
Research Article | DOI: https://doi.org/10.31579/2693-7247/130
Family Physician & Public Health Consultant Bengaluru & Visiting Professor of Practice-MPH, Schools of Environmental Science, Public Health and Sanitation Management, Karnataka State Rural Development and Panchayat Raj University (KSRDPRU), GADAG, Karnataka India.
*Corresponding Author: Suresh Kishanrao, Family Physician & Public Health Consultant Bengaluru & Visiting Professor of Practice-MPH, Schools of Environmental Science, Public Health and Sanitation Management, Karnataka State Rural Development and Panchayat Raj University (KSRDPR
Citation: Suresh Kishanrao, Family Physician & Public Health Consultant Bengaluru & Visiting Professor of Practice-MPH, Schools of Environmental Science, Public Health and Sanitation Management, Karnataka State Rural Development and Panchayat Raj University (KSRDPRU), GADAG, Karnataka India., J. Pharmaceutics and Pharmacology Research, 6(4); DOI:10.31579/2693-7247/130
Copyright: © 2023, Suresh Kishanrao. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 April 2023 | Accepted: 28 April 2023 | Published: 18 May 2023
Keywords: chronic venous disease; lymphedema; vascular medicine
Chronic limbs edema is a progressive, physically disfiguring and currently incurable condition. Multiple etiologies must be considered and often more than one cause may be present especially in chronic bilateral oedema of both lower limbs. In India for want of vascular specialists at district level for evaluation, patients with lower limb edema visit Physicians or Endocrinologist or Cardiologist or even Surgeons if there is an history of injury. The role of lymphatic system regardless of the underlying pathology has been underestimated. A thorough history and physical examination and a carefully considered laboratory and imaging evaluation are critical in differentiating causes. A multifaceted program has been recommended to manage the swelling.
In this article, I report a case that was wrongly diagnosed as Hypothyroid case and following a reaction to the thyroid hormone was referred to a super specialty unit of a public sector Medical College to clinch the correct diagnosis after venous doppler test and treated appropriately to completely cure the condition otherwise thought to be incurable.
Material & Methods: A female of 43 years in known circle presented to Physician in March 2022, in Hubballi a city of author’s medical education. She was diagnosed as Hypothyroid case based on non-pitting bilateral chronic oedema and serum TSH levels. A drug reaction to the thyroid hormone led to second opinion seeking from me on video-consultation. After a detailed history, and video inspection of affected limbs I referred her to a super specialty unit of a public sector Medical College to clinch the correct diagnosis of cellulitis after venous doppler test and treated appropriately. An antibiotic therapy for over 2 weeks resolved the oedema of both the lower limbs. A review of literature and studies of lower limb oedema, epidemiology of Filariasis as the locality is known to be endemic are the resources guided this article.
Chronic limbs oedema is a progressive, physically disfiguring and currently incurable condition. It is a major clinical problem that impacts on an individual’s physical and psychosocial wellbeing [1]. Swelling of the upper or lower extremities may be either unilateral or bilateral: i) Unilateral limbs swelling is more often due to causes like local trauma, venous disease, (e.g., deep vein thrombosis) or cellulitis. Bilateral swelling is usually due to systemic conditions (e.g., cardiac failure, Hypothyroidism), it may be much more obvious on one side than the other and therefore can appear to be unilateral swelling [4].
The most common cause of swelling of the legs is peripheral oedema, due to accumulation of fluid in the interstitial space; however, any tissue of the legs can be swollen. Systemic causes of swollen legs include Congestive cardiac failure, Hypo-proteinemia due to liver failure, nephrotic syndrome, malnutrition, protein-losing enteropathy, Acute kidney injury and chronic kidney disease, Fluid overload, Anemia, Medication like calcium antagonists, non-steroidal anti-inflammatory drugs, and Hypothyroidism [2].
Chronic Oedema has been defined as swelling in the tissue that persists beyond three months, and is considered as a progressive, physically disfiguring, and incurable condition [1]. Chronic edema is significantly associated with a history of cellulitis, that patients with and without wounds suffered at least one event of cellulitis compared to those without CO.
The nature of the presentation will give essential clues in establishing the diagnosis. Therefore, the history should capture the nature of swellings- Acute or chronic, Unilateral, or bilateral, Acute, or chronic onset, Painful or not painful and associated symptoms if any like i) orthopnea, paroxysmal nocturnal dyspnea due to heart failure. ii) Diarrhea or other bowel dysfunction suggesting protein-losing enteropathy iii) Painful swollen calf pointing to deep vein thrombosis or inflammation due to cellulitis, osteomyelitis iv) Pigmentation suggesting venous insufficiency. v) Immobility due to Pelvic mass or pregnancy [2].
Diagnostic challenge may often be clear without the need for any tests. The choice of initial tests will depend on the differential diagnosis based on clinical assessment. Potential initial investigations include: i) Urinalysis: proteinuria suggests renal cause ii) FBC: high white cell count in infection; anemia iii) Biochemistry: renal function and electrolytes (raised creatinine in renal disease) iv) LFTs (impaired liver function and associated low albumin); v) Blood glucose (infection associated with diabetes); vi) Thyroid Function Tests to rule out hypothyroidism). vii) blood Clotting screen: abnormal clotting associated with spontaneous hematoma. viii) Chest X Ray (CXR) for pulmonary oedema. ix) D-dimer blood test -raised in patients with venous thromboembolism, though sensitivity is high, but specificity is poor. x) ECG: heart failure xi) Ultrasound, CT scan: hematoma, tumor, abdominal or pelvic mass. xii) Duplex Doppler Venography for deep vein thrombosis, arteriovenous fistula. xii) Lymphangiography to demonstrates cause of lymphedema like hypoplasia or obstruction and Lymph node biopsy and Renal biopsy for confirming infection or tumor [3].
In this article I report one case of bilateral swelling, misinterpreted as hypothyroidism-based Serum TSH levels showing mild hypothyroidism and later diagnosed as Cellulitis based on Venous doppler test in a tertiary care public sector hospital and treated with antibiotics.
Exactly a year ago (18/03/2022) Purnima, a cook by profession, aged about 43 years, approached with the complaints of swelling of both lower limbs to private Physician in Hubballi, Karnataka. The swelling was insidious, over last 4 months with mild discomfort in the last one month. There was no history of fever or any other signs of infection or inflammation like reddish discoloration, and neither there was much pain nor any tenderness on pressing. Oedema was non-pitting in nature. The swelling was not affected by dependency during the day or improved with elevation. Although the main complaint was in the lower limbs, evaluation of the heart, lungs, and abdomen were done to assess for systemic etiologies or contributing factors and prima facia none were found positive. The patient was a bit heavily built but not identified as obese or had a large abdomen that contribute to bilateral lower limb edema.
Basic investigation of blood indicated a total WBC count of 14,300 as against (a range of 4-11K), and increased TSH of 8.8MicroIU/ml ((as against normal range (0.27-4.2). Based on this suspecting Hypothyroidism the physician puts her on Thyroid hormone (Tab Thyronorm 25 mcg daily) along with Grilcol (a combination of Calcium citrate, Magnesium, Vitamin D3 and Zinc). Within a week’s time, as she was uncomfortable sought my opinion.
Based on the photographs shared (Fif-1-4 see next page) and a video consultation, I assessed both lower limbs, and found that both limbs were swollen though it was more in left lower limb with the compliant as affected limb. Disproportionate swelling was noted from the ankles to the waist when compared with the torso above. A lack of pitting lymphedema, Painless, slightly restricted range of motion, were noted. I suspected some low-grade infection / inflammation (Filarial lymphedema) as the area is endemic for Filarial infections. Keeping her occupation and the cracks & fissures in her sole’s toes and the environment in which she works daily, I suspected chronic inflammation.
Therefore, I referred her to super specialty hospital attached to the Medical College. On 25 March 2023, she consulted an endocrinologist. With clinical a differential diagnosis of i) subclinical hypothyroidism ii) Superficial Chronic venous disease/post-thrombotic syndrome iii) Diffuse Cellulitis iv) Idiopathic edema were considered and advised a venous doppler. The Venous doppler ruled out Thrombophlebitis as CPV, SPV, PV and PTV courses were normal. Narrowing down the diagnosis to Diffuse Cellulitis she was advised MgSo4 crape bandage and antibiotics for 10 days. By 9th April 2022 the swelling had reduced a lot as seen in the fig 5-6. And by 26th April her feet were normal (Fig-7).
Figure-1: 25 March 2022 Rt. Leg Oedema

Figure-2: 25 March 2022 Rt. Leg Oedema

Figure-3: 25 March 2022 Pedal Oedema

Figure-4: 25 March 2022 Cracks in Toes

Figure-5, 9: April 2022 Lt. Leg Reduced Oedema

Figure-6, 9: April 2022, Reduced Pedal Oedema

Figure-7: 26 April 2022 Normal feet.
Lower limb edema is a common and challenging diagnostic problem often with a significant impact. It is defined as swelling caused by an increase in interstitial fluid that exceeds the capacity of physiologic lymphatic drainage. In most cases it occurs when fluid accumulates in subcutaneous tissues leading to volume expansion. Systemic conditions like infra-inguinal superficial and deep venous reflux, supra and infra inguinal deep vein obstruction, and primary and secondary lymphatic diseases. Recent works have demonstrated that chronic edema negatively impacts physical and psychological health and reduces quality of life. Multiple etiologies must be considered and often more than one cause may be present especially in chronic bilateral oedema of both lower limbs. In India for want of vascular specialists at district level for evaluation, patients with lower limb edema visits Physicians or surgeons if there is an history of injury. The role of lymphatic system regardless of the underlying pathology has been underestimated. A thorough history and physical examination and a carefully considered laboratory and imaging evaluation are critical in differentiating causes.
It is essential to take a complete patient history to facilitate accurate, efficient, and cost-effective diagnostic testing and management. The site of swelling and any associated manifestations should be assessed, including whether it is unilateral, bilateral equal or bilateral but asymmetric, along with any changes that occur with its severity with position and time of day. Swelling can be asymptomatic, associated with symptoms as in our case such as aching, pain, heaviness. In our case Physician missed the diagnosis as he did not look for oedema in neck, upper limbs and entire body. Patients may describe a gradual onset or a more long-standing condition as in our case, but a sudden onset of limbs swelling is not rare if it is due to secondary infections.
Chronic swelling may be due to venous insufficiency, lymphatic dysfunction, static foot disorders, or more longstanding medical etiologies. In the reported case Venous edema was ruled out as there was no complaints of aching, or fatigue of the limbs. Lymphedema is usually painless and may present with classic signs of foot involvement. Lipedema was also ruled out as it almost always is bilateral, spares the feet, and presents with disproportionate pain, tenderness, and an unusual tendency to bruise easily.
As a systemic issue was suspected, appropriate laboratory tests were performed by the primary care physician, included Complete blood count, a metabolic panel including evaluation of creatine, urinalysis, thyroid panel, atrial natriuretic peptide, hepatic enzymes, and albumin level only moderately elevated TSH. Despite a clear understanding that normal range for TSH in most Indian laboratories is 0.4 milliunits per liter (mU/L) to 4.0 mU/L and If TSH is higher than 4.0 mU/L on repeat tests, we should suspect hypothyroidism, the physician diagnosed as Hypothyroidism and put her on Thyronorm. As she did not tolerate the hormone, she sought second opinion and was referred to tertiary care hospital where the cardiologist ordered imaging studies -Venous doppler study and confirmed the diagnosis as Chronic Diffuse Cellulitis. Chronic venous disease could have been cause of edema in the lower legs, a condition in which the veins in the legs cannot pump enough blood back up to the heart because the valves in the veins are damaged.
Duplex ultrasound (DUS) is a non-invasive, low-cost test that surveys the extremities for vascular and non-vascular causes of both acute and chronic swelling and offers a reproducible method of viewing venous anatomy, valve function, and patency. It allows the initial and often the only imaging test in patients with swollen lower limbs without a clear cause based on history, physical and laboratory exam, or when further details are required to make therapeutic decisions. This test has sensitivity and specificity rate greater than 90% for DVT, venous reflux, and non-vascular etiologies, swelling can be readily and robustly evaluated.
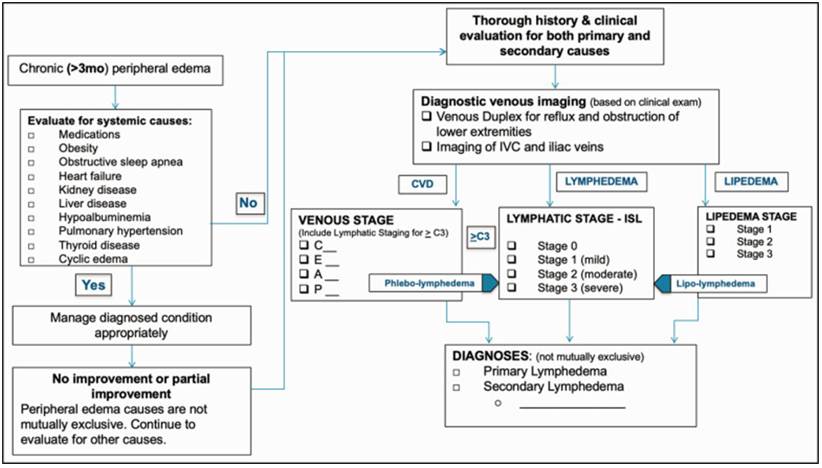
Figure-8: A practical diagnostic Algorithm [2]
There are many potential causes of swollen feet, legs, and ankles. Swelling occurs in most cases because of such lifestyle causes, such as: i) Being overweight, Excess body mass can decrease blood circulation, causing fluid to build up in your feet, legs, and ankles, that was ruled out in our case ii) Standing or sitting for long periods- as our case’s occupation involved log hours of standing for 3-4 hours each in the morning and late evenings and the cracks and fissures in legs and the unhygienic environment she worked prompted to suspect chronic inflammation. Other possible causes like Natural / induced hormonal changes (as she is used to take oral contraceptive for postponing the menstrual cycles) was considered. Fluctuating levels of estrogen, and progesterone can reduce circulation in the legs and lead to swelling. Idiopathic and Pre-menstrual oedema were considered and ruled out as in females of menstruating age idiopathic or cyclical edema is seen throughout the menstruating period and premenstrual edema occurs few days prior to menstruation and our case had the oedema throughout and increased over 4 months.
Cellulitis: Chronic Cellulitis is caused when streptococcus and staphylococcus, enter through a crack or break in the skin. In our case this was the suspected cause to put the lady on antibiotics [6]. Cellulitis a common, potentially serious bacterial skin infection is an infection that occurs in the subcutaneous tissues, caused by multiple bacteria (Staphylococcus, Streptococcus, Klebsiella, Acinetobacter, Pseudomonas aeruginosa, and E. coli.). Fusarium solani and Purpureocillium lilacinum are important pathogens causing opportunistic fungal cellulitis. The affected skin is swollen and inflamed and is typically painful and warm to the touch, but exceptionally it is chronic, insidious as in our case. Cellulitis usually affects the lower legs, but it can occur on the face, arms, and other areas. The infection happens when a break in the skin allows bacteria to enter. Left untreated, the infection can spread to the lymph nodes and bloodstream and rapidly become life-threatening. It isn't usually spread from person to person. The incidence of a more serious staphylococcus infection called methicillin-resistant Staphylococcus aureus (MRSA) is increasing [6]. Trimming fingernails and toenails carefully and not to injure the sole and feet are preventive measures. Lubricating the skin helps prevent cracking and peeling. Protecting hands and feet by wear footwear and gloves suitable to activities are advised but the Indian customs of cooking do not permit such actions. Promptly treating infections on the skin's surface, mild cellulitis as in our case can be treated with oral antibiotics, (penicillin, cephalosporins, dicloxacillin, or clindamycin) and or anti-fungal drugs (Amphotericin B / Ketoconazole) as soon as they occur are the only options. Having had cellulitis once increases the risk of getting it again and the patient is advised to be careful and take possible preventive actions suggested above.
Filarial Elephantiasis: In India, the incidence of microfilarial infection has decreased from 1.24% to 0.26% over a period of 18 years from 2004 to 2021 along with a decrease in the incidence of lymphedema (Elephantiasis). Lymphatic filariasis impairs the lymphatic system and can lead to the abnormal enlargement of body parts, causing pain, severe disability, and social stigma. 863 million people in 47 countries worldwide remain threatened by lymphatic filariasis. More than 8.6 billion cumulative treatments have been delivered to stop the spread of infection since 2000. 51 million people were infected as of 2018, a 74 percentage decline since the start of WHO’s Global Program to Eliminate Lymphatic Filariasis in 2000. An essential, recommended package of care can alleviate suffering and prevent further disability among people living with disease caused by lymphatic filariasis [6].
In India, lymphatic filariasis is reported to be endemic in 250 districts (presently 256) in 16 states and 5 UTs. About 31 million people are estimated to be the carriers of mF and over 23 million suffer from filarial disease manifestations in India. The national program had listed more than 800,000 lymphoedema and 400,000 hydrocele cases The state of Bihar has highest endemicity (over 17%) followed by Kerala (15.7%) and Uttar Pradesh (14.6%). Andhra Pradesh and Tamil Nadu have about 10% endemicity [8]. Karnataka’s focus is on selected pockets of Vijayapura, Bidar, and Kalaburagi. Karnataka is one among the ten high-burden States in the country, with 12,000 chronic cases of LF [9]. 16 cases of elephantiasis among migrant workers in Tumakuru district in 2022. Out of the 16 patients, 13 are from Bihar and one each from Odisha, UP and Vijayapura district [10].
The above data clearly shows that there is changing pattern in the etiology of pedal edema from communicable diseases like HBV, HCV and Filariasis to non-communicable diseases like CHD, Alcoholic Liver Disease, CKD due to Diabetes Mellitus, Systemic Hypertension etc.
Diagnosis and testing: Diagnosis of cellulitis is usually made clinically and routine collection of cultures, including blood, cutaneous aspirates, biopsies, or swabs are not recommended. Waiting for culture results should not delay the initiation of treatment; however, when available, culture results can be used to tailor antibiotic therapy.
Treatment: For typical cases of non-purulent cellulitis, treatment with an antibiotic that is active against both Staphylococcus aureus and group A strep. Group A strep remains susceptible to beta-lactam antibiotics. Mild cellulitis can be treated with oral antibiotics, including penicillin, cephalosporins dicloxacillin, or clindamycin. If signs of systemic infection are present, then intravenous antibiotics can be considered, such as penicillin, ceftriaxone, cefazolin, or clindamycin.[6]. The recommended duration of antibiotic treatment for most cellulitis cases is 5 days but some cases not seeing major improvement during this period may require longer durations of treatment as was in our case.
Prognosis and complications: Occasionally, cellulitis can result in bacteremia and rarely in deep tissue infections, such as septic thrombophlebitis, suppurative arthritis, osteomyelitis, and infective endocarditis. Patients with impaired lymphatic drainage of the limbs are at increased risk of recurrent infection.
As such, in this opinion article, I second the proposal of a practical diagnostic approach to identify the causes of chronic edema accurately and efficiently in affected patients and to institute appropriate antibiotic therapy. This diagnostic algorithm (Fig-8) incorporates a systematic approach to the patient with leg swelling and provides an efficient pathway for the differential diagnosis and management for this problem [2].
In approaching bilateral chronic lower limb edema, a careful history and physical examination, followed by basic investigations and Venous doppler test are essential in the differentiation of causes. The proposed differential diagnostic pathway facilitates a systematic approach to patients presenting with a chronic bilateral leg swelling.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
