
Research Article | DOI: https://doi.org/10.31579/2640-1053/234
1College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia
2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia.
3Princess Noorah Oncology Center, Jeddah, Saudi Arabia.
4Division of Dermatology, Department of Medicine, Ministry of the National Guard-Health Affairs, Jeddah, Saudi Arabia.
*Corresponding Author: Abdulhadi Jfri, MD, MSc, FRCPC, FAAD. Assistant professor of dermatology, College of Medicine, King Saud Bin Abdulaziz University for Health Sciences of Medicine Jeddah, Saudi Arabia.
Citation: Noura E. Aljehani, Farah A. Turkistani, Mays K. Alzahrani, Joud H. Damanhuri, Marya H. Shaheen, et al, (2025), Cutaneous Immune-Related Adverse Events due to Immune Checkpoint Inhibitors: A Clinical Phenotype-Cancer Subtype Association, J. Cancer Research and Cellular Therapeutics. 9(3); DOI:10.31579/2640-1053/234
Copyright: © 2025, Abdulhadi Jfri. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2025 | Accepted: 07 April 2025 | Published: 29 April 2025
Keywords: immune checkpoint inhibitors; cutaneous immune related adverse events; anti-PD-1; anti-PDL-1; anti-CTLA-4; drug reaction
Background and Aim
Immune checkpoint inhibitors (ICIs) block the interaction of checkpoint proteins, increasing the anti-tumor response from T lymphocytes. However, because this response is nonspecific, it can cause skin damage, resulting in cutaneous immune-related adverse events (cirAEs). In this study, we aimed to investigate the association between the cirAEs phenotype and cancer subtype at our oncology center.
Materials and Methods
This is a retrospective single-center study conducted at the Princess Noorah Oncology Center in Jeddah, Saudi Arabia. It included all adult patients receiving ICI as cancer therapy from January 2016 through September 2023. Data were analyzed to evaluate the prevalence and phenotypes of cutaneous immune-related adverse events (cirAEs), treatment outcomes, and cancer subtypes. Chi-square and Mann–Whitney U tests were used to assess associations between cirAE status and categorical or continuous variables (age, BMI), respectively. Statistical significance was set at p < 0.05. Analyses were performed using JMP software, version 10.0 (SAS Institute Inc., Cary, NC, USA).
Results
Out of 201 patients, 116 were male (57.7%), 85 were female (42.3%). The prevalence of cirAEs was 36–17.9%; the most common culprit drug was pembrolizumab. Most genitourinary malignancies (N = 10, 27.78%). The most common cirAE clinical phenotype was ulceration (36%), and the median cirAEs from initiation of ICI were 53.5 days.
Conclusion
ICIs have been associated with the development of cirAE in 17.9% of our cancer patients, with ulceration being the most common phenotype and pembrolizumab being the most common culprit medication. The cirAE was mostly prevalent among patients with genitourinary cancers. Further prospective studies are needed.
Immune checkpoint inhibitors (ICIs); immune-related adverse events (irAEs); cutaneous immune-related adverse events (cirAEs); cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4); anti-programmed death 1 agents (anti-PD-1); anti- programmed cell death ligand agents (anti-PDL-1)
The immune system defends the body and maintains health by distinguishing between self and non-self-cells (1).Normally, the body uses molecules called immune checkpoints expressed on body cell surfaces to modulate the level of immune response. Tumor cells, however, evade the immune system’s surveillance by expressing these molecules which sends inhibitory signals to T lymphocytes and decreases the anti-tumor immune reaction [2]. By targeting these compounds in treating cancer, Immune Checkpoints Inhibitors (ICI’s) have opened the door for long-term survival for patients with metastatic illnesses. ICIs are immunotherapy medications that stop checkpoint proteins from interacting with their targets resulting in an intensified anti-tumor response, T cells can then destroy cancer cells or slow the proliferation, which stops the inhibitory signal from being transmitted by cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1) [2].ICIs encompass anti-programmed death 1 agents (anti-PD-1) which includes Nivolumab, Pembrolizumab, Cemiplimab, and Dostarlimab. Another example is Ipilimumab known as a anti-cytotoxic T lymphocyte-associated 4 antigen (anti-CTLA-4). Lastly, Atezolizumab, Avelumab, and Durvalumabare anti- programmed cell death ligand agents (anti-PDL-1) [1].
Since ICIs cause nonspecific activation of the immune system, which amplifies the immune reaction against healthy cells, they have been associated with cutaneous immune-related adverse events (cirAEs), mainly damaging the skin and its appendages [3,4]. Moreover, the choice of drug can significantly impact the likelihood of cirAEs. A study found that combination therapy of anti-CTLA-4 and anti-PD-1 resulted in the highest level of immune-related adverse events (irAEs) incidence (59 –72%), whereas monotherapy had the least occurrence of irAEs. In addition, anti-CTLA-4 was associated with 44-59% of irAEs, as opposed to anti-PD-1 which was exclusively associated with 20% of irAEs[5–7].
Eczematous dermatitis, which is a prevalent side effect of anti-PD-1 therapy, and lichenoid, both affecting 17% of patients, are the most common rahses linked to cirAEs [8]. Additionally, vitiligo can occur in 2-9% of patients receiving anti-CTLA-4 medication, while pruritus affects 14–47% of patients receiving the same treatment [8]. Morbiliform eruptions on the trunk and extremities might affect 10–50% of patients undergoing the anti-CTLA-4 therapy as well [8]. It is worthy to note that even though most cases report to be easily controlled, a severe reaction and a reduction in a patients’ quality of living is possible, resulting in a need to bring the treatment to an end [4]. That being said, the effectiveness of ICIs and irAEs has been investigated in 52 research, 51 of which found a positive correlation [9].
Although the association between cirAEs and ICIs has been previously inspected, the association between the clinical phenotype of the cirAEs, cancer subtype, and the given ICI has not yet been explored thoroughly. Melanoma, a type of skin cancer, is the most common skin cancer treated with ICI and is therefore linked to the most severe cutaneous side effects in cancer patients [10]. This cannot be said about other types of cancer. Therefore, additional study is required to clarify the relationship between the cancer phenotype and a particular cutaneous side effect in patients receiving ICI.
This study aims to investigate the relationship between cirAE phenotypes and cancer subtypes in patients receiving immune checkpoint inhibitors (ICIs) at our oncology center. The goal is to enhance clinical outcomes and support the development of more effective cancer management strategies by improving the prediction and recognition of cirAEs based on cancer subtype and ICI type.
Study Setting:
This study was a single center observational retrospective cohort study conducted at Princess Noorah Oncology Center (PNOC), King Abdulaziz Medical City-Jeddah (KAMC-J), Jeddah, Saudi Arabia.
Inclusion and Exclusion Criteria:
Inclusion criteria for this study encompassed all adult oncology patients who presented at PNOC between January 2016 and September 2023, received immune checkpoint inhibitors (ICIs) as their main cancer treatment, and experienced cutaneous immune-related adverse events (cirAEs) as a side effect of their therapy. However, patients whose charts lack rash details or those who only experienced non-cutaneous manifestations of immune related adverse events (irAEs) were excluded.
Sample size and Sampling Technique:
Data from 201 patients receiving ICI for cancer treatment was collected using a consecutive sampling technique, the patients’ data was gathered through the hospital's electronic records.
Data Collection Tools:
The study variables were categorized into four sections in the data collection sheet. The demographic variables included patients’ age (years), weight (kg), height (cm), BMI (kg/m2) and gender. The cancer related variables involved the cancer diagnosis, the cancer stage, the type of immunotherapy administered, and whether it was monotherapy or combination therapy. The rash related variables encompassed the rash’s morphology, any concurrent irAEs, the treatment of the rash, and whether the immunotherapy was held due to the rash, and the duration it took for the rash to appear and resolve. The prognostic factors included what occurred to the patient prior to and after the rash’s resolution. These variables were then entered into an excel sheet.
Ethical Consideration:
An Institutional Review Board approval was acquired, as a result of the study being a chart review thus no consent form was needed.
IRB Study Number: SP22J/151/12, Approval Date: 31/12/2022, Institution: KAIMRC
A non-parametric approach was used to describe numerical variables (such as duration to cirAEs occurrence and its resolution) as median and interquartile range (IQR). Additionally, categorical variables (gender, cancer diagnosis and stage, mode of therapy, type of therapy, cirAEs morphology, cirAEs treatment, status of ICI post-cirAEs presentation, and concurrent irAEs) were presented as frequencies and percentages. Chi-square test was used to compare between the patients with cirAEs and those with no cirAEs in relation to other variables (demographic, cancer, medication variables). Mann-Whitney U test was also utilized to compare between the mean and standard deviation of those with cirAEs and those with no cirAEs’ ages (years) and BMI (kg/m2). A p-value of less than 0.05 was considered to be statistically significant. The statistical analysis was preformed using JMP software (John's Macintosh Project), version 10.0 (SAS Institute Inc., Cary, NC, USA).
Retrospective chart review of N=201 cancer patients receiving ICI for their cancer therapy indicated that N=36 (17.9%) presented with cirAEs. Females had a significant association with cirAEs (N=22; 61.11%, p-value=0.0116). On the contrary, males who developed cirAEs accounted for 38.89% (N=14, p-value= 0.0116). Additionally, the mean age of those with cirAEs was 54.361 ±17.98 years, whereas those who did not experience cirAEs 59.745±14.69 years (p-value= 0.185). Patients BMI was also similar between the 2 groups (with cirAEs and without cirAEs) with the BMI being 27.086±6.505 kg/m2and 25.25±5.82kg/m2 respectively (p-value=0.083). Majority of the patients were receiving ICI for stage IV cancer with N=17 patients (47.22%, p-value= 0.175) experienced cirAEs, and N= 90(54.55%, p-value= 0.175) did not experience cirAEs. For most of the patients, a combination of treatments was administered. For clarification,27 patients (75%, p-value=0.402) presented with cirAEs and 112 patients (67.88%, p-value=0.402) did not present with cirAEs. Table (1).
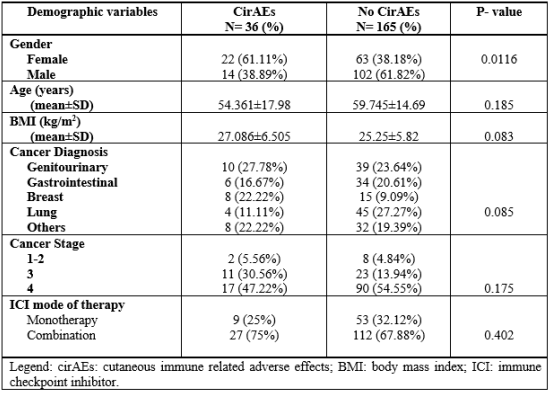
Table 1: Patients’ demographics, cancer and medication variables using Chi-square test and Mann-Whitney U test.
The most common cancer in those with cirAEs was genitourinary (N=10, 27.78%, p-value= 0.085) followed by breast cancer (N= 8, 22.22%, p-value= 0.085). On the other hand, the most common cancer in patients without cirAEs was lung (N= 45, 27.27%, p-value= 0.085), followed by genitourinary (N= 39, 23.64%, p-value= 0.085). Table (1), Figure (1)
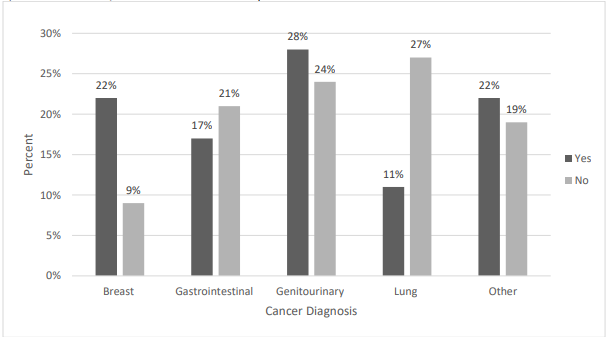
Figure 1: Illustrates the relation between malignancy subtypes and the presence of cutaneous immune related adverse events (cirAEs).
Those with cirAEs presented with a range of rash morphologies; the most prevalent rash morphology was ulceration N=10(27%) followed by plaques N=7 (19.44%), while the least common were papules N=4 (11.11%) and hyperpigmentation N=4 (11.11%). The median number of days between starting the treatment and the onset of the cirAEs was 53.5 days (IQR=213), and the median duration to the resolution of the cirAEs was 3 weeks (IQR=5.5). After developing rashes, the majority of patients N=28 (73.68%) continued receiving their therapy. Out of those who developed cirAEs, patients receiving anti-PD-1 and anti-PDL-1 accounted for N=33 (92%) and N=3 (8%) respectively. Table (2)

Table 2: CirAEs sub-analysis
The bulk of patients who developed cirAEs N=29 were taking Pembrolizumab (an anti-PD1 agent), four patients were using Nivolumab (anti-PD1 agent), and three patients were taking Atezolizumab (anti-PDL1 agent). The most common rash morphology among patients taking anti-PD-1 was ulcers (36%) followed by plaques (20%). Patients taking anti-PDL-1 presented with plaques (8%) and ulcers (4%). However, none of the patients receiving the anti-CTLA-4 medication (Ipilimumab) experienced cirAEs. Figure (2), Figure (3)

Figure 2: Demonstrates the type of immune checkpoint inhibitors (ICI) administered and presentation of cutaneous immune related adverse events (cirAEs).
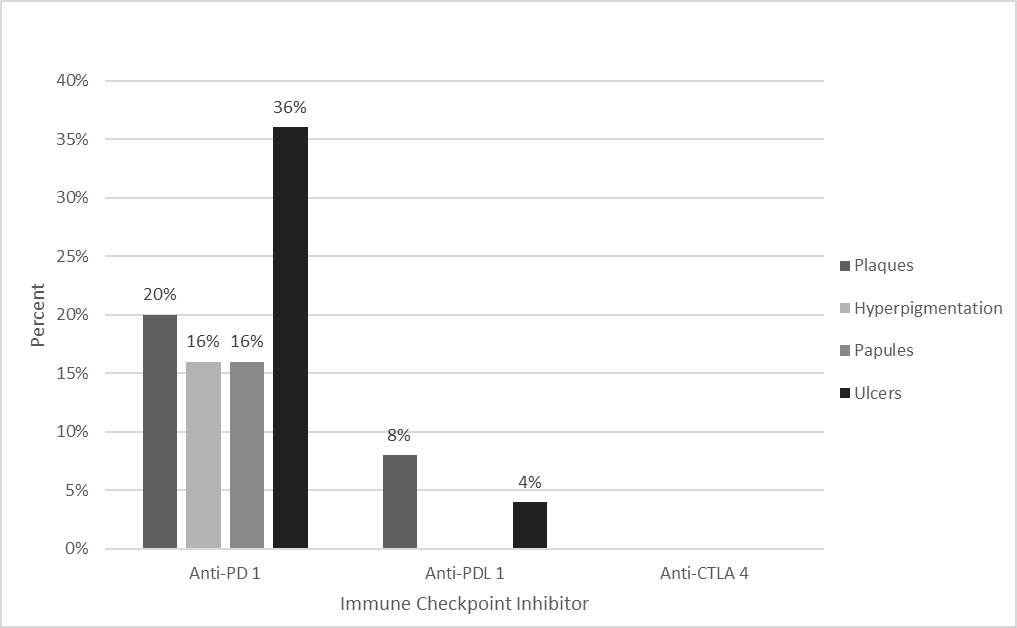
Figure 3: Compares between the morphology of cutaneous immune related adverse events (cirAEs) and the category of immune checkpoint inhibitor (ICI) administered.
The use of immunotherapies has increased in recent years, showing efficacy in advanced malignancies. However, ICIs are associated with notable adverse effects, particularly cutaneous toxicities. This study aimed to investigate the incidence of cirAEs associated with ICI therapy at our institution, characterize their clinical presentations and phenotypes, and evaluate patient survival outcomes in relation to cirAE development and management within the context of active malignancy. Our data indicated that a significant proportion of patients receiving ICIs developed cirAEs ranging in severity, with greater severity observed in those with grade III and IV malignancies, likely due to their compromised immune function. An earlier study conducted in January 2016 to December 2018 at the Oncology Centre of King Abdulaziz Medical City in Riyadh aimed to evaluate the safety of ICIs and identify the adverse events resulting from them. This study corroborates our findings, revealing that a similar percentage of individuals, specifically 15%, who underwent treatment with anti-PD1 medication exhibited cutaneous reactions(11). Despite our data reporting the highest exhibition of dermatological side effects while using pembrolizumab, Kichenadasse et al. describes atezolizumab as the most frequently associated drug in developing cirAEs[12].
Our study has also reached to a conclusion that the cutaneous immune related adverse effects appeared after approximately 2 months of receiving the immunotherapy doses, however other studies suggested that these side effects progressed after the first six months of the initiation of the immunotherapy [13]. Moreover, the findings show genitourinary cancer as the most frequent cancer subtype exhibiting cirAEs. As observed, females had a slightly higher risk of developing irAEs compared to males in our sample. After the treatment is administered, four out of 36 of the patients developed diseases associated with the thyroid, immediately followed by pneumonitis, equal to a comprehensive study conducted by Kichenadasse et al.[12]. However, ICI-induced endocrine disorders may exhibit a delayed onset after anti-PD1 therapy administration. For this reason, identifying thyroid dysfunction caused by ICIs is challenging [14].
Furthermore, rashes of unspecified morphology were reported in 30.5% of patients secondary to PD-1 inhibitors, forming the majority of our population. Of the irAEs found in our study, eruptions of ulcers and plaques were also seen but lesser in frequency, while hyperpigmentation and papules were the least reported skin manifestations. In contrast to our study, other articles showed the opposite; identifying among the various cutaneous side effects associated with ICIs, maculopapular rash stands out as the most frequently observed adverse reaction [15]. Contrary to previous studies, our study findings revealed a contrasting pattern regarding the manifestation of immune-related adverse events associated with anti-PD1 immunotherapy. Specifically, while vitiligo and lichenoid reactions were reported as the most concurrent irAEs in previous studies [16], our study demonstrated that these reactions were the least frequently observed irAEs. As for the intervention of these cirAEs, a notable subset of cases, approximately 26.3%, necessitated the discontinuation of the specific treatment used due to severe skin manifestations.
In addition, similar findings documented by Sanlorenzo et al. revealed the vast majority of patients with mild symptoms can be treated with topical corticosteroids, and only 13.8% of patients needed systemic steroid treatment. Several large-scale studies have consistently reported a significant improvement in treatment efficacy among patients who developed irAEs. Notably, a remarkable 26% of patients who experienced any form of irAE demonstrated positive treatment responses, while a mere 2% of patients without cirAEs exhibited similar responses [17].
It is important to discuss and acknowledge some of the limitations present in our study, with the most notable being the absence of documented assessments of patients' rash severity using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 grading system. The lack of a defined evaluation metric limits our capacity to draw conclusive and complete conclusions from the data collected within our sample population. Consequently, the interpretability and generalizability of our findings are limited. Considering this limitation, we recommend subsequent studies prioritize the use of validated grading techniques, such as CTCAE v5.0, in order to accomplish more robust and conclusive findings.
To conclude, ICIs increase the likelihood of developing a variety of cirAEs including ulcers, plaques, hyperpigmentation, and papules. Moreover, receiving anti-PD-1, specifically Pembrolizumab, is linked to the highest risk of developing cirAEs and it was mostly prevalence among genitourinary cancer patients. Further studies are needed to assess the status of malignancies following the development of these cirAEs.
The authors declare that there are no conflicts of interest related to the conduct of this research
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
