
Case Report | DOI: https://doi.org/10.31579/2690-8794/041
Department of General Surgery, Izmir Bozkaya Research and Education Hospital İzmir, Turkey
*Corresponding Author: Ethem Bilgiç, Department of General Surgery, Izmir Bozkaya Research and Education Hospital İzmir, Turkey.
Citation: Ethem Bilgiç (2020) COVID-19 cases: definitive, or not? J. Clinical Medical Reviews and Reports 2(7); DOI: 10.31579/2690-8794/041
Copyright: © 2020, Ethem Bilgiç, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 August 2020 | Accepted: 31 August 2020 | Published: 02 October 2020
Keywords: severe acute respiratory syndrome corona virus 2; corona virus Pandemics
Context: A cluster and increase in pneumonia cases with unknown cause were detected in Wuhan, Hubei province, China, in December 2019. These cases were reported to be associated with a new coronavirus type by the Chinese health authorities on January 7, 2020. The first case in Turkey was diagnosed on March 11, 2020. COVID-19 (SARS-CoV-2 infection) guide was prepared for the pandemic by the Ministry of Health scientific committee. However, despite strong clinical, laboratory and radiological suspicions, there are also patients who do not meet the exact case definition.
Case report: In this case report, we aimed to discuss two cases that did not meet the definitive case definition and followed up in our clinic.
Conclusions: Although gold standard method for the definitive diagnosis of SARS-CoV-2 infection is PCR, rapid antibody tests and CT findings are used in combination with PCR for a more effective struggle in the pandemic process would enhance rapid diagnosis of cases, necessary treatment and isolation measures to prevent transmission. It is thought that it would be useful to make case definitions.
Coronaviruses are common among humans, mammals and birds; enveloped ribonucleic acid(RNA) viruses that cause respiratory, enteric, hepatic and neurological diseases. There are six types of coronavirus known to cause disease in humans. Four of them (229E, OC43, NL63 and HKU1) typically cause cold symptoms in individuals with healthy immune systems. The other two are SARS-CoV which cause severe acute respiratory syndrome and MERS-CoV, which causes Middle East Respiratory Syndrome. They are zoonotic infections with mortality rates of 9.6% and 34.4%, respectively [1, 2].
A cluster and increase in pneumonia cases with unknown cause were detected in Wuhan, Hubei province, China, in December 2019 [3, 4]. These cases were reported to be associated with a new coronavirus type by the Chinese health authorities on January 7, 2020. The World Health Organization (WHO) termed the clinical picture of the new coronavirus "corona virus disease 2019" (COVID-19) and the virus that caused this disease severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on February 11, 2020 [5]. The main transmission routes of the virus have been reported as respiratory droplets and close contact between people. After that, COVID-19 has spread all over the world and has become a global public health problem.
The first case in Turkey was diagnosed on March 11, 2020. COVID-19 (SARS-CoV-2 infection) guide was prepared for the pandemic by the Ministry of Health scientific committee. This guideline contains information about the virus that caused COVID-19, ways of transmission, case definition, diagnostic methods, strategy and behavior patterns for COVID-19 case or contacted in follow- up. The “COVID-19 (2019-nCoV Disease) Guide” is updated in line with current WHO recommendations and current scientific developments. According to this guide, cases with SARS-CoV-2 detected by molecular methods (polymerase chain reaction) from respiratory samples are defined as definitive cases [6]. However, despite strong clinical, laboratory and radiological suspicions, there are also patients who do not meet the exact case definition.
In this case report, we aimed to discuss two cases that did not meet the definitive case definition and followed up in our clinic.
We declare that all patients gave their consent to have their cases to reported.
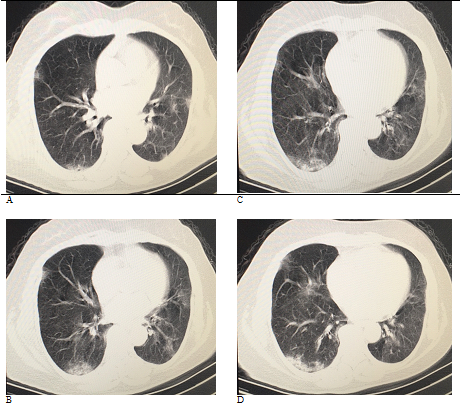
Case 1: Our first case, a 69-year-old male patient applied to our emergency department with complaints of fever and cough on 27.03.2020. It was learned from the anamnesis of the patient that he came from Istanbul to Didim by bus on 25.03.2020, traveled with his wife and his complaints had been present for five days. The patient had a history of hypertension and antihypertensive use. In the physical examination of the patient, fever was measured as 37.9oC. System examination was normal. White blood cells (WBC): 4.32 K/μL (4.6-10.2 K/μL), platelet count(PLT): 115 K/μL (142-424 K/CRL), c-reactive protein (CRP): 8.4 mg/L (0-5 mg/L) was determined in laboratory tests. In the non-contrasted thorax computed tomography (CT) examination, “Peripherally located ground-glass views and patches of stone in the middle lower zones in both lungs are noteworthy. The peripheral location and patterns of the lesions were evaluated as highly significant in terms of COVID-19.” as reported (Figures 1A and 1B).

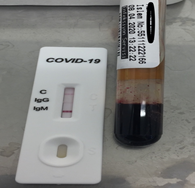
The patient was hospitalized by isolation precautions. Levofloxacin 500 mg IV 1x1 and oseltamivir 75 mg capsule 2x1 was started for treatment. Nasopharyngeal swab sample was taken for COVID-19 polymerase chain reaction (PCR) test on 27.03.2020 and 30.03.2020. However, PCR tests were negative. On 31.03.2020, hydroxychloroquine 200 mg tablet was added to the treatment of the patient whose fever continuedon the first day as 2x2, then 2x1 and continued for five days. A nasopharyngeal swab sample was taken from the patient for the third time on 06.04.2020 for PCR testing and control CT without contrast was taken. The third PCR test was also negative. The control CT was reported as “draws attention in the form of patchy peripheral frosted glass in both lungs on the posterior segment of the right upper lobe on the right, and on the left at the level of the lower lobe of the upper lobe, on the right middle lobe, on the levels of the superior segment of both lower lobes and the posterobasal segment of both lower lobes. Thin linear density increases accompany the existing ground glass shapes and curvilinear streaks are added in basal segments. Occasionally, cobblestone views are formed. The findings are peripheral and bilateral. Compared to the older CT, there is an increase in the number and area of the lesion. The findings are compatible with the mid-term natural course in terms of its radiological course. Although progression is observed, it does not mean clinical progression. The patient's findings have been evaluated in favor of the natural process of COVID-19 infection and clinical evaluation is recommended for progression.” Nasopharyngeal swab sample was taken from the patient for COVID-19 PCR test again on 08.04.2020. After the delivery of the rapid diagnostic kit, the patient was administered a rapid test with COVID-19 (SARS-CoV-2) Antibody Test Kit (Colloidal Gold) by recommendations of producer company (Anhui Deep Blue Medical Technology, Anhui, China). The last PCR test was negative but the rapid antibody test, COVID-19 immunoglobulin M (IgM) was positive (Figure 2). The patient, whose fever and cough complaints decreased in the follow-up and the respiratory distress did not develop, was discharged on the 15th day of hospitalization with the decision to follow up at home.
Case2: The second case was a 67-year-old female patient and was the first case’s wife. The patient, who had a history of bus travel with the first case, was called to the Infectious Diseases Policlinic on 28.03.2020 after the first patient was hospitalized. Her complaint was soreness of all body, not cough and breathe distress. She had no fever. Her physical examination is normal. WBC: 4.71 K/μL (4.6-10.2 K/μL), hemoglobin (HGB): 11.7 g/dl (12.2-18.1 g/dl), hematocrit (HCT): 34.3% (37.7-53.7%), PLT: 148 K/μL (142-424 K/μL), CRP: 11.2 mg/L (0-5 mg/L) were resulted in laboratory tests. The non-contrast thoracic CT was reported as “The right lower lobe superior segment in both lungs, and both lower lobe anterobasal, laterobasal and posterobasal segments in the form of patches of peripherally located frosted glass, and patches of cobblestones are remarkable. The findings are highly suspicious for COVID-19 infection.” (Figure 3). The patient was hospitalized for further examination, isolation and observation. The nasopharyngeal swab sample was taken for the COVID-19 PCR test on 28.03.2020. Levofloxacin 500 mg IV 1x1 and oseltamivir 75 mg capsule 2x1 were started for treatment. The PCR test was positive on 30.03.2020, then she was transferred to the city pandemic hospital.
The first cases were detected in the United States, Russia, the Philippines, Singapore, Japan, Sweden, Canada, England, Spain immediately after the World Health Organization declared a global public health emergency against coronavirus disease on January 30, 2020. This rapid spread demonstrated the importance of the need for fast and effective identification methods that can be used in health institutions dealing with the diagnosis and treatment of COVID-19.7
The gold standard for the diagnosis of COVID-19 is the identification of viral nucleic acid by polymerase chain reaction. However, the polymerase chain reaction method is a long time method that should be done meticulously. Also, some potential COVID-19 cases may have false negative results that may be detrimental to the control of the outbreak.8 We met a similar situation in the two cases we described above. The second case resulted in a positive COVID-19 PCR test, then she was recorded as definitive case, included the total number of cases in Turkey. However, despite the fact that the first case was clinically and radiologically compatible, positive COVID-19 rapid antibody test, the COVID-19 PCR test was negative and was not recorded as a definitive case.
In one retrospective study, the CT findings of 53 patients with COVID-19 were compared with PCR test. It has been reported that the diagnosis of viral pneumonia by CT could be three days earlier than PCR test, and CT could be standard method for COVID-19 diagnosis [7]. So, isolation and treatment of patients can be done earlier with rapid diagnosis and potential transmission can be prevented. Another fast, simple and sensitive method of diagnosing COVID-19 is to measure SARS-CoV-2 specific antibodies in peripheral blood.While the first defense mechanism against viral infections is immunoglobulin M (IgM), immunoglobulin G (IgG) is important in long-term immunity and immune memory [9]. In one study, it was reported that IgM antibodies could be measured in patient blood three to six days after SARS infection and eight days after IgG antibodies [10]. Hence, rapid detection of IgM and IgG antibodies will make an important contribution to the diagnosis and treatment of COVID-19. Li et al. reported the sensitivity as 88.66% and the specificity as 90.63% of rapid tests [8].These tests are important and quick method for local health institutions that do not have the possibility to perform PCR, because they do not require special equipment and personnel.
Although gold standard method for the definitive diagnosis of SARS-CoV-2 infection is PCR, rapid antibody tests and CT findings are used in combination with PCR for a more effective struggle in the pandemic process would enhance rapid diagnosis of cases, necessary treatment and isolation measures to prevent transmission. It is thought that it would be useful to make case definitions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
