
Case Report | DOI: https://doi.org/10.31579/2690-8794/043
1* IC Universal Legal, Advocates & Solicitors, Mumbai, India.
*Corresponding Author: Rd. Twinkle Dhamecha, Principal Associate at IC Universal Legal, Advocates & Solicitors, Mumbai, India.
Citation: Dhamecha T., Bhavita Prajapati Dr. Anant Marathe (2020) Cryptococcus laurentii (Non Cryptococcus neoformans/gatti) infections – Immunocompromised or Immunocompetent -Who is at risk? – Systematic review J. Clinical Medical Reviews and Reports 2(8); DOI: 10.31579/2690-8794/043
Copyright: © 2020, Twinkle Dhamecha, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 September 2020 | Accepted: 10 September 2020 | Published: 17 October 2020
Keywords: cryptococcus laurentii; immune competent; immune compromised; cryptococcus neoformans
Non neoformans cryptococci are usually regarded as saprophytes and human infections are rare. C.laurentii is rare of the non neoformans Cryptococci that can cause human infections. Incidence of human infections with Cryptococcus laurentii and albidus has increased over last couple of decades. The risk factors for C. laurentii infections usually include diminished Cell mediated immunity and presence of invasive devices, while mortality risks increases with CNS involvement and age above 45 years. Clinical manifestations are indistinguishable from other invasive yeast infections. High index of suspicion with any yeasts associated with raised inflammatory biomarkers and presence of neutrophils in the specimen’s stained smear is important in the diagnosis and prompt initiation of appropriate treatment since C. laurentii shows low susceptibility to fluconazole.
We report here a case of lower respiratory infection due to Cryptococcus laurentii in a 57 years old female patient with bronchiectasis. The patient was admitted with complaints of fever, dyspnoea with productive cough. She was on antibiotic treatment. Her chest x-ray report revealed infiltrative opacities at right upper mid zone of the lungs and pleural effusion at left lower zone. The patient later also developed quadruparesis and urinary incontinence.
Non-neoformans cryptococci were previously considered to be saprophytes and nonpathogenic to humans [1] Cryptococcus laurentii is frequently used as a biological means to control fruit rot [1]. Cryptococcus are encapsulated yeast, an opportunistic fungal pathogen that may lead to life- threatening infections such as meningoencephalitis and disseminated cryptococcosis, usually in immunocompromised hosts [2].More than 30 species of Cryptococcus are known, only two species are commonly pathogenic in humans, Cryptococcus neoformans and Cryptococcus gatti [2]. In 2006 there were one million cases of cryptococcal meningitis and 625,000 deaths attributable to the disease worldwide in people living with HIV (PLWH) [3].
An Indian study showed that clinical and environmental C. gattii s.l. isolates had high fluconazole MICs [4]. However, despite these differences in antifungal susceptibility among cryptococcal species, the initial cryptococcosis therapy is the same. The clinical management changes are based on clinical presentation and immune status of the individual patient but does not consider the species involved in the disease [5].
The clinical presentation of C. laurentii is similar to that of C. neoformans but the cryptococcal antigen test is often negative [6], and the organism exhibits decreased fluconazole susceptibility [7, 8]. Therefore, accurate identification of the species is essential for appropriate selection of antifungal agent.
A 57 year female patient of bronchiectasis presented with fever, productive cough with yellow expectoration. She had history of pneumonia few months ago and had taken a complete course of antibiotics. She developed quadriparesis and low back pain since 6 months which progressed to inability to walk since 15 days. She further developed bilateral pedal oedema, anorexia and bladder incontinence.
Laboratory investigations showed raised total WBC counts 28,540/cmm (Normal range: 4,000-10,000), neutrophilia (91%) and thrombocytopenia (111000/ micro litre) with ESR of 48 mm at 1 hr. Other biochemical parameters of RFT and LFT were within normal limits. Serology for HIV antibody was negative.
The patient had productive cough with yellow coloured sputum. Her chest x-ray report revealed infiltrative opacities at right upper mid zone of the lungs and pleural effusion at left lower zone. Patient’s spine MRI shows bilateral sacroiliaitis.
Gram’s stained smear of sputum revealed plenty of neutrophils and moderate number of budding yeasts and no bacteria. The budding yeasts appeared larger in size than candida and had a conspicuous large capsule. Fluconazole was added based on the sputum microscopic findings. Culture report was awaited.
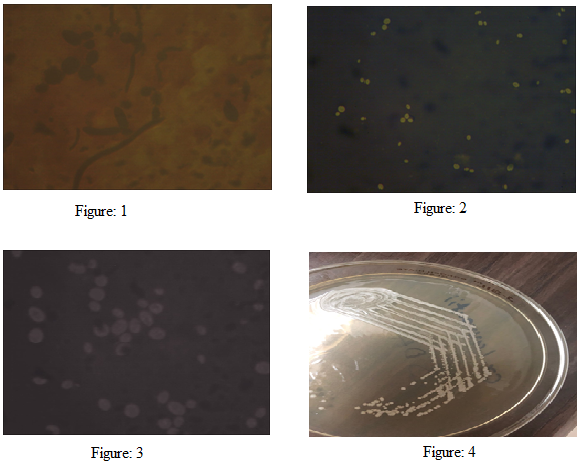
Aerobic bacterial culture was negative. The yeast grown on blood agar and SDA was further processed for ID and susceptibility on Vitek II. On the third day mucoid, cream colour colonies appeared on SDA (Figure 4). Staining with 10% Nigrosin with formaline, showed round budding yeast cells, measuring 5-20 µ in size with distinct large capsule. (Figure 2). The yeast was identified as Cryprococcus laurentii that was resistant to fluconazole, voriconazole, itraconazole and susceptible to amphotericin B by vitek II. The patient was stable for two days but expired third day.
Cryptococcus neoformans/gattii is more commonly associated with infections in immunocompromised patients and sometimes in immunocmpetent hosts [3]. Non C.neoformans / gatti infections are on rise and have been reported several occasions.
C.laurentii infection in HIV positive patient [1]:
C. laurentii in HIV infected patient with low CD4 count-Shankar et al described a case of pneumonia with pleural effusion due to C.laurentii in HIV positive patient. The C.laurentii was also isolated from pleural effusion indicating the involvement of C.laurentii in the pathogenesis of pleural effusion.
C.laurentii infection patient of CRF on CAPD [10]:
Marina Asano et al described a case of Successful Treatment of Cryptococcus laurentii Peritonitis in a Patient on Peritoneal Dialysis. Patient on peritoneal dialysis developed infection with C.laurentii who was treated successfully with voriconazole and removal of the catheter.
C.laurentii infection in non HIV patient [11]:
Miriams T. Castro-Lainez et al presented a case of Cryptococcus laurentii meningitis in a non-HIV patient. The patient was having history of exposure to pigeon droppings and was working at agriculture fields.
C.laurentii in patient with malignancy and on chemotherapy [16]:
A patient with cervical cancer who had received aggressive chemotherapy developed blood steam infection (fungaemia) with C.laurentii as decribed by Rejane Pereira Nevesa et al.
Cuteneous C.laurentii infection [18]:
Alejandro Molina-Leyv et al havereported cutaneous Cryptococcus laurentii infection in an immunocompetent child. The C.laurentii was isolated from skin lesion with limited skin involvement without any visceral or disseminated infection.
C.laurentii Lung abscess infection [22]:
Lynch JP 3rd et al described a pulmonary infection with Cryptococcus laurentii occurred in a patient with dermatomyositis receiving corticosteroid therapy. The isolate was susceptible to amphotericin B but resistant to 5-fluorocytosine, and synergism could not be demonstrated with these 2 drugs. Amphotericin B without surgical resection, concurrent with reduction in the dosage of corticosteroids, resulted in clinical and roentgenogrphic resolution of the infection.
In the present case bronchiectasis was the only obvious predisposing factor for colonization and subsequent disease development as the patient did not have any signs or symptoms suggestive of immunodeficiency and the serology for HIV was negative.
C.laurentii is well known bio-control yeasts reported to reduce postharvest fungal disease of fruits and vegetables [1]. This report raises several questions regarding probable virulence factors of Cryptococcus laurentii, the environmental exposure of people to the Cryptococcus organisms, the role of individual innate immunity and the other host factors in the development of the disease.
As has been described earlier the localized cryptococcal infections can disseminate hematogenously. The correlation between C.laurentii infection and its haematogenous spread to the CNS in development of quadriperesis in this patient remains unexplored due to death of the patient.
Lower respiratory infection due to Cryptococcus laurentii in non-daibetic, HIV negative patient is rare but significant. Generally yeasts in sputum specimen are considered as normal oral flora and not processed unless asked for by a clinician. The present case suggests importance of careful examination of morphology, especially the size and presence of capsule, when yeasts are present predominantly in association with neutrophils in a clinical specimen. The culture and susceptibility could be yielding especially in absence of any other associated pathogen.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
