
Case Report | DOI: https://doi.org/10.31579/2690-1919/217
1 Professor and Head/Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No.(1) Defence Services General Hospital (1000-Bedded).
2 Senior Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded).
3 Consultant Physician and Haematologist, No. (1) Defence Services General Hospital (1000-Bedded).
4 Consultant Nephrologist, No. (1) Defence Services General Hospital (1000-Bedded).
5 Nephrology Fellow, No. (1) Defence Services General Hospital (1000-Bedded).
6 Assistant Lecturer / Consultant physician, Defence Services Medical Academy.
*Corresponding Author: Khin Phyu Pyar, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No.(1) Defence Services General Hospital.
Citation: Khin P. Pyar, Soe W. Hlaing, A. Aung, Zar N. H. Aung, Nyan L. Maung, et al. (2022). The Effective Management and Outcome of Hand Burns. J Clinical Research and Reports, 10(2); DOI:10.31579/2690-1919/217
Copyright: © 2022, Khin Phyu Pyar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 November 2021 | Accepted: 27 December 2021 | Published: 07 January 2022
Keywords: COVID-19; stress reaction; central cyanosis; dark urine; oliguria; jaundice; anaemia; methemoglobinemia; suicide; naphthalene mothball poisoning; exchange transfusion
Case Summary
A young man presented with abdominal pain and vomiting after eating Naphthalene Mothball. He had dyspnea, central cyanosis (SaO2 on air was 67% on air), marked pallor, deep jaundice and dehydration. His urine color was black; and, his plasma in clotted blood sample was brownish. He was treated as methemoglobinemia due to suicidal Naphthalene Mothball poisoning with fluid and electrolyte replacement, ascorbic acid, N-acetylcystine and exchange transfusion twice with four units of whole blood. Dramatic improvement in central cyanosis immediately following exchange transfusion. Psychiatric consultation and counselling were done; he admitted the main reason for committing suicide was socioeconomic stress due to COVID-19.
In COVID-19 pandemic, the incidence of mental health problems are increasing; anxiety, depression, alcoholism, suicide and stress disorder (Shevlin et al., 2020) (Stevenson & Wakefield, 2021) (Sahimi et al., n.d.) (Ueda et al., 2020). The impact of the COVID-19 pandemic on stress, mental health and coping behaviour were found to be changing (Voltmer et al., 2021).
Naphthalene (mothball) is a commonly used deodorizer. Naphthalene poisoning is a rare form of toxicity that may occur after ingestion, inhalation, or dermal exposure to naphthalene-containing compounds such as mothballs. Poisoning may present with acute manifestation or chronic form depending on extent of poisoning. It is relatively common in children due to accidental poisoning (Sarangi et al., 2016). Even neonates may have poisoned due to inhalation from mother. Severe haemolysis from naphthalene poisoning occurs particularly in patients with G6PD deficiency, who have a low tolerance to oxidative stress. Renal failure as a complication of naphthalene-induced haemolysis and haemoglobinuria has been reported. Early recognition of methemoglobinemia following anesthetic drugs is important in operating theater and recovery room (Sharma & Haber, 2002) (Cefalu et al., 2020). In mild cases, SaO2 may be normal (Uthuman et al., 2019).
Extremely rare form of poisoning was reported in patients with end stage renal disease on maintenance hemodialysis due to contamination of dialysis fluid with H2O2 in dialysis water (Newbigging et al., 2009).
Mode of entry of naphthalene, age of patients and their underlying medical diseases in several case reports were interesting: (1) the youngest one was neonate due to inhalation or ingestion of mother during gestation (Molloy et al., 2004) (Sahni et al., 2019); (2) mother and baby due to ingestion (Molloy et al., 2004); (3) two year old baby presented with metabolic acidosis due to ingestion (Annamalai et al., 2012); (4) 21 month old baby with G6PD deficiency due to ingestion (Dela Cruz et al., 2019); (5) two patients with autism due to ingestion (Volney et al., 2018) (Kapoor et al., 2014); (6) a case of carcinoma of stomach following benzocaine spray (Lockhart & Ong, 2018); (7) severe COVID-19 infection (Faisal et al., 2020) (Naymagon et al., 2020); (8) patients requiring renal replacement therapy (Kundra et al., 2015) (Deo et al., 2016).
A 21-year-old male was brought to hospital last month because he had abdominal pain and vomiting after eating Naphthalene Moth ball. He was drowsy, dehydrated, dyspnoeic, respiratory rate 32/min, SaO2 on air was 67% on air, it increased to only 70% with 10 L of oxygen (Double Flow Meter). Blood pressure was 160/90 mmHg, pulse rate 124/ minutes. He had marked pallor and was deeply jaundiced. Abdomen was soft and non-tender. Urine color was black.
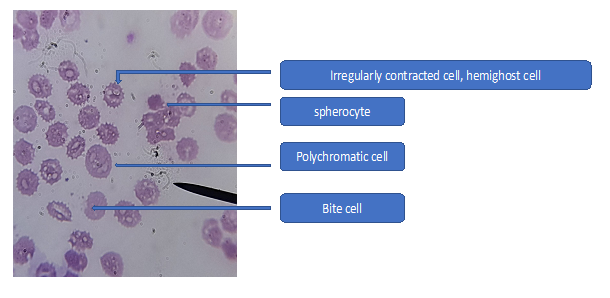
Thorough history taking revealed that he had eaten three Naphthalene Moth ball (25g each) per day for two days (total 6 ball) with the intention to die 5 days ago. He felt nothing till 24 hours after ingestion of 3 balls; then, he took 3 more balls. On the next day, he had vague abdominal pain, nausea and vomiting. He also noticed that his urine color changed to black and oliguria 48 hours later. And his friends took him to hospital. First, his urgent blood tests for full blood count and electrolyte were refused from lab as they thought it was the hemolyzed blood due to wrong storage as the color of plasma was chocolate brown. After discussion with biochemists, they performed the tests. He had severe anaemia (Hb 6.2g%; MCV 93 µm, MCH 31 pg, MCHC 33.4 g/dl) with low PCV (Hct 18.5), neutrophil leucocytosis (Total WBC 22.8 × 109/L, N 67.5%, L 27.4%, M 5.1% and low normal platelet count (179 × 10 9/L). Severe anemia was due to hemolysis as the patient had elevated LDH and retic count. Peripheral blood film examination showed changes in RBC series like numerous hemighost cells, irregularly contracted cells, bite cells, spherocyte and polychromatic cells indicating evidence for oxidative hemolysis. Figure (1) Reticulocyte count was raised 5 times normal (8 %).
He had oliguria and raised serum creatinine nearly three times normal (Urea 110.5 mg/dl; Crearinine 2.82 mg/dl); serum sodium was 131 meq/l, potassium was 4.12 meq/l and, chloride was 94.1 meq/l. Chest radiograph was normal. His nasopharyngeal swab PCR was negative. His ALT was normal- 38.9 U/L (0-40) and AST was five times normal- 196.3 U/L (0-37). Prothrombin time was 17.9 (10-14) and INR was 1.45. Although methemoglobin level in blood, and the discrepancy in arterial oxygen level from ABG and SaO2 percent in pulse oximeter were not measured, he was treated as a case of methemoglobinemia due to suicidal Naphthalene Mothball poisoning.
He was given high concentration oxygen, fluid and electrolytes replacement, N acetyl cystine, ascorbic acid, Ceftriaxone 1G, 8.4% Na HCO3, Dexamethasone, and anti-emetics. Hematologist decided to do urgent exchange transfusion. Nephrologist suggested fluid and electrolytes replacement to combat dehydration which caused acute kidney injury. The pre-procedure workup was done including ABO and Rh typing, antibody screening and matching.
After doing one unit of exchange transfusion, his SaO2 improved at a drastic rate 68% (with oxygen double source with high flow mask) to 70% with CPAP. Then, SaO2 rose to 80% with CPAP after two units of exchange transfusion; clinically, the degree of central cyanosis was much better and patient became more alert. Second exchange transfusion was done 24 hour later; SaO2 improved to 90
Naphthalene mothballs are commonly used in households; it is very uncommon agent of poisoning worldwide. Severe haemolysis from naphthalene poisoning is rare unless there is no G6PD deficiency. Toxic manifestations of naphthalene may be due to enhanced production of free oxygen radicals, resulting in lipid peroxidation and deoxyribonucleic acid damage. The patient did not have G6PD deficiency; however, he developed methemoglobinemia, central cyanosis, acute kidney injury and liver toxicity. Acute kidney injury was owing to naphthalene-induced haemolysis, haemoglobinuria, pigment nephropathy and acute tubular necrosis, requiring renal replacement therapy (Deo et al., 2016).
The patient had all manifestations of naphthalene poisoning which was rarely reported before: drowsiness, confusion, behavioral changes, fits, ocular palsy; neurological involvement; nausea, vomiting and abdominal pain; gastrointestinal involvement, jaundice and raised liver enzymes; hepatic involvement, black urine and acute kidney injury; renal involvement, anemia, intravascular hemolysis and methemoglobinemia; hematological involvement, and, cyanosis, dyspnoea and reduced SaO2; respiratory system involvement.
In this patient, though he had dyspnoea, central cyanosis and low SaO2 on air, there was no clinical clues from examination of heart and lungs: clear lung field on auscultation and chest x-ray, normal blood pressure with normal cardiac examination. This peculiar finding, cyanosis with normal heart and lung, favored the diagnosis of methemoglobinemia. Clinical awareness is important to get early diagnosis and treatment. Thus, it is the good case to learn. The differential diagnosis of methemoglobinemia includes cyanotic congenital heart disease and sulfhemoglobinemia. The potassium cyanide test can distinguish between methemoglobin and sulfhemoglobin. But as the cause was already known, it was not required.
Methemoglobinemia and carbon monoxide poisoning are potentially life-threatening conditions that can present with nonspecific clinical features; thus, exact diagnosis can be down with modern blood gas analyzers which measure carboxyhemoglobin (COHb) and methemoglobin (MetHb) levels. However, both are treatable with antidotes of methylene blue and oxygen (Shelton et al., 2020).
In this case, the technician noticed brownish plasma in clotted blood and informed the clinician for possible causes like over left specimen or intravascular hemolysis. This point was particularly imported in resource limited area where ABG or methemoglobin level was not easily available. Both the treating physician on call, the phlebotomist and lab technician had awareness of the color of plasma on clotted venous blood sample which turned brownish because of severe intravascular hemolysis in this case. Another important clue for methemoglobinemia is that if the color of the arterial blood changes to dark brown with normal PaO2 result. In this patient ABG and Coomb’s test was not done; and, reagent for bilirubin was also in shortage. In this patient, getting early diagnosis was based on team collaboration between medicine on call team and laboratory team, highlighting the importance of intradepartmental collaboration.
Although the concentration of methemoglobin in the blood was not measured, it was above 1.5% if the patient had cyanosis. Methemoglobin is the oxidized form of hemoglobin, which does not bind oxygen and increases the affinity of oxygen for the partially oxidized portion of hemoglobin. Methemoglobinemia is fatal if not treated timely. Ascorbic acid acts as a free radical scavenger and hence may be useful in this situation.
Treatment includes oxygen, fluid therapy and observation. Acute kidney injury may need hemodialysis. Specific antidote, methylene blue, can be beneficial; however, caution must be taken as it can cause paradoxical methemoglobinemia in patients with G6PD deficiency. Vitamin C (ascorbic acid) and N acetyl cystine may be helpful. Exchange transfusion is life-saving in severe poisoning; report on good outcome with exchange transfusion if methemoglobinemia was refractory (Patnaik et al., 2014). The patient made dramatic improvement even after one unit of exchange transfusion. Therapeutic red cell exchange was one of treatment option (Khetarpal & Kotwal, 2018) though some cases may improve with red cell transfusion (Volney et al., 2018).
In COVID-19 era, psycho-social stress may lead to increase incidence of suicide; high index of suspicion on poisoning is important. Naphthalene toxicity is uncommon but fatal. It should be suspected in patients with black urine, nausea, vomiting and abdominal pain, combined with acute hemolytic anemia, methemoglobinemia, and acute kidney injury. Methemoglobinemia is a potentially severe disorder; it should be suspected in acutely dyspnoeic cyanotic patient with apparently normal lungs and heart in physical examination and chest radiograph. Treatment of naphthalene poisoning depends on severity of toxicity; supportive care, fluid therapy, respiratory support, ascorbic acid, methylene blue, and N acetyl cystine. Exchange transfusion is life-saving in severe naphthalene poisoning.




The authors would like to thank the patient for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; Professor Tin Moe Mya for laboratory support, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Our institution does not require ethical approval for reporting cases.
The authors received no financial support for publication of this article.
The informed consent for publication in this article was obtained from patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
