
Case Report | DOI: https://doi.org/10.31579/2642-9756/125
1 Department of Obstetrics and Gynecology, Danbury Hospital, Danbury CT.
2 Bhaktapur Cancer Hospital, Bhaktapur, Nepal.
*Corresponding Author: Anya Laibangyang, Department of Obstetrics and Gynecology, Danbury Hospital, Danbury CT.
Citation: Anya Laibangyang, Eliza Shrestha, Sanat Chalise, Linus Chuang. (2022). Cutaneous Metastsis of An Endometrioid Adenocarcinoma to The Face. J. Women Health Care and Issues. 5(5); DOI:10.31579/2642-9756/125
Copyright: © 2022 Anya Laibangyang, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 July 2022 | Accepted: 19 August 2022 | Published: 16 August 2022
Keywords: endometrial; adenocarcinoma; cancer; facial; metastasis; cutaneous
Background: Cutaneous metastasis is uncommon in endometrial cancer. Recurrence to the skin has been demonstrated to occur in the abdomen, pelvis and scalp. This is the first case presented of a cutaneous metastasis to the face.
Case: A 60-year-old Nepalese woman stage 1A grade 1 endometrial adenocarcinoma experienced metastasis to her external iliac lymph node 15 months after her initial presentation. After the recurrence was treated with chemotherapy, she experienced cutaneous metastasis of her endometrial carcinoma to her face 34 months after her initial surgery. The patient passed away 3 months after.
Conclusion: Endometrial adenocarcinoma can metastasize to the face and is associated with a poor prognosis
Endometrial cancer is the sixth most common cancer in women worldwide. [1] The most common presenting symptom of endometrial cancer is postmenopausal bleeding. Though nearly 70% of endometrial cancers are limited to the uterus at diagnosis, for the remaining, the most common locations of metastasis include the vagina, pelvic and para-aortic lymph nodes, peritoneum and the lungs. Less commonly, endometrial cancer can metastasize to the skin. [2] There have been several reported cases of cutaneous metastasis, particularly to the abdomen and scalp. [3] There have been no cases reported of endometrial cancer metastasizing to the face. We present a case of endometrial cancer with metastasis to the face.
A 60-year-old Nepalese nulliparous woman initially presented with complaints of intermittent postmenopausal bleeding for one month. Endometrial biopsy was obtained and revealed endometrial adenocarcinoma, endometrioid type, villoglandular variant. The patient underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic lymph node dissection and appendectomy. Surgical pathology confirmed the diagnosis and noted that the malignancy invaded less than half of the myometrium, with a maximum tumor dimension of 4.5 cm. Lympho vascular space invasion and perineural space were absent, and no tumor was found in the lower uterine segment, bilateral fallopian tubes and ovaries. Pelvic washings were positive for malignancy. The patient was staged as stage IA grade 1 endometrial adenocarcinoma. Chest X-ray done at the time was within normal limits. Her postoperative course was uneventful, and she was observed with close follow up. On routine CT imaging 15 months after her initial surgery, the left external iliac lymph node was noted to be enlarged, measuring 21x11mm. The patient underwent 6 cycles of carboplatin and paclitaxel as per request of the patient. Repeat imaging demonstrated a well-defined cystic lesion measuring 4.1x3.6x3.9 cm in the left external iliac region. Fine needle aspiration of the lesion demonstrated metastatic poorly differentiated adenocarcinoma. The patient received an additional 6 cycles of gemcitabine and carboplatin. The choice of chemotherapy regimen was limited by financial constraint. Imaging at this time demonstrated resolution of the lymph node. The patient continued with close follow-up and at 34 months after her initial surgery (19 months after completion of her second line of chemotherapy), the patient presented with respiratory difficulty and submandibular swelling (Figure 1)

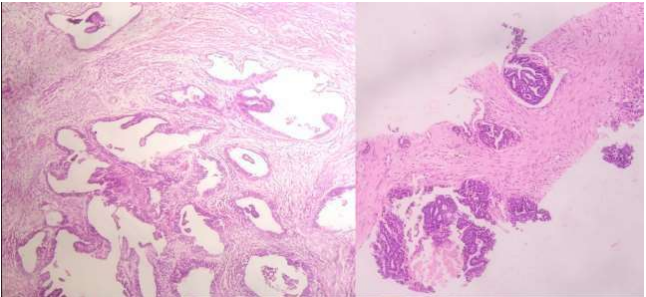
CT imaging demonstrated a right mandibular nodular lesion with multiple discrete nodules in the bilateral lungs. Fine needle aspiration of the right cheek mass was positive for malignancy suggestive of metastatic adenocarcinoma (Figure 2).
Though the pathology from the original surgery did not match that of facial metastasis, the likelihood of a second primary was low as the patient had no history of tobacco use, betel nut uses or other risk factors. The patient was followed by palliative care and after 3 months, passed away.
Endometrial adenocarcinoma is the most common gynecologic cancer, the five-year survival rate for patients with disease limited to the uterus is up to 95%. For patients with recurrence or disease outside the pelvis, the rate can be as low as 17%. [4] Cutaneous metastasis of endometrial cancer is rare, occurring in <1>
Cutaneous metastasis from endometrial cancer have been found in various sites, most commonly the abdominal wall, umbilicus and scalp. Other reported sites include the external genitalia, surgical site, and lower leg. [3] The lesions often vary morphologically and diagnosis should be confirmed with a tissue biopsy. In most cases, the metastasis is not limited to the skin and the patients present with widespread disease. This is the first reported case of an endometrial adenocarcinoma metastatic to the face. Her unusual site of recurrence in the face highlights the possibility of recurrence not limited to the lymph nodes, abdomen and lungs. In addition to the cutaneous metastasis, our patient also had metastasis to the lungs and retroperitoneal lymph nodes and after 3 months, succumbed to her disease.
Though this patient received adequate care in a prompt fashion, gynecologic cancer care in Nepal and other resource-constraint countries are not without its challenges. While endometrial cancer may be the most common gynecologic malignancy in the United States, this does not hold true in Nepal (and in low-resource settings) in which the most common gynecologic malignancy is cervical cancer. In Nepal, cervical cancer accounts for 16.4% of all cancer cases and 11.1% of all cancer deaths. [5] This is in stark contrast to endometrial cancer which accounts for less than 1% of all cancers in Nepal.
Patients receiving cancer care in these resource-constraint countries often face long wait times and prohibitive costs. Care is additionally limited by the lack of access to oncologists and health care. Though our patient was able to obtain care in a timely manner, her management plan did not adhere to standard practice due to financial constraints. In addition, her rapid demise after confirmation of her metastasis highlights the need for close follow-up in these patients and the importance of health care access. The poor prognosis in patient with cutaneous metastasis underscores the need for interdisciplinary management and initiation of a goals of care conversation to determine the next treatments, if any, the patient would like to pursue.
This case underscores the poor prognosis of endometrial carcinoma with metastasis to the skin. Currently, there are no definitive guidelines regarding treatment of endometrial adenocarcinoma with cutaneous metastases; often, patients in this late stage of the disease are treated with radiation and/or chemotherapy. Despite treatment, these patients often do not live past an additional year. The decision to pursue further clinical treatment should be made with a shared decision-making model involving the patient and all his/her healthcare providers. The goals of care should be clearly stated and the treatment plan (or lack thereof) should be made with these goals in mind.
The authors declare that there are no conflicts of interest regarding this article.
AL and ES contributed to the drafting of this manuscript. SC and LC critically revised and edited the manuscript.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
