
Review Article | DOI: https://doi.org/10.31579/2690-1919/548
1 Department of Pharmacy, Vignan Pharmacy College, Vadlamudi, Guntur, Andhra Pradesh, India.
2 Department of Regulatory affairs, Shri Vishnu College of Pharmacy, Bhimavaram, West Godavari (Dt), Andhra Pradesh, India.
*Corresponding Author: N.L Prasanthim, Pharm, PhD Professor, HOD, Department of Regulatory affairs, Shri Vishnu College of Pharmacy, Bhimavaram, West Godavari (Dt), Andhra Pradesh, India.
Citation: Sarvan M. Seethamraju, K. Venkateswara Raju, G. Dhamasri, Lakshmi P. Nori, (2025), Current Scenario and Regulatory Issues of Mammography- A Magic Tool for Women’s Health, J Clinical Research and Reports, 20(3); DOI:10.31579/2690-1919/548
Copyright: © 2025, N.L Prasanthim. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 June 2025 | Accepted: 02 July 2025 | Published: 09 July 2025
Keywords: breast cancer; mammograms; mortality; 3d image; tomosynthesis
The most frequent kind of cancer in women over 40 is breast cancer. According to studies, the likelihood of surviving breast cancer is considerably increased by early identification and adequate treatment. Additionally, they have demonstrated how early diagnosis of tiny lesions improves prognosis and significantly lowers mortality. In this situation, mammography is the most effective diagnostic method for screening. However, due to minute variations in the densities of various tissues in the breasts with thick tissues, mammography interpretation is challenging. This study examines the automated mammogram image analysis for breast cancer early detection. If it is identified early, this research might provide radiologists with a greater understanding of preconceptions and offer a better prediction, leading to a considerable drop in mortality of women with breast cancer.
Mammogram is the most effective technique for women to detect breast cancer early, when it is less difficult to treat and before it has grown large enough to feel or produce symptoms. “Regular mammograms can reduce the likelihood of dying from breast cancer. For the majority of women who are screening age, a mammography is now the best method of detecting breast cancer [1]. An X-ray of the breast is used in mammography to detect cancerous alterations. It is utilized as a screening test for asymptomatic women as well as a diagnostic tool to check sick women. The purpose of screening mammography is to find breast cancer early, before a breast lump is felt, while assuring consistently excellent mammography results and exposing the women to radiation as little as possible. The success of mammography screening depends on having a population-based screening programme that achieves high screening coverage of women in the at-risk age group, as well as on the quality performance of the technology.” Women who are detected with abnormal results are then diagnosed and treated. “In 2014, the most recent year for which data is available, the Centers for Disease Control and Prevention (CDC) reports that over 235,000 women had breast cancer diagnoses, and more than 41,000 of them passed away from the condition. In 2017, it was predicted by the National Cancer Institute of the National Institutes of Health that over 250,000 women will be diagnosed with breast cancer and over 40,000 of them would pass away from the condition. As the second biggest cause of cancer deaths among women after lung cancer, breast cancer is now the most prevalent non-skin cancer.” The best way to avoid deaths that may occur if the diagnosis is postponed until the start of more severe symptoms is early diagnosis of breast cancer, which commonly involves breast physical examination and mammography. X-rays are used in mammography, a form of medical imaging, to create images (mammograms) of the internal breast tissues. Screen-film mammography, full-field digital mammography, and digital breast tomosynthesis are all terminology that are used interchangeably in this text. By directing x-rays through the breast, screen-film mammography exposes an x-ray film sheet that is stored in a cassette. The x-rays travel via an image receptor, an electronic component or plate that is radiation-sensitive, during full field digital mammography. Images can be digitally enlarged and shown on a computer workstation, for instance. A computer workstation and an electronic image receptor are used in digital breast tomosynthesis to gather several images of the breast taken from various perspectives. Then a sequence of parallel pictures that resemble breast slices are created on a computer. Mammography can detect breast cancer in its earliest, by detecting with any other method. The interpreter could overlook a malignant lesion if the image quality is subpar. An unnecessary death or increased morbidity could occur as a result of such a false negative diagnosis that delays treatment. It is also true that when normal tissue is mistakenly identified as abnormal due to subpar photos or incorrect interpretations, a false positive diagnosis may result. This could result in unneeded stress for the patient, expensive extra testing, and unnecessary biopsies2.The Comparison of mammography and tomosynthesis is given in the Figure 1.

Figure 1: Comparison of mammography and tomosynthesis
History of Mammography
Normal X-ray equipment was used to create the first mammogram in 1913 by Berlin surgeon Albert Salomon on an axilla and breast that had been surgically removed. Dr. Salomon sought to demonstrate how the breast cancer had migrated to the axillary lymph nodes. “Dr. Salomon's study was unfortunately cut short by political upheaval in Germany, and it wasn't until 1927 that another German surgeon, Otto Kleinschmidt, revealed a technique for imaging the breast that he ascribed to his mentor, the cosmetic surgeon Dr. Erwyn Payr. In 1931, Walter Vogel and Paul Seabold made the first discoveries on how to distinguish benign from malignant tumors on a mammogram. Shortly after, in 1938, radiologists Jacob Gershon-Cohen and Albert Strickland wrote a paper documenting the radiographic changes in a woman's breast throughout the course of her menstrual cycle and life. In an effort to convince his colleagues of the importance of mammography, Dr. Gershon-Cohen often contrasted pathological samples with mammographic pictures throughout his career. By using two films to capture data from both the thinner peripheral breast and the denser posterior breast tissue, Dr. Gerson-Cohen emphasized the importance of image contrast and compression3. Despite his efforts, mammography was not widely used until the 1950s. In 1949, Raul Leborgne of Uruguay reported using mammography to discover micro calcifications in 30% of breast cancers.” As a result, interest in mammograms was revived. Leborgne, who created the modern mammogram, stressed the importance of adequate compression and spot/magnification to more clearly show minute structures. He laid the foundation for our current methods with his huge cone-shaped compression devices, meticulous placement instructions, and calibration for exposure times. But Robert Egan was the one who brought all the technologies together. In the early 1960s, he effectively standardized screening mammography by using high mill ampere, low-kilovolt x-rays on grid-covered industrial film. The first national mammography study, which encompassed 24 institutions, was presented at a symposium on mammography by the US Department of Public Health's Cancer Control Programme in May 1963 at M.D. Anderson Hospital. The results shown in the Egan’s method screening trail gave 21 Percent sign false-negative rate and a 79 Percent sign true-positive rate. This was a turning point in how American women were seen. Mammography screening had a challenging beginning. Leborgne's initial poses, in which the lady was lying on her side, have been replaced with Egan's posture, in which the woman is standing [4].
Outlook of breast cancer
Breast cancer is a disorder when the cells in the breast proliferate uncontrollably. There are various types of breast cancer, each of which is caused by breast cells turning cancerous. Breast cancer may develop in a variety of breast tissues. Figure 2 shows the three essential parts of a breast.
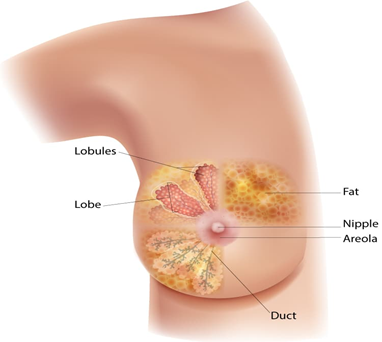
Figure 2: Diagram of the breast
The glands that generate milk are called lobules. The milk ducts that lead to the nipple are known as. The connective tissue, made up of fatty and fibrous tissue, surrounds and holds everything in place. The lobules or ducts are where most breast cancers begin. Breast cancer treatment can be quite effective, especially if the illness is caught early. Breast cancer is commonly treated with a combination of surgical surgery, radiation therapy, and medication (hormonal therapy, chemotherapy, and/or targeted biological therapy) in order to cure the microscopic cancer that has spread from the breast tumor through the blood.Such therapy can halt the development and spread of cancer, therefore saving lives [5].
Overview of the problem
In 2020, 2.3 million women worldwide lost their lives to breast cancer, which claimed around 6,85,000 lives. Breast cancer, which had been discovered in 7.8 million women over the preceding five years, was the most prevalent disease in the world as of the year 2020. Breast cancer is the form of cancer that results in the most lost disability-adjusted life years (DALYs) for women globally. Although the incidence rates increase as people become older, breast cancer affects women after puberty in every place on earth. The death rate for breast cancer did not vary from the 1930s to the 1970s. Improvements in survival began in the 1980s in countries with early detection programmes and various sorts of therapy to get rid of invasive illness. Some indicators of breast cancer include a newly discovered lump in the breast or armpit, Swelling or thickening of a portion of the breast, Dimpling or irritation of the breast skin, Redness or dry skin around the breast or nipple, Nipple pulling in or soreness in the nipple region, Nipple discharge, such as blood, that is not breast milk, Any modification to the breast's size or form and pain in any breast region. Breast cancer can be found and diagnosed using a variety of tests. Such as mammograms, breast ultrasound, breast MRI and newer and experimental breast imaging test [6]. Distribution of breast cancer cases and deaths by world area in 2020 is shown in Figure 3.

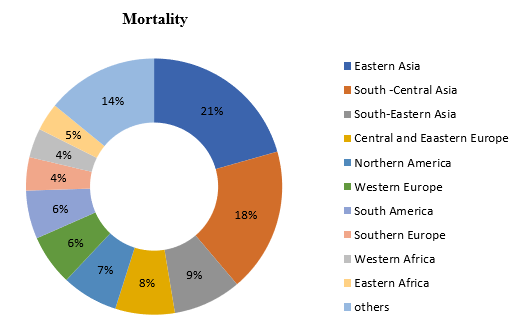
Figure 3: Distribution and death related breast cancer cases world area in 2020
Mammography techniques and technologies
3D mammography -Before being commercialized in the United States, new breast imaging equipment must first get FDA approval, clearance, or permission. Digital breast tomosynthesis sophisticated mammography machines that can generate numerous cross-sectional pictures of the breast from X-rays obtained from various angles have been approved by the FDA. These tools offer useful breast tissue images and could be useful for assessing dense breast tissue [7]. Breast tomosynthesis and digital breast tomosynthesis (DBT) are other names for three-dimensional (3D) mammography. Each breast is crushed from two separate angles (once from top to bottom and once from side to side) similar to a conventional (2D) mammography while x-rays are being collected. However, during a 3D mammography, the machine moves in a tiny arc around the breast while taking numerous low-dose x-rays. The photos are then combined by a computer into a series of thin slices. Doctors can now more clearly and in three dimensions observe the breast tissues thanks to this.
Digital Mammography - Breast cancer screening was initially carried out using screen-film mammography. With the development and launch of affordable large-area digital detectors in the early 2000s, digital mammography was created and made available for clinical usage. In Digital mammography, the usage of film was swapped out with a digital x-ray detector, which produced an image digitally right away, ready for the acquiring radiographer to assess for suitability and the radiologist to interpret. Than screen-film mammography the DM has a number of advantages, with the workflow being one of the most straightforward. The development of more sophisticated image acquisition techniques, such as DBT and dedicated breast CT, as well as the introduction of post-acquisition processing and analysis algorithms make the introduction of digital detectors for breast imaging an additional benefit. By getting two views of each breast - the cranio-caudal (CC) and the medio-lateral oblique (MLO) viewsduring screening mammography, the problem of tissue superposition and performance loss in dense breasts is lessened. The interpreting radiologist compares these two views in an effort to think critically about whether a candidate lesion seen in one view is present in the other or can be discounted as random tissue superposition. They also hope that a different breast compression direction will cause an otherwise occult lesion to be visible in at least one of the views8.
Film-screen mammograms - Black and white images are produced by mammography on film. The film is used by doctors to examine the findings and determine whether there are any problems. This is a slower procedure that used to happen more frequently a few years ago. By using this tumor that are not measurable can be found using x-ray scans and useful to find out minute problems9.
Analog mammography - In analogue mammography, breast tissue changes are identified using low radiation doses that produce X-rays. Film cassettes use the radiation from an X-ray as a source to create a film that shows the breast from several perspectives. The film can be examined by the doctor or translated using computed radiography into a digital image10.
Mammography screening effectiveness
Mammography screening of women between the ages of 50 and 74 can lower the risk of breast cancer death by 20–25%. Because mammography screening schemes had not been in existence for long enough at the time, there was a lack of information allowing an evaluation of the effectiveness; therefore, the Handbook's conclusions were primarily based on the findings of breast-screening trials [11].
Detection of cancer by screening mammography
Breast cancers that are detected in women who participate in screening comprise asymptomatic malignancies discovered during screening and interval cancers. Asymptomatic ductal carcinoma in situ (DCIS) frequently has calcium deposits, which can be easily detected with x-ray-based approaches. The sensitivity of mammography is significant [12].
Are Mammograms safe?
Breasts undergo minimal radiation exposure during mammograms. However, the advantages of mammography outweigh any possible radiation exposure risks. Breast x-rays taken with modern equipment have an excellent image quality despite using modest radiation doses. For a conventional mammography with two views of each breast, the overall dose is typically around 0.4 millisieverts (mSv represents a unit of radiation exposure). The radiation exposure from 3D mammograms can be marginally lower or marginally higher than that from traditional 2D mammography. In the US, people are typically exposed to around 3 mSv of radiation annually merely from their surroundings, which helps put these amounts into context. Background radiation is the term for this. A screening mammography for both breasts uses around the same amount of radiation that a woman would naturally absorb over the course of seven weeks. Inform the x-ray technician and your healthcare practitioner if there's even a remote possibility that you might be pregnant. Mammograms are not regularly performed in pregnant women who are not at greater risk for breast cancer, despite the fact that the danger to the fetus is very low and that they are widely regarded as safe during pregnancy. The advantages of mammography are, at 11 years of follow-up, data from mammography screening programmes point to a 20% reduction in breast cancer mortality, as with other screening tests, mammography screening might produce erroneous positive results; according to estimates, this represents about 20%. Over diagnosis is a risk associated with mammography screening. The quantitative estimates of overdiagnosis in the various age groups are currently characterized by a high degree of uncertainty [13].
Types of mammograms
Screening mammograms: Women who have no symptoms or issues with their breasts get a screening mammography to look for indicators of breast cancer. Each breast is imaged using an X-ray machine from two distinct angles, generally.
Diagnostic mammograms: Mammograms are used to examine a woman's breast when she exhibits breast symptoms or when an atypical finding is made during a screening mammography. They are known as diagnostic mammograms when utilized in this fashion. They could contain extra breast views (images) that aren't included in screening mammography. Women who have already undergone treatment for breast cancer may occasionally be screened using diagnostic mammography [14].
Working of mammogram
The patient's breast is placed on a flat support plate and squeezed with a parallel plate called a paddle during a mammogram. “A brief burst of x-rays is produced by an x-ray machine and passes through the breast to a detector on the opposite side. A photographic film plate, which captures the x-ray image on film, or a solid-state detector, which transmits electronic signals to a computer to generate a digital image, can be used as the detector. Mammograms are the images that are created Low-density tissues, such as fat, look translucent on a film mammography (i.e., darker shades of grey approaching the black background), whereas dense tissues, such as connective and glandular tissue or tumors, appear whiter on a grey backdrop.” A normal mammogram includes a top and side view of each breast, with additional views performed if the physician is worried about a suspicious area of the breast. The working of the Mammography Detection is given in the Figure 4 [15].
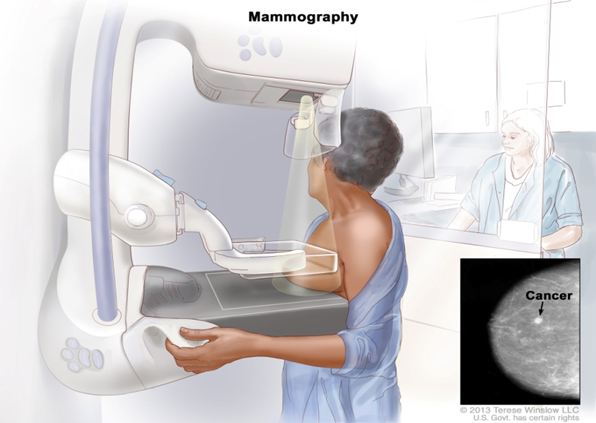
Figure 4: Mammography Detection
Need of compression on the breast
Compression maintains the breast in position to reduce patient movement-related x-ray image blurring. Additionally, compression evens up the breast's contour so that the x-rays have a less way to take in order to reach the detector. This lessens the emission exposure and enhances the image of the x-ray. At the end, compression makes it possible to see all the tissues in one plane, which reduces the likelihood that tiny anomalies may be covered up by breast tissue [16]. Women of age of 40’s advised to go for screening mammogram for every one to two years. Mammograms for screening should be performed on women in their 50s every year. Two breast images are routinely taken during screening mammography from the above (cranial-caudal view, CC) and from an oblique (mediolateral-oblique, MLO). A diagnostic mammogram may be done to investigate an anomaly found during a physical examination or screening mammogram. Taking additional views that are customized to the particular issue during diagnostic mammography may be necessary i.e., each side which includes latero medial, and mediolateral view, cranial-caudial and other views (spot compression, magnification views). If an anomaly is found during mammography diagnostic, further breast imaging, such as ultrasound or biopsy to be used as a kind of follow-up.
Mediolateral oblique view (MLO)
A viewpoint that is angled or oblique is used to capture the mediolateral oblique view (MLO). “The MLO view is preferred during routine screening mammography over a lateral 90-degree projection because more breast tissue may be visible in the upper outer quadrant of the breast and the axilla (armpit). Before capturing an MLO view in step 1, the mammography technologist will set the angle for the appropriate projection (30 degrees to 60 degrees) [17]. An object table is the pedestal that supports the breast and contains the film cassette or digital detector. The top edge of the object table should be parallel to the pectoral (chest) muscles and level with the axillary (armpit) fold. In step 2, patient should remain still and maintain a 45-degree angle with the mammography stand during an MLO view. The technician will urge the patient to elevate her elbow while keeping a firm grip on the machine's handle. The technician will pull the medial (middle) portion of the breast forward while the patient leans slightly forward and the technician will hold the elevated arm and breast from below. The technician will hold the patient's collarbone (clavicle) such that the compression plate just clears the bone once compression has been applied. The technician will check to make sure nothing is obstructing the desired image's field of view after the compression is adequate”. In step 3, technologist will ask the patient to stand very still after positioning her before departing to make the exposure [18]. The images of MLO given in Figure 5.
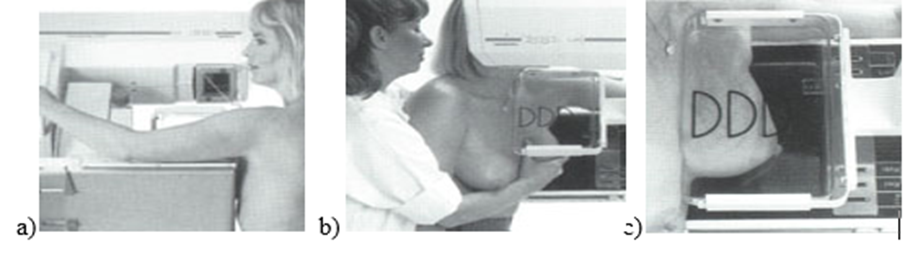
Figure 5: a) MLO view b) During MLO View Figure process c) Final position
Mammography analysis techniques
It demonstrates the many methods of mammography analysis that try to find anomalies as well as the numerous tools created for that purpose. The stages for mammogram analysis are given in Figure 6.
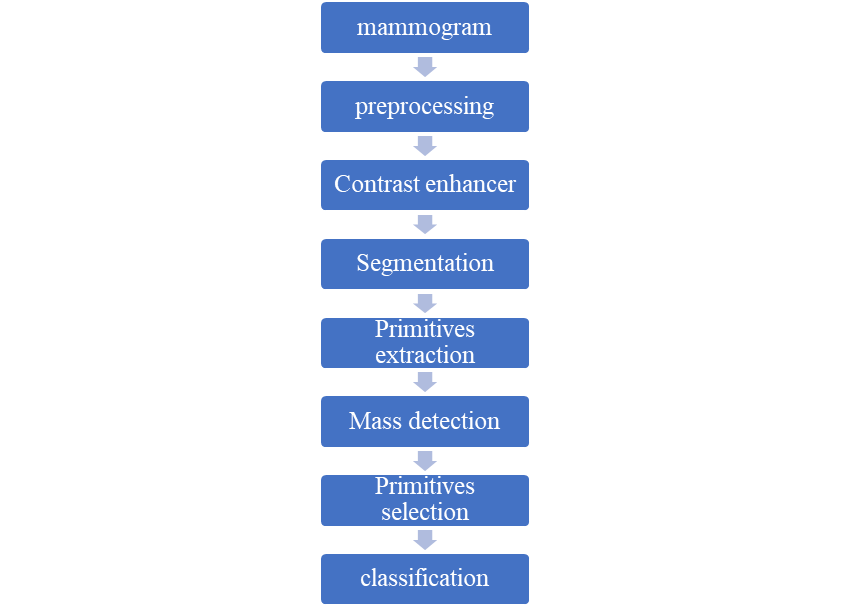
Figure 6: Steps in mammograms analysis
There are four crucial and complimentary approaches that can be used to summarize these processes [19].
Abnormalities shown in the mammograms
Frequently, unusual breast tissue can be seen on mammograms. They can aid medical professionals in determining whether additional testing (such a breast biopsy) is necessary, but they cannot definitively determine whether an atypical spot is cancer. Using a mammography, the following primary breast alterations can be identified: Calcifications, Masses and Distortions [20].
Types of results getting from a screening mammogram
The Breast Imaging Reporting and Data approach (BI-RADS), a standard approach for medical reporting, is used by radiologists and other healthcare professionals to explain screening and diagnostic mammography findings. The outcomes are categorized by this system into groups with numbers 0 through 6. The categories of BI-RADS is given in the Table 121.
| BI-RADS Category | Definition | Explanation |
| 0 | Incomplete. | The radiologist should compare your most recent mammogram with older ones to see if there have been changes in the area over time. |
| 1 | Negative. | No abnormal areas or findings. |
| 2 | Benign (noncancerous) finding. | Found a benign (noncancerous) structure in your breast, such as benign calcifications, lymph nodes, cysts |
| 3 | Probably benign finding. | The findings in this category have a greater than 98% chance of being benign (noncancerous). But since it’s not proven to be benign. |
| 4 | Suspicious abnormality. | This result means the finding(s) could be cancer but are not guaranteed to be cancer. The radiologist recommends a breast biopsy to get more information. |
| 5 | Highly suggestive of malignancy. | This result means the findings look like cancer and have at least a 95% chance of being cancer. |
| 6 | Known biopsy-proven malignancy. | Radiologists only use this result for findings on a mammogram that have previously been diagnosed to be cancer by a biopsy. |
Table 1: Categories of BI-RADS
Basic tests to improve the quality in mammography as a tool. The performance and quality of mammography instrument are tested by various quality tests. The test and instruments used to assess the quality are listed in Table 2.
| S. No | Test name | Equipment used | Type of measurement |
| 1. | Process development |
| The optical density was measured |
| 2. | AEC System |
|
Solidity exposure |
| 3. | Compression force | Three mammographic scales | Measure the force of compression |
| 4. | Analysis results of rejected films |
- |
5980 mammogram films |
Table 2: Test and equipment used to measure the quality
The following tools were used: a viewing box, a pair of magnifying glasses, a densitometer, a sensitometer, electronic and mammographic scales, PMMA plates, a Europhantom, a screen film contact phantom, and thermometer. To check the mammography unit's quality control, four tests were conducted [22].
Emerged companies in the mammography industry
Canon Medical Systems - Canon Medical, which was established in 1930, provides a broad selection of diagnostic medical imaging solutions, including CT, MR, X-Ray, Ultrasound, and Healthcare Informatics, to clients all over the world. In Tochigi, Japan, the headquarters are located.
Siemens Healthineers - Through its subsidiaries, Siemens Healthineers AG creates, produces, and distributes a variety of diagnostic and therapeutic goods and services to healthcare providers all over the world. Germany's Erlangen serves as the organization's headquarters.
Planmed Oy - The business sells mammography and orthopedic imaging products that are renowned for their imaging quality, usability, and superior ergonomics. The corporate headquarters of the corporation are in Helsinki, Finland.
Konica Minolta Inc - Konica Minolta, Inc. operates in the fields of industrial, healthcare, professional print, and digital workplace. The headquarters of Konica Minolta, Inc. are in Tokyo, Japan, where it was established in 1873.
MetaltronicaSpA - Metaltronica, a diagnostic imaging industry leader with a substantial market share in both domestic and foreign markets, was founded in 1977. The corporate offices of the corporation are in Pomezia, Italy.
Global mammography market
The size of the worldwide mammography market was estimated at USD 1.95 billion in 2021, and it is projected to increase at a CAGR of 10.26% from 2022 to 2030. “One of the main reasons projected to fuel demand for breast cancer diagnostic equipment throughout the forecast period is the rising prevalence of breast cancer and the rising demand among patients for early-stage diagnosis.” The U.S mammographymarket size by product graph below as Figure 7.
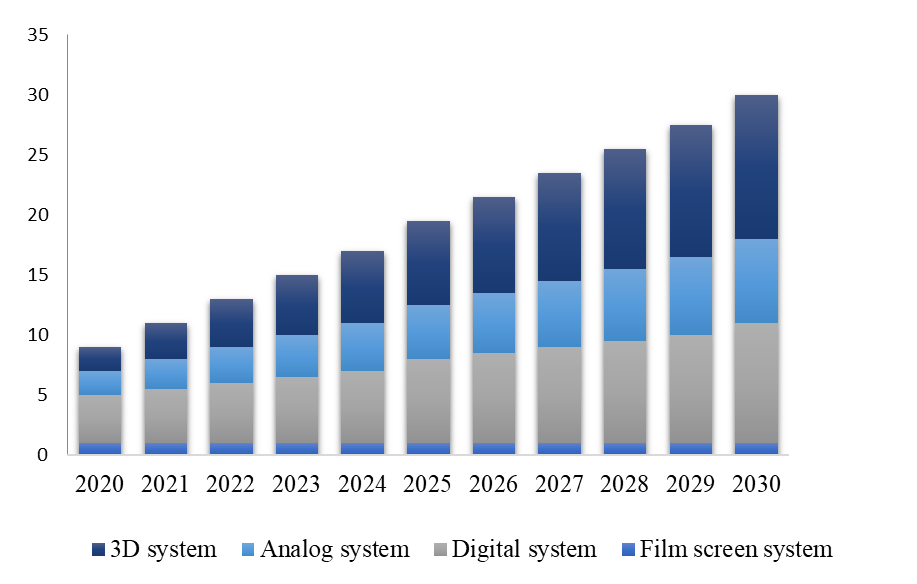
Figure 7: Expected U.S mammography market size
Globally, there was a considerable decline in cancer screening, cancer management visits, and cancer operations as a result of the COVID-19 pandemic. In some locations of the United States, mammograms decreased by up to 92% at the pandemic's height in 2020, according to a report published in the Journal of the American College of Radiology. The FDA reports that 38.8 million women were screened for breast cancer in 2021, which suggests that hundreds of thousands of women in the United States may have postponed or missed their exams as a result of the pandemic.
Regional insights:
With a revenue share of over 36.4% in 2021, North America led the world market and is predicted to rise at a significant rate throughout the forecast period. “One of the main variables influencing the local market is the increasing prevalence of breast cancer. The American Cancer Society estimates that in 2020, there will be around 276,480 new cases of invasive breast cancer in women. In addition, it has been determined that 48,530 women have in situ breast cancer, and it is anticipated that this figure will increase in the upcoming years.” The American organization that provides free mammograms and breast cancer education to needy women in the National Breast Cancer Foundation (NBCF). It is projected that the presence of developing nations like China, Japan, and India will accelerate the region's growth. The regional growth of mammography is given the below. The main leaders of U.S Mammography are “Fujifilm Holdings Corporation, GE Health care, Hologic Inc, Koninklijke Philips NV and Siemens A”.
Indian Mammography market
At a CAGR of 10.53% over the forecast period (2023-2028), the India Mammography Market is anticipated to increase from USD 60.93 million in 2023 to USD 100.52 million by 2028.The Aster RV Breast Clinic, which uses 2Dadvanced, mixed with mammograms 3D, breast ultrasounds, biopsies, and breast MRI to accurately detect and treat all breast-related disorders, opened in India in November 2020. This will probably accelerate the growth of the market. In the long run, this can increase the demand from these facilities for mammography equipment. The mark share of the Indian mammography is given in the Figure 8.

Figure 8: Expected market share of the Indian mammography
The main mammography leaders of Indian market are “Siemens AG, Planmed OY, Hologic Inc, Fujifilm Holdings Corporation and GE Health care”.
Mammography Quality Standards Act (MQSA)
The Mammography Quality Standards Act, which was passed by Congress in 1992 and went into force in 1994, is known by the acronym MQSA. With the help of this law, mammography facilities and doctors who perform mammograms on patients will be held to a set of quality standards. Due to the MQSA, all mammography facilities in the US were compelled to follow a set of minimal standards in order to maintain their MQSA certification and their rights to go on offering mammography services. It consists of approval must be done by the FDA For accreditation organization, should meet the FDA or State Approval standards, mandatory to qualify the annual MQSA inspection, the MQSA certificates approval should be displayed prominently, it should conduct an annual Medical Physicist survey on all mammography equipment and it must maintain ACR accreditation by an FDA approved accrediting body
MQSA requirements for mammography
To perform a mammography on a patient, one needs extensive training. It requires more now than it did in the 1990s, at least. At this time, Congress started to pay attention to the caliber and expertise of mammography. Before the passage of this landmark legislation, many facilities in the US
produced and interpreted subpar images using out-of-date technology and untrained radiologists and technologists with inadequate training. This meant that the photos that were taken weren't as useful as they may have been in identifying breast cancer. There were also issues with how patients were informed of their results. There were also few programmes in place that gave patients the chance to voice their objections. But with the passage of the Mammography Quality Standards Act in 1992, everything changed. Since then, significant improvements have been made to the entire set of MQSA criteria [23].
Mammography screening guidelines recommended by the six us medical organizations
On June 22, 2017, the American Congress of Obstetricians and Gynecologists (ACOG) published updated breast cancer screening recommendations for women with an average risk of developing the disease. The new regulations were given by the ACOG. The new guidelines recommend women for the screening mammography over the age of 40 every one to two years, with the first screening mammogram occurring no later than age 50. The decision to continue screening mammography in women over the age of 75 should be made by each woman in consultation with her healthcare provider and should take into account the woman's health status and expected lifespan. There are little changes from the numerous medical organizations regarding the mammography screening guidelines [24]. The recommendations of six US medical organizations are summarized in Table 325.
| Organization | Starting age (years) | Stopping age | Mammography interval |
| AAFP | 50 recommended, individual decision from 40-49 | 74 years | Every 2 years |
| ACR/SBI | 40 | No specified age, tailored to health status of patient | Annually |
| ACS | 45 recommended; option to start at 40 | Continue to life expectancy <10> | Annually between 45-54; every 1 or 2 years at 55+ |
| ACOG | Offer at 40, not later than 50 | Age 75, then shared decision making | Every 1 or 2 years |
| NCCN | 40 | Upper age limit for screening, not established, consider severe comorbidities limiting life expectancy | Annually |
| USPSTF | 50 | 74 years | Every 2 years |
Regulations of Mammography Quality Standards Act (MQSA)
The quality standards of the Mammography Quality Standards Act’s, which were designed, go into force as of the following act i.e., 21CFR900- Mammography standards act [26]. This act having number of subparts, part-A deals with accreditation process, subpart B deals with quality standards and certification and Subpart C deals with states as certifiers. The Mammography Quality Standards Act (MQSA), codified at 42 U.S.C. 263b, is carried out via the rules outlined in this part. The processes for applying to become approved accreditation organization, which certifies the provisions as being qualified to provide screening or diagnostic mammography services, are outlined in Subpart A of this part. The procedures and standards for accreditation organizations are further established in Subpart A to guarantee that all mammography provisions subject to US jurisdiction are suitably assessed for compliance with quality standards. To promote safe, dependable, and accurate mammography, this part's subpart B defines minimum national quality requirements for mammography facilities. Facilities owned or operated by the Department of Veterans Affairs are exempt from the restrictions in this chapter [27]. “In Subpart C of this part, the procedures for applying to a State to become a certification agency designated by the FDA to certify businesses within the State to offer mammography services are laid forth. Subpart C of this part further establishes requirements and standards for State certification agencies to ensure that all mammography facilities under their jurisdiction are properly and consistently evaluated for compliance with quality standards at least as stringent as the national quality standards established by FDA”.
The MQSA program's most frequently requested national statistics are provided in this area of MQSA Insights. Every month on the first, these stats are updated. Table 4 provided national statistics relating to the MQSA programme. The number represents the average of all yearly procedures that facilities reported to their accrediting bodies at the time of their re-accreditation, which takes place every three years. Only information supplied by non-veterans’ hospital administration hospitals that were MQSA-certified was pooled. The sum could not possibly reflect the volume of procedures now performed at these institutions. It contains computed radiography and full field digital mammography units. It also facilities with FFDM also have DBT; hence the number of DBT facilities is included in the total number of digital facilities.
| Certified facilities, as of October 1,2022 | 8,790 |
Certification statistics, as of May 1, 2023 Total certified facilities/Total accredited units Certified facilities with 2D digital units / Accredited 2D digital units Certified facilities with DBT digital units / Accredited DBT digital units | 8,829/24,904 8,825/ 13,370 7,628/11,531 |
Percent of inspection where the highest noncompliance was a: Level 1 violation Level 2 violation Percent of inspections with no violation |
1% 10.9% 88.1% |
| Total annual mammography procedure reported, as of May 1, 2023 | 39,732,862 |
Table 4: National statistics regarding the MQSA program
Case study on mammography
Mammography Problems at Capitol Radiology, Laurel, Maryland: FDA Safety Communication issued on June 30, 2022. Concerns about the caliber of mammograms conducted at Capitol Radiology, LLC were brought to the FDA's attention [28].A Full Field Digital Mammography (FFDM) unit was not accredited by the provisions accrediting organization, the American College of Radiology, the provision dialed too conduct quality control test of an imaging unit for 12 .Due to the provision’s failure to operate in accordance with the MQSA, the FDA advised the provision that it needed to conduct an Additional Mammography Review (AMR) to check whether the general caliber of mammography performed at the facility had been harmed and whether it was necessary to notify patients who might have been affected [29].
Warning letter
The warning letter was issued for the company East Jefferson General hospital in 13/11/19.This letter is on behalf of FDA; they have inspected your facility and your facility did not meet the conditions of Mammography Quality Standard Act to practicing mammography and conditions present in the section 263b of Tittle 42 of USC. The issues involved are, the x-ray unit 98, 12 room of mammography 3 is not accredited as per 21 CFR Part 900.4(a), (b) &(c) (4).
Mammography is a valuable and crucial diagnostic tool used in the detection of breast cancer by two types of views i.e., cranial - caudal view and mediolateral-oblique view. Screening of breast cancer allows identifying the abnormalities such as tumor or calcifications that may indicate the presence of cancer. Advancement technologies present in the mammography such as 3D mammography (tomosynthesis), digital mammography etc. This article also provides the analysis steps for the mammography detection. There are certain quality tests for the improvement of the mammogram quality. Based on the existing research evidence mammography has been shown to reduce the breast cancer mortality rates by detecting tumors at the early stage. The growth of the mammography market in the U.S and India has been increasing vastly. Some of the U.S organizations recommended mammography screening guidelines for breast cancer detection. According to FDA, Mammography quality standards act regulations are mentioned in the CFR TITLE [21] PART 900. According to this CFR, the mammography facilities should be accredited and provide high quality of mammography services to the patients.
No
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
