
Research Article | DOI: https://doi.org/DOI:10.31579/2639-4162/060
1*Health Center Santa Maria de Benquerencia Toledo, Spain.
*Corresponding Author: Jose Luis Turabian, Health Center Santa Maria de Benquerencia Toledo, Spain.
Citation: Jose Luis Turabian (2022). Covid-19 Breakthrough Infections In Vaccinated People With Vaccine Booster In 2022 Versus Covid-19 Cases In Unvaccinated People In 2020: A New Disease Whose Clinic We Should Know Or Another Cause Of The Old Symptoms Of The Common Cold?. J. General medicine and Clinical Practice, 5(2); DOI:10.31579/2639-4162/060
Copyright: © 2022 Jose Luis Turabian, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 May 2022 | Accepted: 08 June 2022 | Published: 15 June 2022
Keywords: COVID-19; SARS-CoV-2; vaccination; breakthrough infection; epidemiological characteristic; symptoms; acute respiratory Infections; secondary analysis; general practice
Background It is not clear whether the symptoms of covid-19 have varied throughout the pandemic and what effect vaccination may have had. Objective To compare clinical-epidemiological characteristics between cases of covid-19 in 2020 without vaccination, and covid-19 breakthrough infections in vaccinated people with vaccine booster during 2022 in general medicine. Methodology Comparison of secondary data of cases of covid-19 without vaccination of previous studies in 2020, with other cases of covid-19 breakthrough infections in vaccinated people with vaccine booster in 2022, all of them carried out in the same population of patients treated in a general medicine office in Toledo, Spain. Results Cases of covid-19 breakthrough infections in vaccinated people with vaccine booster in 2022 (N= 46) vs. cases in 2020 without vaccination (N=100), differed statistically by being older, having more sociohealth workers, presenting more chronic diseases, and having more ENT symptoms and fewer digestive and psychiatric ones. Conclusions In the context of general medicine in Toledo (Spain), the cases of covid-19 in 2022 are different from those of 2020, affecting older people and showing symptoms of upper respiratory tract infection. This change in symptoms that causes covid-19 to present itself as a common cold can do away with preventive precautions, so it is important to test to see what the symptoms mean. |
In December, 2019, a pneumonia associated with a novel coronavirus emerged in Wuhan, China. What started as a cluster of patients with a mysterious respiratory illness was later determined to be coronavirus disease 2019 (COVID-19). The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was subsequently isolated as the causative agent that it is primarily transmitted between people via respiratory droplets and contact routes [1-3].
At the beginning of the pandemic, SARS-CoV-2 infection presented clinically with fever, fatigue, myalgias, conjunctivitis, anosmia, dysgeusia, sore throat, nasal congestion, cough, dyspnea, nausea, vomiting, and/or diarrhea. In most critical cases, symptoms could become into acute respiratory distress syndrome accompanied by a runaway inflammatory cytokine response and multiorgan failure [1]. That is, systemic and pulmonary manifestations predominated, with an increasing emphasis placed on gastrointestinal symptoms as both diagnostically and prognostically important [1].
However, covid-19 has shown a wide variety of symptoms; Much remains unknown about why there is such a wide range of responses, and it has been claimed that up to 40% of infections may be asymptomatic [4-6]. SARS-CoV-2, like all viruses, are constantly changing. These changes occur over time and can lead to the emergence of variants that may have new characteristics. In the course of the covid-19 pandemic, SARS-CoV-2 has mutated enough to escape first-line immune defenses, specifically antibodies. This is why we are seeing breakthrough infections even in highly vaccinated populations. Booster vaccination was expanded in coincidence with introduction of omicron variant into the population, causing the largest epidemic wave of SARS-CoV-2 infections in Spain and the world [7-10].
Research of covid-19 symptoms in 190 countries during 2020 showed that the frequency of symptoms of cough, fever, and loss of smell, was different depending on the country and the presence of underlying health conditions such as asthma and diabetes [11]. In addition, it seems that the symptoms with which covid-19 manifested itself at the beginning of the pandemic are no longer the same. Fever seems not to be the most permanent symptom; loss of taste and smell also do not, and runny nose, sore throat or dry cough and headache appear as very frequent symptoms in people with the vaccine [12].
In the current Surveillance and Control Strategy Against Covid-19 in Spain, since April 2022 [13] symptoms compatible with covid-19 are defined as acute respiratory symptoms consisting of sudden onset in the last 10 days of any of the following symptoms: cough, dyspnea, sore throat, or runny nose, with or without fever. Likewise, the UK's official list of covid-19 symptoms was recently updated to include sore throat, fatigue, headache which are now commonly associated with the virus [14].
Understanding the variation of symptoms by location and temporality is crucial for clinical practice; It could help speed diagnosis, predict outcomes more accurately, and guide treatment, especially as new variants emerge. Likewise, the fact of being able to reflect this variation in symptoms in public health messages can contribute to prevention. It has been said that future work should focus on symptom profile variation in emerging SARS-CoV-2 virus variants [11].
In this context, a study is presented based on the secondary analysis of data previously published, referring to the same population attended in a general medicine consultation, and collected by the same general practitioner, which are used to compare clinical-epidemiological characteristics of COVID-19 breakthrough infections in vaccinated people with booster in 2022 vs. patients with COVID-19 without vaccination during 2020.
A secondary analysis of data collected, processed, analyzed, and published for purposes other than this research objectives, was conducted to compare clinical-epidemiological characteristics between cases of covid-19 in 2020 without vaccination, and covid-19 breakthrough infections in vaccinated people with vaccine booster, in general medicine.
Therefore, this study compares data from previous studies:
1. The set of two previous studies on covid-19 cases. A study of covid-19 cases from March 1 to May 31, 2020 (15), and another study from March 15 to November 15, 2020 [16]. In 2020 there were still no vaccines against covid-19; they are therefore cases without vaccination. In this period, from March to April, in Spain, the A lineage of the coronavirus predominated, especially the SEC7 and SEC8, and from summer to December, 2020, the 20E (EU1) variant [17, 18].
And 2. A study of covid-19 breakthrough infections in vaccinated people with vaccine booster from December 2021 to February 2022 (19, 20). In this period, the omicron variant was dominant in Spain after having displaced the Delta variant [21].
All studies were conducted on the same population: patients saw in a general medicine office in Toledo, Spain, which has a list of 2,000 patients > 14 years of age (in Spain, GPs care for people > 14 years of age, except for exceptions requested by the child's family and accepted by the GP). The GPs in Spain work within the National Health System, which is public in nature, and are the gateway for all patients to the system, and each person is assigned a GP [22]. The methodology of all studies has been previously published [15, 16, 19, 20].
Current study objective
To compare selected clinical-epidemiological characteristics between cases of covid-19 in 2020 without vaccination, and covid-19 breakthrough infections in vaccinated people with vaccine booster during 2022, in general medicine.
Collected variables
Variables for which data were available in all previous studies that were to be compared were included. The following variables were collected: age, sex, socio-health worker, symptoms and chronic diseases (defined as "any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non-reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment” [23-25], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD-10 Version: 2019 [26], and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths / min; pulse oxygen saturation ≤ 93% with room air at rest; arterial partial pressure of oxygen / oxygen concentration ≤ 300 mm Hg) [27].
Statistic análisis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test, for percentages (according to the number the expected cell totals), and the Student t test for the mean.
cases of covid-19 that occurred during 2020 were compared with 46 cases of covid-19 breakthrough infections in vaccinated people with vaccine booster in 2022. The cases of covid-19 breakthrough infections in vaccinated people with vaccine booster vs. cases in 2020 without vaccination were statistically different for being older, having more socio-health workers, presenting more chronic diseases, and having more ENT symptoms and fewer digestive and psychiatric symptoms (TABLE 1, TABLE 2, and TABLE 3).
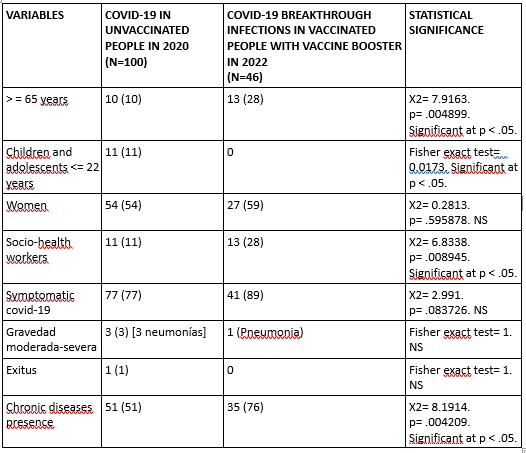
( ): Denotes percentages; NS: Not significant
CRHONIC DISEASES ACCORDING TO WHO, ICD-10 GROUPS*
| COVID-19 IN UNVACCINATED PEOPLE IN 2020 (N=100)
| COVID-19 BREAKTHROUGH INFECTIONS IN VACCINATED PEOPLE WITH VACCINE BOOSTER IN 2022 (N=46) | STATISTICAL SIGNIFICANCE |
| -II Neoplasms | 3 (3) | 5 (3) | X2 with Yates correction= 0. p= 1. NS |
| -II Diseases of the blood | 1 (1) | 1 (1) | Fisher exact test= 1. NS |
| -IV Endocrine | 26 (23) | 24 (16) | X2= 1.7185. p= .189886. NS |
| -V Mental | 11 (10) | 8 (6) | X2= 1.6685. p= .196455. NS |
| -VI-VIII Nervous and Senses | 9 (8) | 14 (10) | X2= 0.2191. p= .639699. NS |
| -IX Circulatory system | 16 (14) | 18 (12) | X2= 0.1744. p= .676207. NS |
| -X Respiratory system | 12 (10) | 8 (6) | X2= 2.3279. p= .127073. NS |
| -XI Digestive system | 11 (10) | 18 (12) | X2= 0.45. p= .50234. NS |
| -XII Diseases of the skin | 3 (3) | 8 (6) | X2 with Yates correction= 0.6649. p= .414823. NS |
| -XIII Musculo-skeletal | 10 (9) | 17 (12) | X2= 0.5527. p= .457213. NS |
| -XIV Genitourinary | 10 (9) | 23 (16) | X2= 0.6762. p= .410901. NS |
| TOTAL* | 112 (100) | 144 (100) | --- |
Table 2: Comparison of Crhonic Diseases between Covid-19 in Unvaccinated People in 2020 and Covid-19 Breakthrough Infections in Vaccinated People with Booster In 2022
( ): Denotes percentages; NS: Not significant; *Patients could have more than one chronic disease. The percentages of chronic diseases are over the total of chronic diseases
SYMPTOMS * ACCORDING TO WHO, ICD-10 GROUPS
| COVID-19 IN UNVACCINATED PEOPLE IN 2020 (N=100)
| COVID-19 BREAKTHROUGH INFECTIONS IN VACCINATED PEOPLE WITH VACCINE BOOSTER IN 2022 (N=46) | STATISTICAL SIGNIFICANCE |
| General (discomfort, asthenia, myalgia, fever, artralgias) | 24 (31)
| 34 (31) | X2= 0.0014. p= .969854. NS |
| Respiratory (cough, dyspnea, chest pain) | 19 (25)
| 24 (22) | X2= 0.2088. p= .647699. NS |
| ENT (Anosmia / ageusia, odynophagia, rhinorrhea, pharyngeal dryness-mucus, epixtasis) | 8 (10)
| 41 (37) | X2= 16.9281. p= .000039. Significant at p < .05. |
| Digestive (anorexia, nausea / vomiting, diarrhea, abdominal pain) | 9 (12)
| 3 (3) | X2 with Yates correction= 4.6562. p= .030941. Significant at p < .05. |
| Neurological (headache, dizziness, mental confusion -brain fog) | 7 (9)
| 8 (7) | X2= 0.2029. p= .652354. NS |
| Psychiatric (Anxiety, insomnia) | 8 (10)
| 0 | Fisher exact test = 0.0007. Significant at p < .05.
|
| Skin (chilblains, flictenas, rash, petechiae) | 2 (3)
| 0 | Fisher exact test= 0.1682. NS |
| Total symptoms* | 77 (100) | 110 (100) | --- |
Table 3: Comparison of Symptoms between Covid-19 in Unvaccinated People in 2020 and Covid-19 Breakthrough Infections in Vaccinated People with Booster In 2022
( ): Denotes percentages; NS: Not significant; *Patients could have more than one symptom; the percentages are over the total of symptoms
One might think that the symptoms of covid-19 are still the same today compared to the start of the pandemic, because the virus is still the same and symptoms not depend on the variant, but on how the body reacts to the virus. However, the understanding of covid-19 is evolving. The main clinical difference between flu and covid-19 was said to be that the latter had shortness of breath as a differential symptom [28]. In the same population of this study, in 2020,we proposed that symptoms suggestive of covid-19 vs. common cold or flu, were cough, fever, dyspnea, general pain, asthenia, nausea-vomiting, pneumonia [29]. On the other hand, it has been found that the frequency of the main symptoms in 2020 (cough, fever and loss of smell), was different depending on the country and the presence of underlying health conditions such as asthma and diabetes [11]. Thus, it must also be taken into account that the symptoms may not depend so much on the variant, but on how the organism reacts to the virus [30]; it could be said that not everything depends on the pathogen, but also on the host and environment [31].
Comparison with other studies
1. Symptoms of covid at the beginning of the pandemic
In the early stage of the pandemic, symptoms are related only to the initial strains of SARS-CoV-2 that circulated between April and September 2020 and are not related to later variants such as Delta or Omicron. Presentations of covid-19 in unvaccinated people in this first period of the pandemic have ranged from mild/asymptomatic symptoms to severe disease and mortality. Thus, the most frequently reported initial signs or symptoms in the first 12 US patients confirmed with COVID-19 from January 20 to February 5, 2020, were cough and fever, during the course of the disease reported cough, fever, diarrhea, and vomiting [32].
While a wide range of symptoms can accompany COVID-19, the CDC found that the vast majority of patients exhibited one of three symptoms: fever, cough, and shortness of breath. In a Centers for Disease Control and Prevention study involving 164 people in 16 states who had confirmed cases of coronavirus between January 14 and April 4, 2020, researchers found that 96% of patients had a fever, cough, or shortness of breath. About 45% had all three symptoms. The most frequent symptom was cough (84%) followed by fever (80%). COVID-19 patients also showed other symptoms, including chills, muscle pain, headache, fatigue, and digestive problems such as nausea, abdominal pain, vomiting, or diarrhea. Approximately half of the patients reported one or more gastrointestinal symptoms; among these, diarrhea was reported more frequently (38%) and vomiting less frequently (13%) (32, 33).
In a small case series in Japan from 13 to 25 February 2020, 83% had fever, 33% had cough, and 33% had gastrointestinal symptoms. All patients exhibited bilateral ground-glass opacities on computed tomography [34]. In another study of cases of 2019-nCoV in Wuhan Jinyintan Hospital, China, from Jan 1 to Jan 20, 2020, patients had fever in 83%, cough 82%, shortness of breath 31%, muscle ache 11%, confusion 9%, headache 8%, sore throat 5%, rhinorrhoea 4%, chest pain 2%, diarrhoea 2%, and nausea and vomiting 1%. According to imaging examination, 75% patients showed bilateral pneumonia, 14% patients showed multiple mottling and ground-glass opacity, and 1% had pneumothorax [35]. In one study from Wuhan, China, examining >1000 cases of covid-19, the predominant symptoms were fever and dry cough, with 80%. Other studies noted that gastrointestinal symptoms, such as diarrhea (2%–10.1%) and nausea and vomiting (1%–3.6%), were present in a nontrivial proportion of patients. Moreover, a significant proportion of patients presented initially with those atypical gastrointestinal symptoms. It was reported that anosmia and dysgeusia were early symptoms associated with covid-19 (1). Overall, nearly 20% of patients with covid-19 in China developed severe pneumonia [36].
Other studies for the 2020 period showed that fever occurred in 83-88%, Dry cough in 46-82%, Malaise and fatigue in 11-70%, Body aches and myalgias in 11-44%, Pharyngitis/pharyngalgia in 5-17%, Loss of appetite in 40-50%, Diarrhea in 2-15%, Nausea and vomiting in 1-10%, Headache 6-12%, Dizziness 9%, and Confusion 9% (1). Others reports have identified a variety of symptoms associated with covid-19, that include fever or chills, cough, shortness of breath, fatigue, muscle or body aches, headache, loss of taste or smell, sore throat, stuffy or runny nose, nausea or vomiting and diarrhea, and others such as malaise [37-40]. And it was emphasized that taste and smell disorders and diarrhea were important markers in COVID-19 infection [41].
In this sense, the presence of anosmia, ageusia, fever, new persistent cough, chills, loss of appetite, and muscle pain were reported to be the seven symptoms that (out of a total of 26) best predict a positive test result for SARS CoV infection in adults, based on a British analysis of more than 1 million participants studied between June 2020 and January 2021 [42, 43]. An investigation, led by Imperial College London, analyzed data on symptoms reported by 78,299 people in 190 countries between April and September 2020. Of these, 64,699 were symptomatic. Responders who tested positive were more likely to report joint pain, loss of appetite, and loss of smell and taste [11]. Along these same lines, we report in a study in the same population of the GP consultation that this study, from March 9 to April 3, 2020, where covid-19 diagnostic test was not initially performed, that patients who should be considered as probable covid-19 were those who presented fever, dyspnea, diarrhea, nausea / vomiting, or physical signs of pneumonia, with long duration of symptoms [29].
2. Symptoms in COVID-19 breakthrough infections in vaccinated people in 2022
Since the start of the pandemic, general practitioners (GPs) have been familiar with the hallmark symptoms of contagion, including loss of taste or smell, fever, cough, shortness of breath, and fatigue. But what happens now, more than a year later, when in many countries more than half the population is vaccinated? Have the symptoms changed since delta and omicron are the most common variants in some countries? There are few data in this regard and much remains to be clarified [44]. So far we know that the majority of patients with covid-19 after vaccination usually have mild disease or even remain asymptomatic [45]. The symptoms with which covid-19 manifested at the beginning of the pandemic are no longer the same as in the vaccinated population. The symptoms of COVID-19 change for those vaccinated: fever is no longer the most permanent symptom, neither is the loss of taste and smell, and rhinorrhea, sore throat or dry cough and headache appear as very frequent symptoms in people with the vaccine [46].
Generally speaking, it would appear that vaccinated people who contract covid-19 and experience symptoms are prone to them in the same way that an unvaccinated person might experience them but probably with different severity. So, while a person who is not vaccinated may experience a very bad headache, a very severe sore throat, or very serious gastrointestinal problems, those same symptoms would be less severe in a person who is vaccinated [47]. In an observational study evaluating reported clinical symptoms of 63,000 confirmed cases of covid-19 over two time periods (June to November 2021 when the Delta variant predominated and December 2021 to January 2022 when Omicron predominated), showed that the most frequent were nasal congestion (77-82%), headache (75-78%), sneezing (63-71%) and sore throat (61-71%) (48).
In a study conducted in Israel, of 1,497 fully vaccinated health workers, 39 (3%) were positive for SARS-CoV-2, of which 69% were tested solely for having had contact with someone positive. Of the 39 patients who had covid-19 after vaccination, 33% remained asymptomatic and among the symptomatic, 36% reported nasal congestion, 28% myalgia, 28% loss of smell or dysgeusia, and 21
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
