
Case Report | DOI: https://doi.org/10.31579/2690-8808/158
1 West Virginia University School of Medicine, Department of Cardiovascular and Thoracic Surgery
2 West Virginia University Health Sciences, Informed Consent: See appendix (scan of patient’s consent form)
*Corresponding Author: Fazil Abbas, West Virginia University School of Medicine, Department of Cardiovascular and Thoracic Surgery.
Citation: Elwin Tham, Fazil Abbas, Ghulam Abbas. (2023), Costal cartilage disruption and thoracoabdominal hernia: Presentation and Management. J, Clinical Case Reports and Studies, 4(1); DOI:10.31579/2690-8808/158
Copyright: © 2023 Fazil Abbas, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 November 2022 | Accepted: 30 December 2022 | Published: 03 February 2023
Keywords: costal cartilage disruption; diaphragmatic hernia; trauma; thoracoabdominal hernia
Costal Cartilage disruption after forceful coughing in obese males is an uncommon occurrence. Rarely it is associated with diaphragmatic disruptions leading to herniation of the abdominal contents into the chest. A successful outcome requires correcting both elements, namely, repairing the diaphragmatic defect along with the reduction of hernia and repairing the costal cartilage fracture. In this manuscript, we present a case where the diaphragmatic hernia was repaired, but the costal cartilage disruption was missed resulting in a reoccurrence of the diaphragmatic hernia.
Costal-cartilage disruptions occur because of high-energy injuries, blunt trauma or spontaneously from forceful coughing. These disruptions present with pain and dyspnea and may be associated with thoracoabdominal/abdominal wall hernias [1-7]. Anecdotally, among the non-traumatic group, patients are commonly centrally obese and present with pain associated with a tearing sensation after a forceful cough.
Commonly delayed or missed in diagnosis secondary to normal or distracting radiological findings, the mainstay of diagnosis remains in history-taking and physical-exam [4]. Management typically includes pain control and rest with limited data on surgical management [5].
A 63-year-old man who presented to an outside hospital 3 weeks ago for left upper abdominal pain and dyspnea was found to have a diaphragmatic hernia from forceful coughing on CT scan but the fractured left costal cartilage was missed. The diaphragmatic hernia was repaired with laparoscopic suturing of the diaphragm.
Weeks later, he experienced recurrent symptoms with sinus-tachycardia, increasing oxygen requirements and was transferred to our institution for further investigation. Physical exam revealed a left subcostal bulge along with fractured left costal cartilage between the 8th and 9th rib. A CT scan with oral contrast (Figure 1) revealed a large left recurrent diaphragmatic hernia with mesenteric and small bowel extension through the hernia defect and confirmed the fractured left costal cartilage.
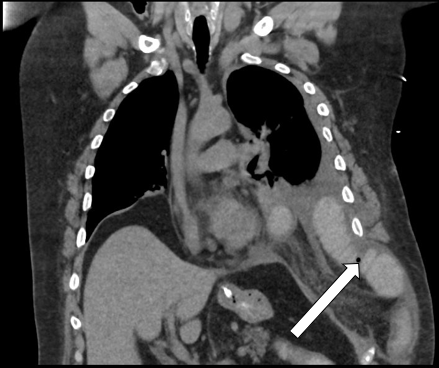
Figure 1: Coronal view of CT scan of patient with Thoracoabdominal hernia
The patient was brought to the operating room for repair. The repair included repair of: [1] diaphragmatic defect with mesh reinforcement, [2] costal-cartilage disruption
Costal-cartilage disruption may occur in association with thoracoabdominal hernias which may involve the triad of intercostal hernia or chest wall defect, abdominal wall hernia, and diaphragmatic hernia, though up to 25-66% of these hernias do not involve of all three structures (8). We identified three main radiological features of thoracoabdominal hernia.
One, thoracoabdominal hernia involves the disruption of inner muscle layers which include the transversus abdominis, intercostal muscles, and often the internal oblique. A clear distinction between thoracoabdominal hernias and pseudo-hernias with preoperative investigation is essential as these entities present identically though pseudo-hernias are treated symptomatically [9].
Two, superficial muscle layers such as the latissimus dorsi and external oblique muscles are typically preserved in Thoracoabdominal hernia [8,9]. Careful identification of the involved defects is essential to allow preoperative planning of the optimal operative approach and correct plane for mesh placement [10,11].
Three, thoracoabdominal hernia characteristically involve costal-cartilage disruption with defects varying from inferior rib displacement by hernia contents and unopposed traction of the abdominal muscle, to rib fractures [8,9]. Costal-margin-rupture is also commonly identified and can be associated with the hernia or present with rib pain as in slipped rib syndrome as described by Hansen et al. [12].
Approach to repair
In our case, we proceeded with a left lower lateral thoracotomy approach. Intraoperatively, we identified a fracture of the left costal cartilage between the eighth and the ninth ribs with complete separation of the ribs and a tear in the diaphragm through which a small bowel loop herniated into the pleural space.
Repair of Diaphragmatic defect
The diaphragmatic defect measured about 5 cm after reduction of the hernia contents back into the intra-abdominal space. This was easily approximated, repaired primarily with #2 Ethibond sutures and reinforced with Gore-Tex mesh using interrupted #2 Ethibond sutures.
In a retrospective study [13] of primary thoracoabdominal hernia, majority of the diaphragmatic defects (n=13) were repaired primarily with permanent sutures. The role of mesh reinforcement in the repair of diaphragmatic hernias remains an ongoing debate although the use of mesh is particularly useful for associated abdominal and/or larger defects [8, 13].
Repair of Costal cartilage disruption
For the repair of the costal cartilage disruption, the key lies in the stabilization and approximation of the ribs to repair the intercostal defect.
One study described 12 repairs of Thoracoabdominal hernia in which the chest wall defect was repaired with a combination of sternal wire sternal wire, cables or absorbable suture and rib-plating [8].
In our case, mobilization of the ninth rib allowed optimal approximation of the eighth and ninth ribs, after which, we placed interrupted #2 FiberWire sutures through the costal cartilage and around the rib to approximate the ribs. A mesh is needed to cover the gap if the ribs fail to approximate. Similarly, a mesh is used to repair the abdominal wall defect if present.
Costal cartilage disruptions may occur in association with thoracoabdominal/abdominal hernias. Extensive investigation is essential for preoperative planning to achieve durable repair and reconstruction of thoracoabdominal wall. Further research into long-term outcomes is required for recommending surgical intervention to patients with such entities.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
