
Case Report | DOI: https://doi.org/10.31579/2768-2757/032
1MBBS, General surgery resident at Bombay Hospital, India.
2Assistant Professor, Maharashtra University of health sciences, Nashik, Postgraduate Teacher, Bombay hospital Institute of Medical Sciences, General surgery resident at Bombay Hospital, India.
*Corresponding Author: Chatterjee S, Assistant Professor, Maharashtra University of health sciences, Nashik, Postgraduate Teacher, Bombay hospital Institute of Medical Sciences, General surgery resident at Bombay Hospital, India.
Citation: Prathamesh P, Raviraj C, Chatterjee S. (2022). Curious case of Retrosternal Colloid Goitre. Journal of Clinical Surgery and Research. 3(1); DOI:10.31579/2768-2757/032
Copyright: ©2022 Chatterjee S, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 September 2021 | Accepted: 29 November 2021 | Published: 05 January 2022
Keywords: retrosternal goiter; compression symptoms, thyroidectomy
Background: Retrosternal goitre is considered to be a rare entity. It is a slow growing enlargement of the thyroid gland which remains asymptomatic for many years. Symptoms are mainly due to compression of airways and oesophagus. Surgical management with the removal of the involved lobe is considered sufficient.
Summary: Here we report a case of a 33 yrs. old lady who presented to us with complaints of neck pain, facial flushing, difficulty in breathing and vague body ache. Clinical examination was within normal limits. The patient was referred to orthopedician for further evaluation. MRI cervical spine was done which was suggestive of large swelling in left lobe of thyroid with retrosternal extension causing deviation of trachea to opposite side. FNAC was done which was inconclusive. The involved lobe was removed surgically with frozen section suggestive of Colloid goitre.
Conclusion: Retrosternal goitre are slow growing enlargement of thyroid gland which may present with vague symptoms, best managed surgically often followed relief from the symptoms post-surgery.
Goitre is defined as any swelling in the neck resulting from enlargement of thyroid gland. The prevalence of goitre is attributed to multiple factorsand is around 15.8 % worldwide [1]. In India, it is estimated that 54 million people are suffering from goiter [2]. Retrosternal goitre amongstall the goitres is considered to be a rare entity.A metanalysis showed a prevalence of approx. 6.28% of all the cases of goiter [3].Retrosternal goitre is defined as a goitre i.e. enlargement of thyroid gland with >50% located in the mediastinum. The natural history of retrosternal goitre is suggestive of a slow growing enlargement of the gland with patient being asymptomatic for many years. Most of the retrosternal goitres are detected incidentally on radiological examination. The most common symptoms of retrosternal goitre are associated with compression of the airways and esophagus [4, 5]. Excision of the goitre with hemi- thyroidectomy of the involved lobe is considered sufficient for retrosternal goitre. Cervical approach is considered sufficient for the excision of the retrosternal goitre. Very rarely, full sternotomy or manubriotomy or thoracotomy is reportedly requiredfor the excision of the retrosternal goitre. Here we present a case of one such retrosternal goitreand its course of management.
A 33 yrs old female with no known comorbidities came to the OPD with complaints of neck pain, facial flushing, difficulty in breathing in lying down position and vague bodyache since 15 days. No h/o fever, difficulty in swallowing, change of voice, swelling in the neck was identified. There was no past surgical or significant medical history. No history of consumption of any regular medication or drug allergies were identified. Clinicalexamination was completely within normal limits.
The patient was referred to orthopedician for further evaluation. MRI of the cervical spine with screening whole spine was adviced with some blood investigations. MRIwas suggestive of a large swelling in the left lobe of thyroid with retrosternal extension causing deviation of trachea to the opposite side and compression effect over the structures in the neck.
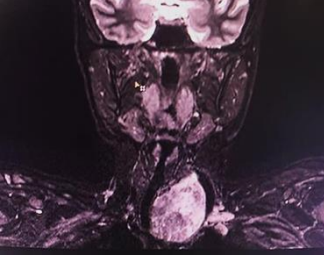
Figure 1: MRI neck showing left thyroid mass with retrosternal extension deviating trachea towards right and causing compressiveeffects over the structures in the neck.
Blood investigations were send to know the thyroid status. The patient was clinically and biochemically euthyroid. FNAC was done which was inconclusive. The patient was then posted for surgery with intraop frozen section. Intraoperatively a horizontal skin crease incision was taken 4-5 cm above the suprasternal notch. Incision was deepened. Subplatymal planes were created and flaps were raised. Midlinewas seen deviatedtowards the right. Strap muscleswere separated accordingly. Left lobe of thyroid enlarged with lower part extending retrosternal. The retrosternal part was delivered out and left hemithyroidectomy was done. The specimen was sent for intraop frozen section.Frozen section was suggestive of colloid goitre. Post-surgery all the symptoms of the patients got relieved.

Treatment of retrosternal goitre has always been challenging. However, surgical excision remains the gold standard treatment of symptomatic retrosternal goitre. Symptoms of retrosternal goitre are mostly due to compression of the airwaysand oesophagus. Symptomsincludeb reathlessness due to chokingsensation, inability to sleep comfortably, difficulty in swallowing and hoarseness of voice. Less commonly, signs of compression of vessels i.e. superior vena cava syndrome and nerves i.e. Horner’s syndrome. There is still a controversy regarding treatment of asymptomatic retrosternal goitres. Traditionally, retrosternal goitre was considered to be th absoluteindication for the surgical management. However, there is controversy regarding treatment of asymptomatic retrosternal goitres. The evidence suggests surgical excisionof retrosternal goitre at an earliest preventing complications. Retrosternal goitre in majority of the cases can be excised via the cervical approach itself with some patient requiring sternotomy. There are no upfront guidelines which helps a surgeonto pre-operatively anticipate requirement of sternotomy for the surgical excision of thyroid gland. It had suggested by some studies that presence of presence of malignancy, involvement of posterior mediastinum, presence of ectopic thyroidand extension beyondthe aortic arch will requiremidline sternotomy extension of the cervical incision [3, 4, 5, 6].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
