
Case Report | DOI: https://doi.org/10.31579/2640-1045/113
Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed, Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
Citation: Y M H Elsayed. (2022). Covid-19 Pneumonia with Acute Pulmonary Embolism in a Morbidly Obese Patient; At Home Dramatic Reversal Management. Endocrinology and Disorders. 6(1): DOI:10.31579/2640-1045/113
Copyright: © 2022 Yasser Mohammed Hassanain Elsayed, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 September 2021 | Accepted: 28 December 2021 | Published: 07 January 2022
Keywords: Covid-19; coronavirus; pneumonia; thromboembolism; pulmonary embolism
Rationale: A novel COVID-19 with the severe acute respiratory syndrome had arisen in Wuhan, China in December 2019 Thromboembolism is a critical clinical entity commonly recognized sequel in COVID-19 patients. Interestingly, the presentation of COVID-19 infection with thromboembolism has a risk impact on both morbidity and mortality in COVID-19 patients. Morbid obesity may add over significant risk value in the presence of COVID-19 pneumonia with thromboembolism.
Patient concerns: Middle-aged housewife female COVID-19 morbid obese patient presented to physician outpatient clinic with unilateral pneumonia suspected acute pulmonary embolism.
Diagnosis: COVID-19 pneumonia with acute pulmonary embolism in morbid obesity.
Interventions: CT pulmonary angiography, non- contrasted chest CT scan, electrocardiography, and oxygenation.
Outcomes: Dramatic of both clinical and radiological improvement had happened. Lessons: The combination of morbid obesity, QTc prolongation with COVID-19 infection is an indicator of the over-risk of thromboembolism. It signifies the role of anticoagulants, antiplatelet, anti-infective drugs, and steroids in COVID-19 patients with unilateral pneumonia and acute pulmonary embolism in morbid obesity are effective therapies. An increasing the dose of both low-molecular heparin and oral anticoagulant with a morbidly obese patient was reasonable.
The primary presentation of a current Coronavirus-2 (COVID-19) that is causing vigorous acute respiratory syndrome (SARS) had emerged in Wuhan, China in December 2019 [1]. COVID-19 Disease is an extremely communicable, expeditiously spread, deadly worldwide disease [2]. Despite COVID-19 disease was initially appeared with respiratory symptoms, but cardiovascular affection was frequent rather than the presence of higher rates [3]. Indeed, cardiac complications may be manifested as a late phenomenon in respiratory COVID-19 patients. Thromboembolism is one of the most common cardiovascular complications among COVID-19 patients [3]. There is a higher incidence of thromboembolism in patients with SARS-CoV2 disease. These complications are seen in multiple organ failure starting from cutaneous thrombosis to pulmonary embolism, cerebrovascular accident, and coronary thrombosis [4]. In some observational studies, thrombotic complications were reported as high as 31% in patients indicating critical care admission [4]. The essential role of thrombo-inflammation and endothelial injury in the pathogenesis of the COVID-19 is clearly detected. Overproduction of pro-inflammatory cytokines such as tumor necrosis factor (TNF), Interleukin (IL)-6, IL-8, and IL-1β that is known as “cytokine release syndrome” or “cytokine storm” not unique to this disease. Also, it had described in sepsis and sterile inflammation [4]. This exaggerated cytokine response may lead to multiorgan failure and eventually death in some patients [5]. A high index of clinical suspicion for thrombotic status and their consequences is needed for accurate and quick diagnosis [4]. The optimal approach to the management of anticoagulation in these patients is still obscure in absence of well-conducted trials. There remains major uncertainty in the optimal management of immune-thrombosis as commonly seen in COVID-19 [4]. Both unfractionated heparin and low molecular weight heparin (LMWH) succeed in these patients both prophylactic and therapeutic measures [6, 7]. Higher doses should be considered for those with higher risk patients (eg, obese, active malignancy, prolonged immobility, or recent surgery) [4]. Obesity is associated with numerous pathological conditions, including venous thromboembolism (VTE). Obesity is an independent and moderate risk factor for VTE. The risk increases with body mass index, age, and other acquired risk factors [8].
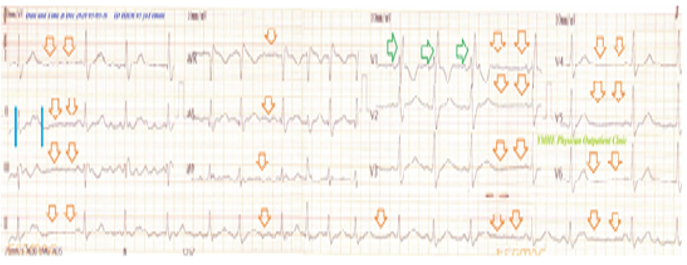
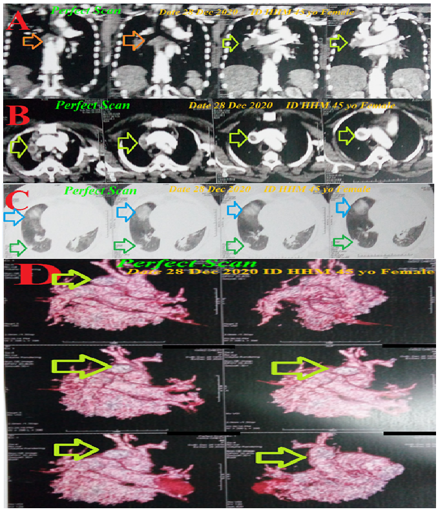
A 45-year-old married housewife Egyptian female patient presented to the physician outpatient clinic (POC) with acute tachypnea and dizziness. Generalized malaise, loss of appetite, loss of smell and taste, and generalized body aches were associated symptoms. The patient gave a history of the symptoms for 6 days. Currently, she had a history of contact with her friend who confirmed a COVID-19 patient in the past 14 days. Informed consent was taken. Upon general physical examination; generally, the patient was tachypneic, distressed, with an irregular pulse rate (sinus arrhythmia with VR; 80 bpm), blood pressure (BP) of 130/70 mmHg, respiratory rate of 32 bpm, the temperature of 37.3 °C, and pulse oximeter of oxygen (O2) saturation of 91%. She appeared very obese with a lasting body weight (one week ago) of 238 kg and a height of 164 cm. According to these weight lengths; calculated BMR was very high (78.6). No more relevant clinical data were noted during the clinical examination. The patient was treated at home with COVID-19 pneumonia with suspected acute pulmonary embolism. Initially, the patient was treated with O2 inhalation by O2 cylinder (100%, by nasal cannula, 5L/min). The patient was maintain treated with cefotaxime; (1000 mg IV every 8hours), azithromycin (500 mg PO single daily dose), oseltamivir (75 mg PO twice daily only for 5 days), and paracetamol (500 mg IV every 8 hours as needed). SC enoxaparin 80 mg twice daily), aspirin tablet (75 mg, once daily), clopidogrel tablet (75 mg, once daily), and hydrocortisone sodium succinate (100 mg IV every 12 hours) were added. Warfarin 5mg oral tablet was added and adjusted with serial INR and PT. The patient was daily monitored for temperature, pulse, blood pressure, and O2 saturation. The initial ECG on presentation showing right bundle branch block (RBBB) with sinus arrhythmia of VR of 78 with prolonged QTc-interval (484 ms in lead II). (Figure 1). The initial complete blood count (CBC); Hb was 10.6 g/dl, RBCs; 4.03*103/mm3, WBCs; 16.6*103/mm3 (Neutrophils; 89.1 %, Lymphocytes: 7.9%, Monocytes; 2%, Eosinophils; 1% and Basophils 0%), Platelets; 158*103/mm3. S. Ferritin was high; 635 ng/ml. D-dimer was very high (2694 ng/ml). CRP was high (98 g/dl). LDH was high (668 U/L). SGPT was normal (39 U/L), SGOT was normal (27 U/L). Serum creatinine was normal (0.7 mg/dl) and blood urea was normal (25 mg/dl). RBS was normal (188 mg/dl). Ionized calcium was slightly low (1.01 mmol/L). The troponin test was negative. After 17 days of management; RBS was normal (107 mg/dl). CBC; Hb was 11.2 g/dl, RBCs; 4.10*103/mm3, WBCs; 8.3*103/mm3 (Neutrophils; 66.4 %, Lymphocytes: 23.5%, Monocytes; 7.1%, Eosinophils; 3% and Basophils 0%), Platelets; 134*103/mm3. Serum ferritin was normal (261 ng/ml). D-dimer was normal (174 ng/ml). CRP was negative (0.5 g/dl). LDH was still high (553U/L). SGPT was normal (22 U/L), SGOT was normal (28 U/L). Serum creatinine (1.2 mg/dl) and blood urea (39 mg/dl) were normal. Ionized calcium was normal; 1.17 mmol/L. The troponin test had still negative. The first CT pulmonary angiography (CTPA) was done on the day of the presentation showing thromboses of the second, distal divisions of the right pulmonary artery, and incomplete filling defects in the superior vena cava. There is single patchy ground-glass pulmonary consolidation in the upper lobe of the right lung. Also, there is right lower lung lobe sub-segmental consolidation (Figure 2A-D). Chest CT without contrast was done within 17 days of treatment showing complete resolution of the above abnormalities (Figure 3). COVID-19 pneumonia with suspected acute pulmonary embolism in morbid obesity was the most probable diagnosis. Within 15 days of the above management, the patient finally showed nearly complete clinical, radiological, and laboratory improvement. The patient was continued on aspirin tablet (75 mg, once daily) and warfarin 8 mg oral tablet with follow-up with serial INR and PT. Further recommended cardiac chest follow-up, and weight reduction was advised.

• Overview:
• Middle-aged housewife female COVID-19 morbid obese patient presented to physician outpatient clinic with unilateral pneumonia with suspected acute pulmonary embolism.
• The primary objective for my case study was the presence of COVID-19 pneumonia with suspected acute pulmonary embolism in a morbidly obese patient in POC.
• The secondary objective for my case study was the question of; how did you manage the case at home?
• There was a history of direct contact to confirmed the COVID-19 case.
• The presence of direct contact to confirmed the COVID-19 case, and unilateral ground-glass consolidation on top of acute tachypnea will strengthen the COVID-19 diagnosis.
• The tachypnea, hypoxia, consolidation, electrocardiographic (ECG) RBBB and elevated d-dimer are highly suggestive of associated pulmonary embolism.
• An associated morbid obesity, ECG RBBB with QTc prolongation, and marked elevated d-dimer in the presence of COVID-19 pneumonia may carry a bad prognostic outcome and is indicating a high-risk condition.
• An accompanied ECG sinus arrhythmia is insignificant and valueless.
• An increasing the dose of both low-molecular heparin (enoxaparin) and oral anticoagulant (warfarin) with a morbidly obese patient was reasonable.
• The dramatic reversal of clinical, electrocardiographic, and radiological after anticoagulants, antiplatelet, anti-infective drugs, and steroids had happened.
• A nearly complete clinical, radiological, and laboratory improvement that occurred after the management with anti-infective drugs, anticoagulants, steroids, and antiplatelet strongly implies their effects.
• Blood pressure, respiratory rate, pulse, and O2 saturation are a strong guide for clinical follow-up in COVID-19 patients.
• A gradual decreasing the level of elevated CRP, d-dimer, and serum ferritin may be used as another good laboratory guide for follow-up for COVID-19 pneumonic patients.
• Acute coronary syndrome was the possible differential diagnosis for the current case study.
• I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison.
• The only limitation of the current study was the unavailability of echocardiography.
The combination of morbid obesity, QTc prolongation with COVID-19 infection is an indicator of the over-risk of thromboembolism. It signifies the role of anticoagulants, antiplatelet, anti-infective drugs, and steroids in COVID-19 patients with unilateral pneumonia and acute pulmonary embolism in morbid obesity are effective therapies.
An increasing the dose of both low-molecular heparin and oral anticoagulant with a morbidly obese patient was reasonable.
CBC: Complete blood count
COVID-19: Coronavirus disease 2019
CTPA: CT pulmonary angiography
ECG: Electrocardiography
IV: Intravenous
O2: Oxygen
POC: Physician outpatient clinic
RBBB; Right bundle branch block
SGOT: Serum glutamic-oxaloacetic transaminase
SGPT: Serum glutamic-pyruvic transaminase
VR: Ventricular rate
VTE: Venous thromboembolism
There are no conflicts of interest.
I wish to thanks the nurse team of the intensive care unit to give me extra copies of the ECG to help me and my wife to save time and improving the conditions for supporting me.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
