
Review Article | DOI: https://doi.org/10.31579/2768-0487/056
1Department of Medical Laboratory Science, Imo State University, Owerri, Imo State, Nigeria.
2Department of Biochemistry, Government College University, Faisalabad, Pakistan.
*Corresponding Author: Emmanuel Ifeanyi Obeagu, Department of Medical Laboratory Science, Imo State University, Owerri, Imo State, Nigeria.
Citation: Emmanuel I Obeagu, Q Babar. (2021). Covid-19 and Sickle Cell Anemia: Susceptibility and Severity. Journal of Clinical and Laboratory Research. 4(1); DOI:10.31579/2768-0487/056
Copyright: © 2021 Emmanuel Ifeanyi Obeagu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 October 2021 | Accepted: 25 October 2021 | Published: 28 October 2021
Keywords: Covid-19; sickle cell anemia; susceptibility; severity
The 2019 Coronavirus disease (Covid-19) is caused by the SARS-COV2 infection, which has become a global pandemic in a short time. Individuals with sickle cell anemia (SCA) suffer from underlying cardiopulmonary comorbidity and are at risk of serious complications, such as pneumonia, acute thorax syndrome, thrombosis, stroke and multi-organ insufficiency. If Covid-19 raises a high risk of morbidity and mortality in patients with SCA remains unclear. Patients with SCA and Covid-19 can present superimposed clinical features, such as respiratory symptoms with infiltrate, hyperinflammatory state and a higher risk of thromboembolism. In this review, we will discuss the susceptibility and severity of the Covid19 in patients with sickle cell anemia.
Infection of severe acute respiratory syndrome Choronavirus 2 (SARSCOV2) is responsible for 2019 Coronavirus disease ', causes a cytokine storm with damage to the organs, especially lungs in severely affected patients [1] .hemoglobin S (HBS), an abnormal structural variant Hemoglobin, results from the replacement of valid for glutamic acid in the sixth position of the beta chain of globin hemoglobin. This alteration results from the polymerization of low-oxygen saturation hemoglobin, the deformity of red blood cells and microvascular occlusion [2]. About 5% of the population in the world is the vector of hemoglobinopathies, mainly sickle cell anemia (SCA), with a prevalence of 10-45% of the population of sub-Saharan Africa for the gene of sickle cells [3].
The Covid-19 pandemic was born as a concern of greater susceptibility of patients with Covid-19 SCA and a more serious form of the disease. Disease control and prevention centers have SCA classified as one of the conditions that should be considered at increased risk of severe disease of Covid19 infection. Including patients with inflammation SCA (1) of chronic inflammation at greater risk of thrombosis, (2) are immunocompanied causes autoinfect from its surgical spleen or splenectomy and particularly prone to infectious diseases and acute thoracic syndrome (AC) and (3) have comorbidity and The dysfunctions of the secondary organs, there is a concern for the preparation and severity of Covid-19 in these patients [4, 8]. The purpose of this review was to summarize and analyze the susceptibility of patients with Covid-19 and its severity [9].
Challenges faced by SCA patients in C0vid-19 pandemic and its clinical management
The American Hematology Society (AHS) has provided indications for the use of transfusions of red blood cells in patients with sickle cell anemia (SCA) in the configuration of Covid-19, since blood donations have been significantly withdrawn in some regions of the United States [10]. 1t informs us that these lack of blood can require the modification of the transfusion thresholds for common demonstrations, such as anemia, the vascular crisis and priapism, although we recommend the continuation of the transfusion guidelines for acute complications, such as syndrome Stroke or acute thoracic. During this time, hospitals have been forced to carefully manage their blood supplies, since the shortage that persists [11]. Scarcity can request the final points of exchange transfusion loosening (ie, direct to 40% hemoglobin s instead of 30%) or changing to a simple transfusion for patients with SCA. Furthermore, the AABB, the American Red Cross, and of the Blood Centers of America recently published a statement that confirms that blood supply still diminish as the pandemic continues [12].
The Voxelotor is an HBS polymerization inhibitor that increases hemoglobin in individuals with SCA, which therefore improves the ability to transport oxygen [13, 14]. According to a patient relationship with SCA he experienced a significant fall in hemoglobin during hospitalization for Covid19 infection which was successfully treated with Voxelotor instead of additional transfusions [12]. Within two days from the start of the Voxelotor, its HB had increased to 8.0 g / dL. It remained clinically stable and was downloaded to the additional oxygen house (Saturday 98% air O2). By day 10, your HB was 10.3 g / dl. For our knowledge, this is the first report that voxelotor is worn clearly in the context of Covid19 pneumonia in an individual with SCA and respiratory anguish, instead of transfusion. In this case, HB HB and general conditions of the patient quickly improved to treatment, thus avoiding exsanguinotransfusion, reduce the exposure of hospital staff for Coronavirus and RBC units saving; Important in this period of limited blood supply pandemic [12].
The shortage of blood caused by the lack of availability of blood donors due to distance and social containment measures are secondary consequences of the Covid-19 pandemic current [15]. Knowing that patients with SCA have a great need for blood transfusions in the event of a crisis, the use of family donations in emergency situations will undoubtedly increase, with the high risk of transmission of infectious agents, such as HIV, Hepatitis B and the virus. This is because blood tests are often less comprehensive in this type of blood donations due to the African detection context. Although the risk of blood transmission SARS-COV2 has not yet been clearly established, blood donors (volunteers and family) should be examined for SARS-COV2 infection [16]. Unfortunately, in several SSA countries, SARS-COV2 detection remains weak and centralized in national reference laboratories. The decentralization of the detection of SARS-COV2 and the implementation of Point of care in Blood Transfusion and Care Centers SCA could deal with these gaps [17].
Hemoglobinopathy and ferroptosis by Covid-19
A preliminary document on the viral inhibition of the metabolism of the Emer binding to Betachas hemoglobin through surface glycoproteins, was followed by another publication on the denaturation of the induced hemoglobin virus [18]. This alteration of hemoglobin contributes to private polyhedric oxygen syndrome, which is actually generated Covid19 disertetealism SARS-cov2.concropsning iron, Uhsani showed a considerable resemblance between the amino acid sequence distant glycoprotein and glycoprotein protein sarscov2 hepcidin [19]. Coronavirus recognize guest receptors using its tilting proteins to facilitate the passage of forming, so as to engage the cell membrane and enter the host cytoplasm; At Furine and the use of reception proteases, Coronavirus polypeptides can fend its tip, which facilitates cellular entry [20]. Epcidine mimicism found by the virus could be carried out through this complex mechanism [19].
Hepcidin is the main iron metabolism regulator, interacting with Ferroportin to promote iron entry into the cells; In the event of a similar activity to SARS-COV2 Hepcidine, a significant iron disablement can occur, with hyperterriteinemia and, ultimately, ferroptosis [21]. The total of hemoglobinopathy and iron distillation can seriously compromise the ability of erythrocytes to carry out the transport of O2, with hypoxia, while inducing alterations of hyperphitiiny tissues. These events will make patients with SCA more serious, which will lead to death.
Pathophysiology of COVID-19 with resepect to heme metabolism
Whether the original pathologic viral process begins in the lungs, with consequent general anemic hypoxia and iron dysmetabolism, or vice versa hemoglobin/iron dysmetabolism is the leading process that results in multi-organ disease and further hypoxia, is a matter of future research.SARS-CoV-2 infection strictly depends upon the virus interaction with host cell receptors and proteases. Together with the acknowledged ACE2, cyclophyllins, furins and TMPRSS2, CD147 was identified as an additional receptor on erythrocytes and other cells [22]. Actually, CD147 may also represent the virus entry-point in bone marrow immature cells; interestingly, myeloma colonization of bone marrow is mediated by this receptor [23]. Hypoxia seems to upregulate CD147 expression, which might be detrimental in case of viral linkage to these receptors in erythrocytes/erythroblasts. Lastly, another receptor, namely DPP4 (CD26), was found to possibly interact with SARS-CoV-2 spikes and intriguingly this molecule has a proven role in hematopoiesis as well [24]. Hematopoiesis in patients with sickle cell anemia (SCA) is associated with erythroid hyperplasia, reticulocytosis, and ineffective erythropoiesis starting at the immature erythroblast stage in the bone marrow, so COVID-19 will trigger these events upto dangerous level [25].
Hemolysis by COVID-19
A viral interaction with the viral molecule was highlighted with the hemoglobin molecule, through ACE2, CD147, CD26 and other receptors located in erythrocytes and / or precursors of the blood cells. By summarizing the available preliminary data, it was claimed that hemoglobinopathies derives from viral endocytosis, through a link between point proteins and cellular receptors. The viral Orf8 protein and glucoprotein on the surface would be joined to porphyrin, attacking the eme in 1 beta of hemoglobin; SARS-COV2 would induce hemolysis and / or would form a complex with the HEME released, generating a quote dysfunctional hemoglobin, with reducing the transport of oxygen and CO2 [24, 26] interferes .SarScov with hemoglobin in erythrocytes and the level of bone marrow ; In fact, through CD147 and / or CD26, the new SARS-COV 2 attack on erythroblasts of the bone marrow is plausible, since the largest dimension and cytoplasmic / nuclear material would facilitate virus replication and interaction with hemoglobin. Hemolysis is a constant response to CO2, therefore, Covid-19 will make these events more serious and dangerous.
Biochemical events caused by COVID-19
LDH is a reliable hemolysis indicator. The evidence of ClearCut of some retrospective studies of long scales indicates that LDH is exceptionally precisely precisely so that the screen is serious from the mild cases of Covid19. More interesting, LDH figures increase from a double turn to the worst scenarios, decrease in parallel hemoglobin [27]. Similarly, a significant hypofreemia has been reported in patients with ICU, with lower levels of serum iron associated with severe hypoxecyed respiratory failure [28].
The hemoglobin level has gradually decreased can lead to an anemia model similar to a silodiplastic, with myelodisplastic characteristics, according to the acute need to replace dysfunctional erythrocytes. The width of the redble cell distribution (RDW) represents a reliable indicator of myelodisplasses, since it occurs when immature cells occur. Covid19 literature remains repeatedly to a generally increased RDW, which is significantly higher (> 14.5%) in deceased or critical patients [24].
Effect of anemic hypoxia induced by COVID-19 on SCA patients
Hypoxia physiologically, anemic induces general vasodilation, but also pulmonary vasoconstriction, with an increase in fibrin formation in lung microvasculation [29]. In particular, Hepcidine / Ferroportalin's ungroved interaction can also create pulmonary artery hypertension, through the proliferation of soft muscle cells [30]. It progressively affects the integrity / permeability of the cell / alveolarpillary / cellular membrane: inflammation, edema and pulmonary cell necrosis can ultimately complicate the pulmonary condition [31]. As regards the role of iron toxicity in the pathophysiology Covid-19, the epcidinthinmimetical action of SARS-COV2 can induce the internalization / block of ferroportin, which could explain progressive anemia [19].
Hepcidine favors iron entry into cells, negative ferroportin adjustment, which is the key iron conveyor out of the cells; In essence, hepcidine is iron as insulin is glucose and excess can cause hepcidine ferroptosis [24]. Physiologically, Hepcidine is, respectively, upwards or subgulated by high serum or standing iron [32] hepcidinogonists inflammation. Other (IL6, ie), hyperoxyhemia, obesity and diabetes. On the contrary, Hepcidine is antagonized, and Ferroportina is upregulated, from hypoxemia, with HydroxiaInduced (HIF) release factors, and anemia [19].
Increasingly, diabetics`s increased hepcidine peers higher level of glucosylate, dysfunctional, hemoglobin; At the same time, obese and diabetic people OVEREXPRESS The CD147 blood receiver, and this series of biochemical alterations increases the risk of complications [22]. Imitating hepcidine action, sarscov 2 could increase considerably circulating and tissue ferritin (interest liver, spleen, bone marrow and muscles mainly), while the induction of iron shortage in serum and lack of hemoglobin, as a result. Hyperriteinemia gives rise to ferropr, with high oxidative voltage and lipoperoxidation, at the end increases mythophagus with accelerated cellular apoptosis / necrosis [21]. Increasing the rusty that the connected multi-agricultural oxidative stress can precipitate inflammatory / immune replacement (the interleucine storm Socclude) in further stages, most of the critical phases. The laboratory data show a higher relevant hemoglobin level and higher ferritin levels in patients without neonvivens, on survivors [19] .Hyperferriteinemia can induce a series of direct and indirect injuries (through autoimmunity) to the greatest number of organs During the Covid19, as coagulopaths, macrophage activation syndrome, liver injuries such as emochromatosis and other ferrophosisosis syndromes [33].
End Organ Damage in SCA
Major organ failure in sickle cell anemia is the direct consequence of the sickle cell evoked vasculopathy. Major organ failure is first clinically apparent as autosplenectomy, then during childhood presents as cerebral infarction and atrophy, and finally culminates in young adulthood as end stage renal failure (glomerulosclerosis), sickle chronic lung disease, intracranial hemorrhage, retinopathy, disabling leg ulcers, and generalized osteonecrosis. The vascular damage begins years before the overt clinical symptoms are apparent with no pain to act as a signal. Organ damage is progressive and irreversible. The rate of progression is genetically controlled from birth. Except for the management of life-threatening infections that are associated with the non-functioning spleen, disease expression has not been altered by therapy. The focus of future clinical investigations must be the prevention of the vasculopathy and tissue damage which is induced by the sickle red cell [34].Covid-19 results in a cytokine storm with damage to organs, mainly lungs in severely affected patients, these events will make disease more severe [1].
Innate immune dysfunction in SCA
Impairment of the innate immunity is the most well described immune dysfunction in individuals with SCA. Part of the dysfunction has been shown to include increased peripheral blood neutrophil count (granulocytosis), which often accounts for leukocytosis in SCA [35]. However, the increased neutrophils are mostly dysfunctional due to impaired chemotaxis, migration and killing ability [36]. Impairment of the alternate pathway of complement activation through qualitative and quantitative deficiencies of factors B and C3 has also been reported, although this observation has not been consistent between studies [37]. Through this impaired immunity SCA patients become more prone to COVID-19 with high mortality rate [38].
Spleen and Innate Immune Dysfunction in SCA
Most of the innate immune changes in SCA are a manifestation of reduced splenic function (hyposplenism), which can occur in the context of atrophied or enlarged spleen [39]. This loss of splenic function in SCA has been attributed primarily to repeated sickling in the spleen with eventual destruction of the architecture and function of the spleen[40]. The BABY HUG study demonstrated that loss of splenic function starts early on during infancy in individuals with SCA [41]. Splenic filtration function is often compromised as well in this setting, leading to decreased ability for trapping and removing bacteria from the circulation [42]. Overall, SCA patients with hyposplenism show reduced opsonophagocytic activity and ability to clear bacteria from the blood [36]. The loss of splenic function and ensuing reduction in opsonophagocytic activity is the most well accepted cause for the increased risk of infection with encapsulated bacteria in SCA [39]. In the absence of interventions, including timely vaccinations and proper coverage with prophylactic antibiotics, immune impairment due to hyposplenism in SCA can results in severe and life-threatening infections [39, 43]. According to a study dynamic immune landscape of innate and adaptive immune cells in disease progression and absolute changes of lymphocyte and myeloid cells in severe versus mild cases or healthy controls was observed in COVID-19 patients [38].
Adaptive immune dysfunction in SCA
High rates of alloimmunization, connective tissue diseases and transplant rejections, as well as incidences of aberrant vaccine reactivity, have bought to surface adaptive immune abnormalities in SCA [44, 45]. Currently, however, little has been done to characterize T and B lymphocyte phenotype, function and contribution to chronic inflammatory diseases in SCA. Limited studies done indicate that abnormalities in both T and B cells occur in SCA [46]. These abnormalities may be induced by SCA disease itself, or may arise as a result of complications of its treatment with repeated blood transfusions. A focus on adaptive immune abnormalities in SCA will refresh our outlook towards SCA as an immune disease, and may open up novel research on immunity in SCA as well as lead to development of newer approaches in combating the immune derangement, inflammatory diseases and improving vaccine outcomes in individuals with SCA.One of the most serious complications of COVID-19 is the development of uncontrolled production of cytokines that poses a major factor contributing to COVID-19 morbidity and mortality which will complicate condition of SCA patients [47].
Transfusion-Induced Changes in T and B Lymphocytes
Patients with SCA who are recipients of multiple blood transfusions for the treatment of severe anemia or primary stroke prevention have an additional risk for immune derangements [48, 49]. These derangements have been observed in the presence or absence of alloimmunization. Regardless of alloimunization status, patients with SCA recipients of multiple blood transfusions were found to have increased proportion of central memory CD4+ T cells, reduced CD4+ helper : CD8+ suppressor T cell ratios and impaired natural killer (NK) cell activity [50, 51]. The reduction of CD4+ helper : CD8+ suppressor T cell ratio likely represents normal immune response to multiple blood transfusions as it has also been observed in individuals with other blood disorders necessitating repeated blood transfusions [50, 52]. The immunomodulation brought about by repeated blood transfusions was linked to reduced responsiveness of children with SCA to H1N1 vaccine, and is hypothesized to contribute to increased infection risk [53]. Repeated blood transfusions can result in alloimmunization in individuals with SCA. In this era of pandemic COVID-19 plays crucial role in severity of disease. Due to hyper activation of immune system plasma transplant in these patients will lead to severe immunomodulation changes which leads to death [54, 55].
Immune activation in SCA
SCA is increasingly recognized as a chronic inflammatory disease characterized by considerable immune activation [56, 57]. Immune activation is thought to contribute to the pathogenesis of alloimmunization, transplant rejection and other inflammatory diseases in individuals with SCA. Due to increase immune response inflammatory profile is increased which causes cytokine storm in COVID-19 patients leads to worsening of disease.
The Spectrum and Sequelae of Immune Activation in SCA
The scope of immune activation in SCA is broad, involving cellular as well as humoral mechanisms. Besides neutrophil, monocyte, natural killer cell, platelet, mast cell and endothelial cell activation, evidence of lymphocyte activation has also been reported in SCA [58-60]. Markers of lymphocyte activation reported in SCA include increased number of memory T cells, increased CD4+ and CD8+ T cell expression of Ki67and increased Treg expression of CTLA-4[61]. Augmentation of the pro-inflammatory Th17 response has also been observed in SCA [62], more so among recipients of multiple blood transfusions [63]. Furthermore, patients with SCA have increased levels of C-reactive proteinand pro-inflammatory cytokines IL-6 and TNF-α, and increased signaling through the pro-inflammatory Toll-like receptor 4, 7 and 8 (TLR4, TLR7 and TLR8) as well as through the inflammasome complex pathways [62, 64, 65].COVID-19 makes these all events more worse due to similar biochemical profile in diseased patients [66].
SCA susceptibility and severity in COVID-19
SCA patients are immunocompromised with multiple comorbidities and a hypercoagulation state. Older patients with pre-existing multiple organ damage are at higher risk of morbidity and mortality from COVID-19, and hemoglobin genotype, or gender seems to be not associated to COVID-19 disease severity [67]. On the other hand, COVID-19 is associated with cytokine storm and hypercoagulability. SCA as well as older age and comorbid diseases such as cardiovascular disease, chronic lung disease, diabetes, or cancer, have been considered as risk factors related to fatal complication among patient infected by SARS-CoV-2 [5]. This is because of the non-functioning of the spleen compromising the immune system, systemic vasculopathy, and a high risk of thrombosis often observed in SCA[68]. Furthermore, the experience of influenza A H1N1 pandemic in 2009 highlighted increased susceptibility of children with SCA to severe complications of a respiratory virus, with an up to 50% increase in hospitalization for this patient population [69]. Thus, with no vaccine and no proven effective treatment, the COVID-19 pandemic would, therefore, became an additional concern in patients with SCA, in addition to malaria, bacterial pneumonia, vaso-occlusive crisis (VOC), and renal disease. However, there is still a gap in the mechanism by which SCA is at risk of fatal complication of the COVID-19. Although the COVID-19 is associated with reduced cellular oxygenation, pneumonia and acute respiratory distress syndrome in severe cases, it is also unclear whether the SARS-CoV-2 pandemic will lead to increase the risk for SCA patients to developing VOC as well as acute chest syndrome (ACS).
Recent case reports have curiously shown that the clinical course of the SARS-Cov-2 infection was mild without fatal complication [70, 71]. Indeed, these studies showed that with different genotypes of SCA and a history of respiratory complications, such as ACS, asthma or pulmonary embolism, no patient required admission to the intensive care unit, mechanical ventilation or non-invasive ventilation. However, in the majority of cases, these patients required blood transfusion. Although evidence with other viral infections suggests that CoV-2-SARS can also cause ACS, the inflammatory, haemolytic and chronic anaemic state observed in the SCA patients could have a favourable influence on the clinical course of the SARS-Cov-2 infection [69, 72]. In fact, chronic haemolysis is responsible for the release of heme which contributes, via its interaction with TLR4 (Toll-like receptor 4), to a proinflammatory and procoagulant state pre-existing in SCA patients [73]. Thus, abnormally high plasma values of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α have been reported in SCA patients at steady state [73]. Similarly, it was reported that the SARS-CoV S protein induces direct up-regulation of IL-1, IL-6, and TNF-α [74]. This similar pathophysiology could explain the low impact of the cytokine storm, reported as a complicating mechanism of COVID-19, in SCA patients whose bodies are already accustomed to a chronic inflammatory state.
In any case, SCA patients are at high risk of bacterial infections. There is, therefore, a risk of missing the diagnosis of a severe bacterial infection, and mistakenly attributing symptoms to SARS-CoV-2 infection, which could delay access to life-saving antibiotics in SCA patients [75]. ErfanNur et al report that COVID-19 may trigger VOC without the presence of COVID-19 flu-like symptoms and an ACS may develop without the typical pulmonary complications observed with COVID-19. This confusion could also result in delayed diagnosis of CoV-2-SARS infection with the risk of causing inadequate management, especially in areas where SARS-CoV-2 testing stills lacking as in Africa[17].
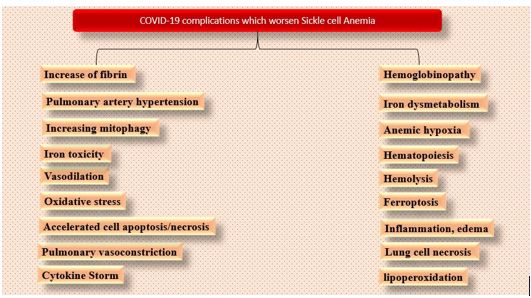
Finally, there remain fundamental gaps in knowledge of the SCA including the insufficient understanding of the missing heritability of HbF and the mechanisms controlling switching of foetal to adult haemoglobin, and incomplete identification of disease modifiers to enable the development of comprehensive prediction models for patient stratification and targeted interventions [76]. Moreover, Africans remain to have poor knowledge and a mythical misconception of SCA[77]. Various events are summarized in figure 1 which are caused by COVID-19 and finally leads to complication in SCA.
It was shown that Covid-19 in pregnant women showed some cases of severe maternal morbidity and perinatal deaths, although the majority of the cases had a good outcome [78]. On the other hand, another paper showed that severe pulmonary complications are common in SCA pregnant women [79]. In our report, however, the patient presented with respiratory symptoms and typical radiographic images of Covid-19, raising the hypothesis that the novel coronavirus infection was the trigger of the respiratory manifestation. Despite her previous history of pulmonary comorbidities and the current pregnancy, her clinical evolution was very favorable. As far as we know, not one case of ACS by the novel coronavirus in pregnant SCA patients was found in the literature [80]. To enhance the knowledge of the scientific community in this field, we believe that physicians should be encouraged to access and submit their experience in data platforms such as ‘Secure SCA Registry', coordinated by Panepinto et al., at the Medical College of Wisconsin, USA [80].
In general, the laboratory results of Covid19, such as hyperferritentemia, low hemoglobin, low sidemia, thrombocytopenia and anison, with high rdw figures, lactate and LDH increase, are reasonably compatible with erythrocyte / bone bone marrow distillation [81] the bodies Experimental are directed directly, or indirectly directed by SARSCOV2 and Multiple Patecanisms have been described, both of the immune / inflammatory type and are connected to hypoxia and ferroposis; TROMBOEMBOLIA seems to play a significant role in the following phases as well. In general, the pathophysiological paths seem to overcome in many cases; However, hemoglobinopathies and iron designer can induce a series of biological events, which are objectively linked to clinical syndromes highlighted during Covid19: i) decrease in hemoglobin appointment that works; ii) Iron increase in cells / tissues; iii) release of free circulation hem toxic; iv) hypoxemia and systemic hypoxia; v) reduction not; Vi) activation of coagulation; vii) ferroposis with oxidative stress and lipoperoxidation; Viii) mitochondria degeneration.sca is increasingly recognized as a chronic inflammatory disease characterized by considerable immune activation [56, 57]. It is believed to contribute immune activation to the pathogenesis of allimmunization, rejection of transplants and other inflammatory diseases in individuals with SCA. Due to increase the inflammatory profile of the immune response, it increases, what causes cytokine storm in patients with Covid-19 leads to the deterioration of the disease. Therefore, patients suffering from sickle cell anemia are more sensitive and prone to Covid-19 with additional complications.
With the current lack of tests on the susceptibility of patients with Covid-19 and a worse prognosis, there is therefore an urgent need for a global, intersectoral and interdisciplinary approach to develop evidence and anticipate interventions in the SCA. This requires great financial resources and proactive interventions. Financial assistance in this period of health crisis, including donors, non-governmental organizations and governments, should also address the problem of SCA and Covid-19 in SCA. The interventions should focus on the detection of the masses for SCA and Covid19, the prevention of vaccination of bacterial infections in patients with SCA, the availability of prophylaxis of penicillin V and hydroxyurea, capacity and construction of transfusion centers and assistance centers SCA, and formation of Healthcare professionals. The patient's insulation and administration centers with Covid19 must implement a specific protocol for clinical, psychosocial and nutritional management of patients with SCA. Communication must be adapted to the local context to avoid stigma and discrimination.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
