
Research | DOI: https://doi.org/10.31579/2693-4779/105
1 Laboratory Service, National Hospital Center of Nouakchott, Mauritania.
2 Faculty of Medicine of Nouakchott, Mauritania.
3 Internal Medicine Service, National Hospital Center of Nouakchott, Mauritania.
*Corresponding Author: Mohamed Lemine Ould Salem, Laboratory Service, National Hospital Center of Nouakchott, Mauritania, Microbiology Laboratory, Nouakchott Faculty of Medicine.
Citation: Mohamed Lemine Ould Salem, Fatimettou Abdellahi, Mohamed Ahmed MM Sidiya, Sidi Mohamed Ghaber, Sidi El Wafi Ould Baba. (2022) Current state of resistance to antibiotics inenterobacterialisolated at the National Hospital Center of Nouakchott-Mauritania. Clinical Research and Clinical Trials. 6(3); DOI:10.31579/2693-4779/105
Copyright: © 2022 Mohamed Lemine Ould Salem. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 June 2022 | Accepted: 28 June 2022 | Published: 22 July 2022
Keywords: enterobacteriaceae; e. coli; antibiogram; nouakchott; mauritania
Enterobacteriaceae are Gram-negative bacteria, facultative aero-anaerobes found everywhere. They include a very large number of genera and species. Their abundance in the intestine, their mobility, the rapidity of their multiplication, the frequent acquisition of mechanisms of resistance to antibiotics.
Objective : The objective of this study was to investigate the antibiotic susceptibility of Enterobacteriaceae strains isolated from various infectious sites in outpatients and hospitalized patients.
Material and method: This is a prospective study carried out in the central laboratory of the Nouakchott Hospital Center and involving 300 strains of enterobacteriaceae isolated from various samples taken from different departments or external consultations. The study was conducted from November 1, 2020 to July 30, 2021
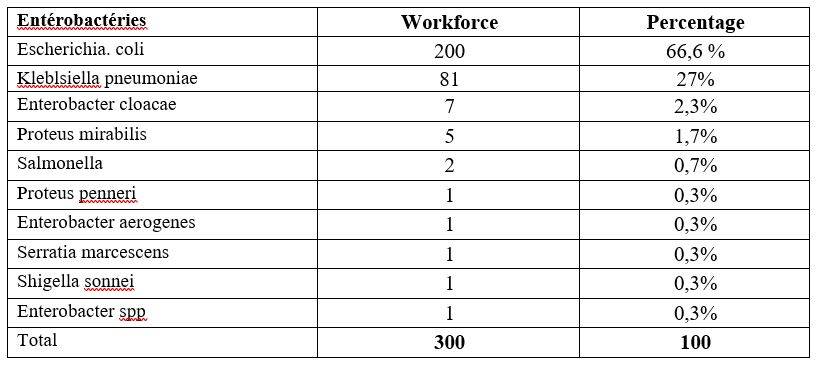
Results : In our study E. coli represents (66.6%), followed by K. pneumoniae (27%), E. cloacae (2.3%). The study of the resistance of these strains to antibiotics revealed resistance rate: Amoxicicillin (93%), Amoxicillin-clavulanic acid (77.6%), Gentamicin (16%) and (9.4%) Fosfomycin.
Conclusion : The significant increase in the frequency of enterobacteriaceae has become worrying in both hospital and community settings. However, implementation requires collective awareness through in-depth training of healthcare teams. Currently, the reference treatment for infections due to multiresistant enterobacteria is essentially based on the use of carbapenems. It is nevertheless fundamental to obey a rational prescription of these antibiotics to limit the emergence of carbapenemase-producing strains. Controlling the spread of enterobacteriaceae requires strict compliance with simple hospital hygiene measures.
Enterobacteriaceae are Gram-negative bacteria, aero-facultative anaerobes found everywhere in soil, in water and especially in the intestine of humans and animals. They include a very large number of genera and species. Their abundance in the intestine, their mobility, the speed of their multiplication, the frequent acquisition of antibiotic resistance mechanisms explain why they are the bacteria most involved in human infectious pathology, especially in the hospital environment [1]. The majority of urinary tract infections have a bacterial origin, and the most frequently encountered pathogens are enterobacteriaceae.[2].Escherichia coli is the most incriminated germ; it is responsible in 85% of cases, Klebsiella pneumoniae comes in second position with 10% of cases, Proteus mirabilis comes in third position with 4% of cases, other Gram-negative bacilli (Pseudomonas aeruginosa) or Gram-positive Cocci ( Staphylococcus saprophyticus, Staphylococcus aureus, Enterococcus sp) may less often be the cause [3]. Literature data show that Escherichia coli is the predominant bacterium in UTI [4]. About 150 million cases of urinary tract infections per year in the world, they constitute as such a public health concern [5]. Enterobacteriaceae are implicated in pneumonia, mainly in a nosocomial context of ventilator-acquired pneumonia and aspiration pneumonia [6]. Escherichia coliwas the leading cause of bacteriemia in France, ahead of Staphylococcus aureus [7] The Global Antimicrobial Resistance Surveillance System (known as GLASS) reveals that antibiotic resistance is a widespread problem affecting 500,000 people with suspected bacterial infections in 22 countries. It is also reported that the most frequently reported resistant bacteria include Escherichia coli; Klebsiella pneumoniae; Salmonella spp [8]. In Europe, the European Center for Disease Control (ECDC) has estimated the number of deaths resulting from antibiotic resistance at 25,000 per year [9]. Around 700,000 people worldwide die each year from drug-resistant infections and, if left unchecked, these infections are estimated to cause 10 million people to die annually by 2050. The situation is alarming in countries with limited resources where infectious diseases, poverty and malnutrition are endemic. The emergence of antibiotic resistance is a complex process often involving host, pathogen and environmental factors. In recent years, an increase in the incidence of resistance to antibiotics of germs responsible for urinary tract infections has been observed. The outbreak of Extended Spectrum Beta-lactamase (ESBL)-secreting Enterobacteriaceae is increasingly prevalent [10]. In West Africa, as throughout the world, antibiotic resistance mainly concerns bacteria producing ESBL [11]. The causes of the emergence and dissemination of this resistance are multiple, but the excessive and/or inappropriate use of these antibiotics is, without a doubt, the main reason for this evolution. This evolution of resistance is unpredictable and should prompt regular monitoring of the sensitivity of the predominant bacterial species to the various antibiotics used [12]. It is in this context that our study was carried out with the aim of:
Epidemiological study of the prevalence of enterobacteriaceae isolated from various infectious sites in outpatients and hospitalized patients.
Prevalence of resistance of Enterobacteriaceae to antibiotics.
II.1. Place of study:Our study was conducted in the central laboratory of the National Hospital Center of Nouakchott (CHN).
II.2. Study period :
Our study was spread over a period of nine months from November 1, 2020 to July 30, 2021.
II.3. Type of study :
It's about aobservational descriptive study.
Data collection was done using a survey form.
II.4. Nature of samples studied:
The strains were isolated from different samples : Urine (ECBU), Pus, blood cultures, genital samples
II.5. Inclusion criteria :
The study covers all bacteriological samples for diagnostic purposes received at the Central Laboratory of the National Hospital of Nouakchott (CHN) from hospitalized patients or outpatients.
II.6. Exclusion criteria :
Duplicate strains : strains isolated from the same patient, at the same anatomical site.
II.7. Services originating from strains :
The samples were sent by the various departments of the hospital and the consultations on an outpatient basis.
II.8. Identification of bacteria :
The identification was made either by thePLC system (Biomérieux®) or automatically on the Vitek-2 automaton (Biomérieux®)
II.9. Antibiotic sensitivity study :
The antibiogram is carried out by the agar diffusion method (disc method) or automatic method on Vitek-2 (Biomérieux®), according to the press release from the antibiogram committee of the French microbiology society (EUCAST CA-SFM) .[13]
III-1 Epidemiological Data
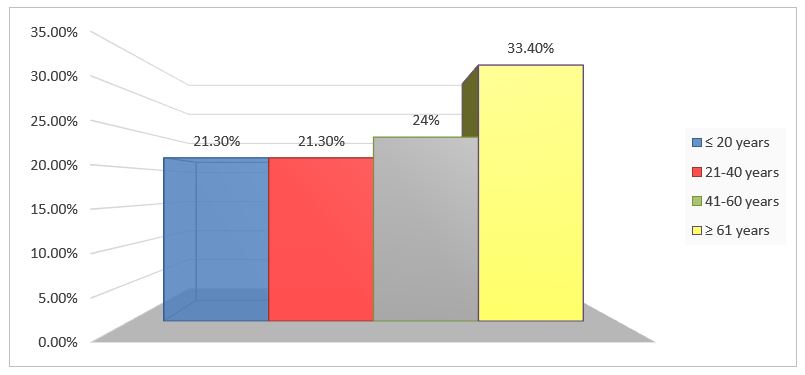
III-1-1 Age
The average age was 41.8 years with extremes of 1 and 83 years.
Figure 1 shows the distribution of patients by age group.
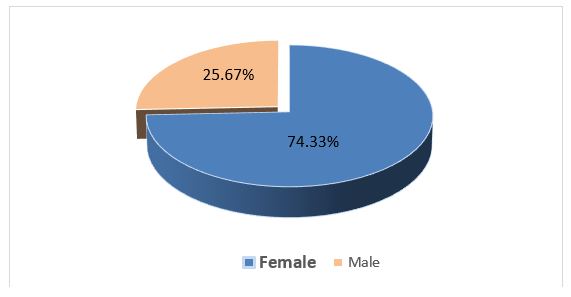
III-1-2 Sex
The sex ratiowas 0.34 in favor of women
Figure 2 shows the distribution of patients by sex
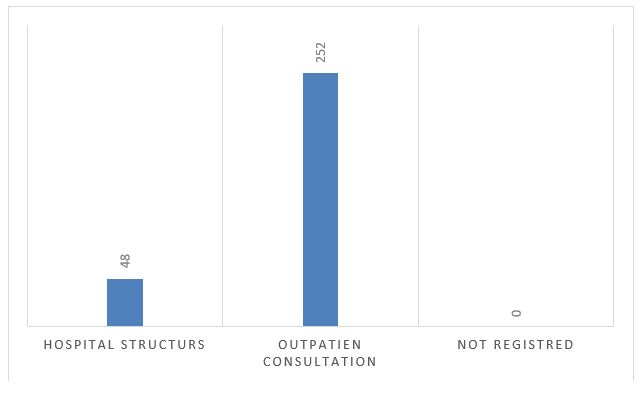
III-1-3 Origin of provenance
Figure 3 shows the distribution of patients according to their origin of origin
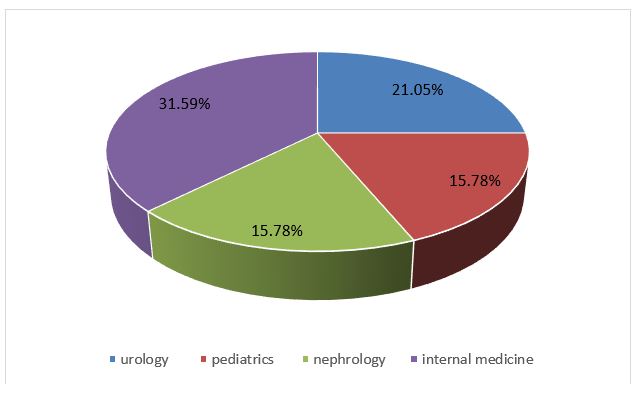
III-1-4 Patient hospitalization services
Figure 4 shows the distribution of patients according to reception services
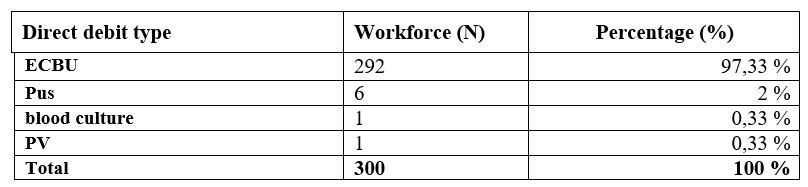
III-1-5 Types of samples
TableIshows the distribution of patients according to the type of sample
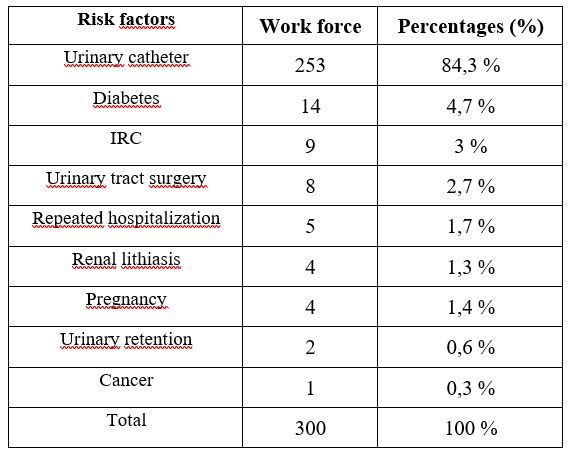
III-1-6 Facteurs des risques :
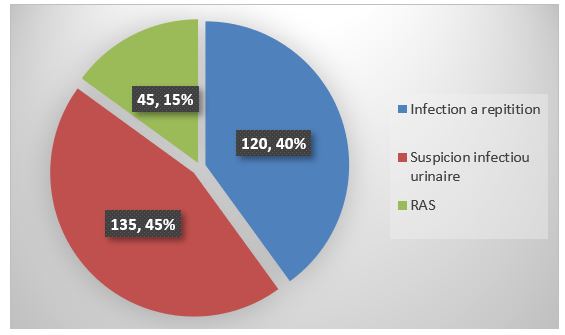
III-1-7 Breakdown of patients according to ECBU indication
III-2 Bacteriological data
III-2-1 Overall distribution of enterobacteriaceae isolated according to bacterial species
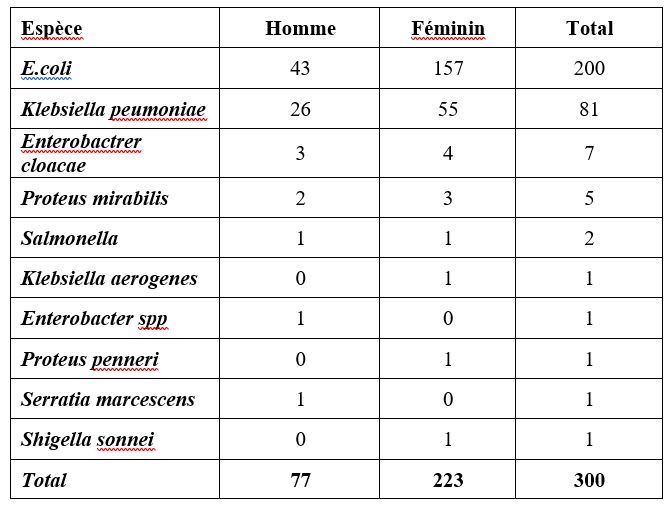
III-2-2 The distribution of bacterial species according to sex
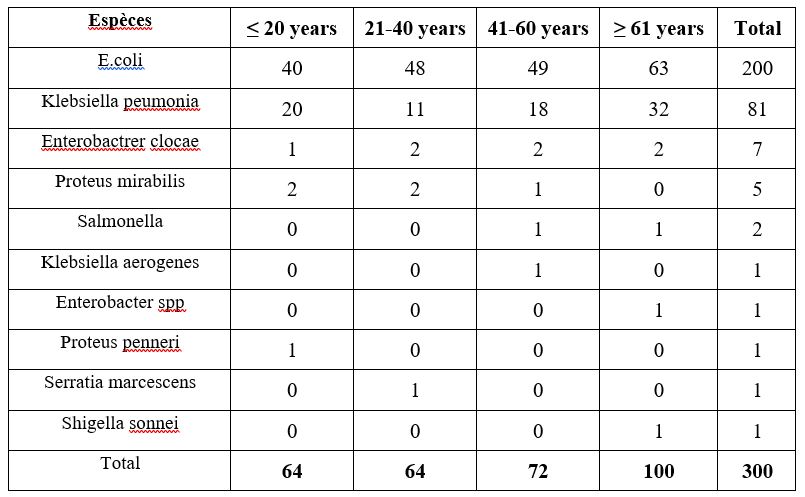
III-2-3 The distribution of bacterial species according to age
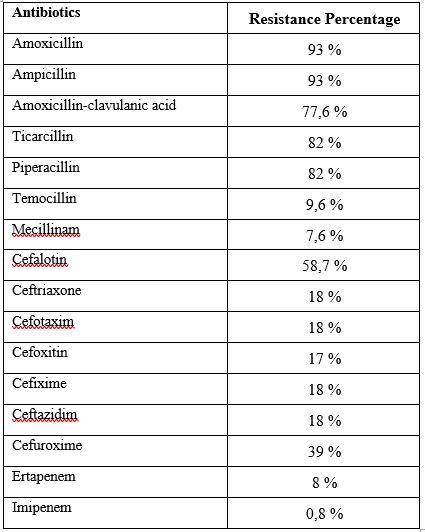
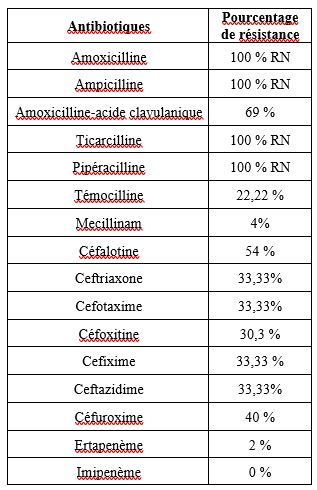
III-2-4 Beta-lactam resistance profile of E.coli
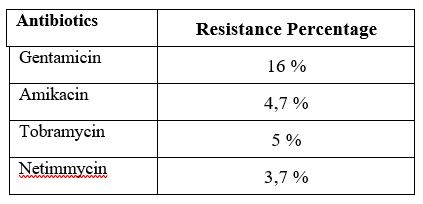
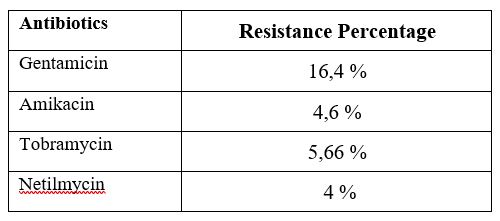
III-2-5 Resistance of E.coli to aminoglycosides
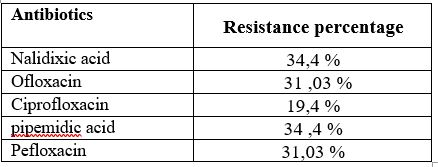
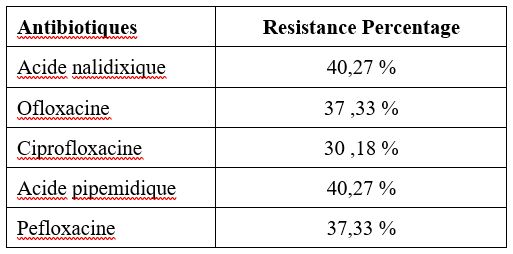
III-2-5 Resistance of E.coli to quinolones:
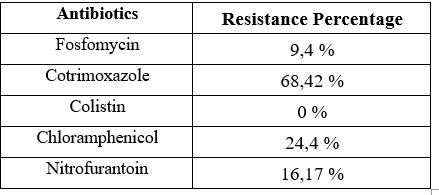
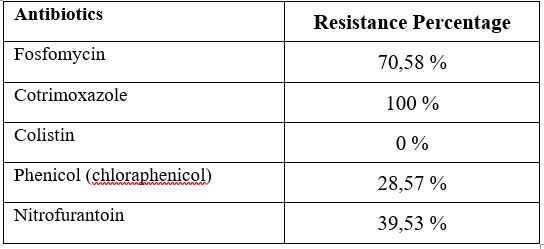
III-2-5 Resistance of E.Coli to other antibiotics:
III-2-6 Resistance of Klebsiella pneumoniae to beta-lactams:
III-2-7 Resistance of Klebsiella pneumonia to aminoglycosides, quinolones and other antibiotics:
Tables XI, XII and XIII show the resistance of Klebsiella pneumonia to aminoglycosides, quinolones and other antibiotics.
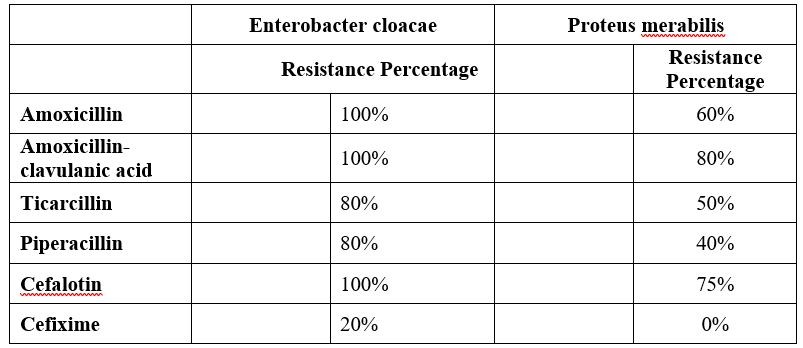
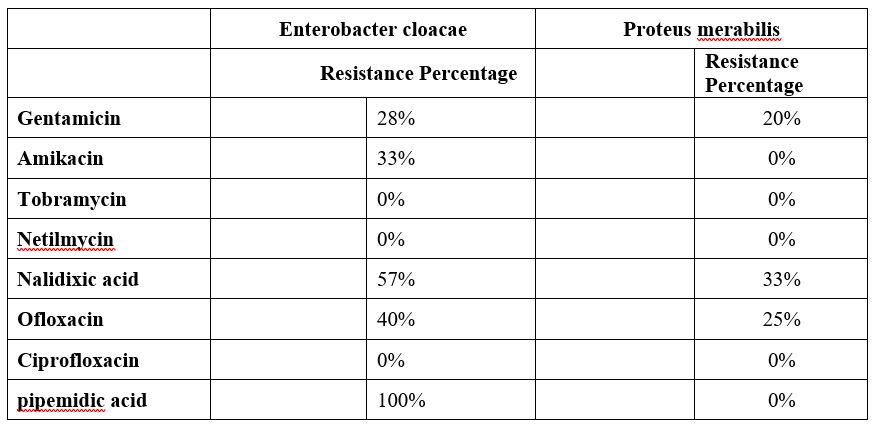
III-2-8 Resistorsof Enterobacter cloacae, Proteus mirabilis to beta-lactams and aminoglycosides:
Resistance of other Enterobacteriaceae:
In our series we have 2 strains of salmonella which were resistant to amoxicillin, Ticarcillin, Piperacillin, no resistance to aminoglycosides or quinolones.
We have a single strain of Proteus penneri which was resistant, in addition to its natural resistance (to amoxicillin, C1G, cefuroxime) to Ticarcillin, amoxicillin+clavulanic acid, and to C2G while it was sensitive to C3G and all aminoglycosides and quinolones.
Our series contains a single strain of Klebsiella aerogenes that was resistant to C3G susceptible to aminoglycosides and quinolones.
For serratia marsescens we have a single strain which was resistant to the betalactamines tested (except carbapenems) while it was sensitive to aminoglycosides and quinolones.
IV-1 Epidemiological data:
IV-1-1 Age:
In our study the average age was 41.8 years with extremes of 1 and 83 years. The most affected age was over 61 with a percentage of 33.4%.
These results could be explained by the fact that these people are more vulnerable to infections because of the fragility of their immune system.
In a study carried out in the bacteriology-virology department of the National Institute of Public Health (INSP) in Bamako, a high frequency of positive ECBU was found in elderly patients (age > 60 years) with 30.4% of case or 183 samples. The average age of this study was 46 years (for the 567 samples whose age was entered) with the extremes ranging from 1 to 96 years[14].In 2017 a study by SABOR et al. showed that people over 60 were the most represented with a percentage of 25.37%.[15].In 2005 Zhanel et al in North America found a predominance of this same category in their studies with rates of 34.1%[16].
IV-1-2) Gender:
In our study, we found a female predominance giving a percentage of 74.3% with a sex ratio of 0.34. A study carried out by KALAMBRY in 2019 in Mali shows a female predominance with 54.2% of positive ECBU among women (326 out of 602 ECBU positives) and 43.0% in men (276 out of 602 ECBU positives) with a sex ratio of 1.18. This same observation has been made by other studies[17].Another study conducted in Morocco by Lahlou Amine also showed a female predominance with a female/male sex ratio of 1.08 (hospitalized: 0.52 and consultants: 1.48)[18] A studycarried out at the bacteriology-virology department of the National Institute of Public Health (INSP) in Bamako, a female predominance was noted with a sex ratio F/H=1.18[14].
This female predominance is linked to anatomical factors.
IV-1-3) Hospitalization structure:
In our study 94 patients from urology and 47 patients from the internal medicine department and 46 patients from the nephrology department.
In the study carried out at the bacteriology-virology department of the National Institute of Public Health (INSP) in Bamako on a sample of 602 cases, 37 patients from the urology department and 3 internal medicine patients and 4 patients from the nephrology[14].
At the CHNU de Fann in Dakar in 2015, which objectified a predominance of the neurology department, i.e. 42%, followed by the infectious and tropical diseases department with 35.68% of cases[19].
This could be explained by the long hospital stay and the use of invasive devices (urinary catheter, etc.), urological procedures and contributing factors such as prostate hypertrophy.
Breakdown by type of sample and place of origin:
The distribution of the species isolated according to the sampling sites reveals that ECBU are the most encountered, followed by suppuration from blood cultures and vaginal samples with rates of 97.33%, 2% and 0.33% and 0.33% respectively.
E. coli is by far the most frequently isolated germ, followed by Klebsiella pneumoniae. This is related to the pathophysiology of urinary tract infection which is generally ascending, and there is strong colonization of the perineum by enterobacteria of digestive origin, and in particular Escherichia coli. Added to this are specific uropathogenicity factors.
Thus, Escherichia coli has andesins, capable of binding the bacterium to the urinary epithelium and preventing its elimination through bladder emptying. Klebsiella secrete a urease which alkalizes the urine, whose naturally acidic pH prevents the proliferation of germs [20].
IV-2) Bacteriological data:
IV-2-1) Frequency of isolated species:
In our seriesEscherichia coliremains the most frequent species with an isolation rate of 66%, followed by Klebsiella pneumoniae 27.7%. This predominance is reported in several studies, but with frequencies varying between 46% and 60% for Escherichia coli, and between 9 and 28% for Klebsiella pneumoniae [2,21]. Enterobacter cloacae and Proteus mirabilis are less common with isolation rates of 2.3% and 1.7%. The same classification was reported by Nijssen et al but with lower rates of 2.2% and 2.9% respectively [22], while higher frequency rates were reported by Cherkaoui in 2014, 9% and 6% respectively [23]. The same observation is reported by Lagha in Algeria, but with rates of 4% and 9% respectively [2].
In the study carried out at the bacteriology-virology department of the National Institute of Public Health (INSP) in Bamako, Escherichia coli was the most isolated enterobacteriaceae (66.6%), probably because of its ability to adhere to cells, followed by Klebsiella pneumoniae (17.0%) [14], which is consistent witha studyrealizedat theHospitalof Mali in 2019[17]. In addition, SABOR in 2017 in DAKAR also found a predominance of these two species of enterobacteriaceae with a rate for Escherichia coli of 40.2% and 27.54% for Klebsiella pneumoniae [15].
Also, these species are distributed differently according to the sampling sites Escherichia coliis considered to be the leader of enterobacterial infections.
Escherichia coliis the most isolated bacterial species in women with 157 against 43 for men among the 200 species of Escherichia coli isolated in our study and affects subjects whose age is over 60 years. This female predominance is explainedpreviously on the basis of the fact that the risk of infections is 50 times more frequent in women, due to the proximity of the urinary meatus and the anus (short perineum) and the shortness of the urethra which is also wide and opens during sexual intercourse [6].
IV-2-2) Resistance to antibiotics:
During this study, we counted 10 different genera belonging to different families of the order Enterobacteraleswere tested against 29 molecules of antibiotics including 15b-lactams, 4 aminoglycosides, 5 quinolones, colistin, fosfomycin, chloraphenicol, Nitrofurantoin, and cothrimoxazole.
Enterobacteriaceae are classified into seven groups based on their natural resistance tob- lactams: Group 0 (Salmonella; Proteus mirabilis), Group1 (Escherichia coli; Shigellaspp), Group2 (Klebsiellaspp; Citrobacter diversus), Group 3 (Enterobacter spp; Serratia spp; Providencia spp; Citrobacter frendii; Hafnia alveii; Morganella), Group 4 (Yersinia), Group 5 (Proteus penneri; Proteus vulgaris), Group 6 (Kluyvera) [24].
Analysis of the resistance profile of Escherichia coli strains in our study shows an increase in resistance rates tob- lactams except carbapenems. Carbapenems and in particular imipenem are molecules of paramount importance which have sometimes become the only effective agents for the treatment of serious infections caused by enterobacteriaceae secreting ab- extended-spectrum lactams (ESBLE), the sensitivity of the latter to imipenem remains high according to several authors[25].
Low resistance rates were obtained for tobramycin 5%, gentamicin 16%, amikacin 4.7%, netilmicin 3.7%. Quinolone resistance has become a concern with a rate of 34.3% for nalidixic acid, 31.8% for ofloxacin, and 19.4% for ciprofloxacin.
While a high resistance rate was obtained for cotrimoxazole 68.42%.
In a study carried out in Bamako over 3 years, more than 72.6% of group I enterobacteriaceaeisolated showed resistance to the combination amoxicillin + clavulanic acid [14]. Our results are similar to those of KALAMBRY, 2019 in Mali, which found 71.0%[17].But they are lower than those of Kara Terki et al. In Algeria, which found 94.0% [26].
The multicenter study by Bouza et al.[27] reports a resistance rate of Escherichia coli of 55% vis-à-vis ampicillin.
A study carried out in the middleurology at the Henri-Mondor hospital, although old(unpublished data),shows that the rates ofresistance evolved from 1998 to 2005, going from 65 to 80% for amoxicillin, five to approximately 15% for cefotaxime, 20 to approximately 35% for ciprofloxacin, ten to more than 20% for gentamicin.
A study in Morocco by Lahlou A et al shows a very clear statistical relationship between the sensitivity to antibiotics that can be used orally for the treatment of cystitis and the history of antibiotic therapy is observed, especially when taking into account the type of antibiotic received: relationship between taking beta-lactams and resistance to amoxicillin - clavulanic acid, the difference in sensitivity being more than 20
Antibiotic resistance is one of the most serious threats to global health today. It is the cause of prolonged hospitalizations and leads to increased medical expenses and mortality. A better knowledge of the local bacterial ecology makes it possible to establish behaviors based on objective data
After the publication of its first report, in April 2014 on bacterial resistance, the WHO is alarmed by a “serious threat to public health” pointing to the ineffectiveness of antibiotics against certain bacteria.
This study, which falls within the framework of a survey on the state of bacterial resistance to antibiotics, has made it possible to highlight certain epidemiological characteristics.
During the study period, 300 strains of enterobacteriaceae were identified in the medical bacteriology laboratory of the CHN.
The rate of resistance to the usual antibiotics is high, this emergence of resistance would be linked to the importance of the prescription of an antibiotic
It is therefore important then
To implement a global management of the use of antibiotics with the aim of reducing and rationalizing their consumption, very early detection of infections with multidrug-resistant germs
Manage the risk factors for enterobacteriaceae infections.
Standard measures include hand washing with a hydroalcoholic solution, wearing gloves in the event of contact with biological fluid and wearing an overcoat in the event of contaminating care, regardless of the patient.
Our study is a prospective study which is related to all samples
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
