-CoV-2 and has caused a large global outbreak [3].
The first case reported was close contact with animals in seafood market that may transmit from animal to human, then it was transmitted from human to human [2].
The transmission of SARS-CoV-2 is through droplets or direct contact and the possibility of transmission by asymptomatic carrier. Due to the tenacity of the virus, it is possible that a person can acquire COVID-19 by touching a contaminated surface or object, and then touching his or her own mouth, nose, or eyes [3].
In February 11, 2020, the Chinese center of Disease Control and Prevention published 72,314 cases of COVID-19 [4].
Multiple skin manifestations have been described in patients with confirmed or suspected COVID-19 infection. These include a morbilliform rash; urticaria; pernio-like acral lesions; livedo-like vascular lesions; and vesicular varicella-like eruptions. A severe multisystem inflammatory syndrome with mucocutaneous, systemic, laboratory, and imaging findings of atypical severe Kawasaki disease has also been reported in children and adolescents with COVID-19 [5].
Differentional Diagnosis:
1- Perniosis and Pseudo-Chilblains (“COVID toes”) clinically presents as erythematous to violaceous papules over acral surfaces (usually the fingers and toes, less commonly the nose and ears) following exposure to cold (fittingly called “acrocyanosis”). Blistering, crusting, and ulceration can occur in severe cases [6].
2- Morbilliform Eruptions and Macular Erythema presented with pink-red macules and papules (morbilliform means “measles”-like) that most often arise on the trunk and then spread to extremities symmetrically [7].
3-Urticaria present as edematous, erythematous papules or plaques often with central pallor [8].
4- Vasculopathies, Livedo presented with livedo refers to a vascular reaction pattern that manifests as “mottling” of the skin, manifesting as a net-like/ reticular discoloration of the skin on the trunk and extremities [9].
5-Vesicular Eruptions present with either diffuse or localize vesicles refer to small fluid-filled skin lesions (< 1 cm). Lesions larger than 1 cm are referred to as bullae [10].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
