
Research Article | DOI: https://doi.org/10.31579/2692-9759/083
1 King Fahad cardiac Centre, College of Medicine, King Saud University Medical City, Saudi Arabia.
2 AlFaisal University, College of Medicine, Riyadh, Saudi Arabia.
3 Universiti Sains Malaysia (USM), Malaysia.
*Corresponding Author: heart failure outcome; troponin leak; ICD therapy; ICD shocks
Citation: Fakhr Z. AlAyoubi, Hayajneh A., Tariq A. Alam, Kazi N. Asfina, Siti M.S. Ghadzi, et al, (2023) Cost of Heart Failure in-patient in Saudi Arabia: Role of Heart Failure Multidisciplinary Program. Cardiology Research and Reports. 5(1); DOI:10.31579/2692-9759/083
Copyright: © 2023 Fakhr Z. AlAyoubi, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 December 2022 | Accepted: 30 December 2022 | Published: 09 January 2023
Keywords: heart failure outcome; troponin leak; ICD therapy; ICD shocks
Background: Globally, the prevalence of heart failure (HF) is rising in many countries, same as in Saudi Arabia but the economic burden of direct and indirect costs for HF hospitalization and re-hospitalization are not well studied in Saudi Arabia. The aim of this study was to assess the efficiency of the newly established multidisciplinary HF team at King Saud University Medical City (KSUMC) in reducing the costs of each HF patient per year.
Material & Methods: A non-interventional retrospective prevalence-based single-center King Fahad Cardiac Centre (KFCC) study was conducted with all the HF in-patients from January 2014 to December 2019 at KSUMC.
Results: The study included a total of 943 patients, where 531 were male, a study period of 6 years. The mean age was 61.65 ± 1.9 year, the median length of stay (LOS) was 11.6 days (compared to the global average which is 4-5 days), BMI was 29.9, the median NT-proBNP was 6015.3 pg/ml and NYHA was 2.9. Hypertension (HTN), Diabetes (DM), dyslipidemia and coronary artery disease (CAD) were the most commonly reported comorbidities in the study period. As per the recent study for Middle East (ME) countries (Egypt, Saudi Arabia and UAE), the average cost per year per patient was 8137 $. The patient’s admission and readmission cost, which were the direct costs, was the major cost driver ranging from 25% to 56% of total cost, therefore, the average admission cost was 30% of total cost. Hence the admission cost for each patient per year was 8137 $ x 30% = 2441 $. The readmission cost in 2014 was $ 90317 and in 2015 was $ 19528, which was represented a drop of 78.4%. In 2016, it was $ 17087 showing a drop of 81%. In 2017, it was 86.5% and 83.9% respectively in 2018 and 2019. The indirect medical costs were estimated based on a human capital approach.
Conclusions: Our HF program has a role to keep up the positive outcomes by reducing the HF readmission, hence reduce the direct and indirect costs. We were able to reduce the re-hospitalization for NYHA Class-2 by managing in outpatient clinics and therefore reducing the total cost of HF per year. We can improve the research quality by adding higher numbers of patients with more geographical representation and estimation of other costs, such as indirect costs may be needed in future studies.
Heart failure (HF) is a clinical syndrome with symptoms and/or signs caused by a structural and/or functional cardiac abnormality and supported by elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion [1]. HF is a global health problem that is associated with poor quality of life and an ever-rising healthcare cost ($24,383 per patient) [2]. Primary goals of HF therapy are to slow down progression of symptoms, improve patient’s quality of life, prolong survival, and decrease cost [3].
The New York Heart Association (NYHA) functional classification by far, is the most used classification system which places heart failure patients in one of four categories based on how much they are limited during physical activity [4].
Despite these goals, morbidity and mortality remain high in managing heart failure [5, 6]. It accounts for 5
2.1 Design and Population:
We conducted a non-interventional retrospective prevalence-based single-centre study at KSUMC to assess the effectiveness of creating multidisciplinary team based (certified HF cardiologists, qualified HF nurses, clinical cardiac pharmacists, dietitians, and health educators) HF program for patients with HF in January 2015 at King Fahd Cardiac Centre (KFCC) Riyadh, Saudi Arabia under the umbrella of KSUMC. This HF program was involved in both outpatient services as well as inpatient. Our study was for the inpatient cost of care. The study population was from January 2014 to December 2019.This was assisted by establishing a HF database, which reflects the comparison of the annual cost of each HF hospitalized patient before and after the initiation of the program. Based on the latest HF guidelines, the diagnosis of heart failure and the standard variables definitions were in accordance with the European Society of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with heart failure [33, 34]. The cost was compared with a public sector perspective (e.g Ministry of Health). We obtained the Saudi Arabian GDP per capita for the year 2020 from the World Bank database and used it as an index for evaluating indirect costs [35]. The total cost was calculated in US dollars (1 USD= 3.75 Saudi riyals).
Direct costs for our study were involved with general physician and specialist physician services, non-physician personnel services, emergency services, hospitalization without surgical services (acute and chronic diseases), day clinic services, diagnostic services (including laboratory, imaging and genetic counseling clinic), health services as non-official person (who are ineligible approved by the Ministry of Health) and the indirect costs covered patient transportation expenses to receive health services along with the family, patient and the family housing costs (other than admission), expenses related to the patient’s temporary and permanent disability due to illness, for the foods, communication technologies (telephone, Internet, etc.) and related to the patient’s changing jobs were estimated based on human capital approach for Saudi Arabia.[36]
2.2 Data Collection:
Secondary data of all patients included in this study were collected by constructing a paper-based case record form (CRF) which were extracted using our Electronic Medical Records (EMR) for all consecutive KSUMC hospitalized acute on top of chronic and de novo (newly diagnosed) HF patients aged more than 18 years for a study period of 6 years (2014-2019), to capture the entire spectrum of medical care for heart failure patients. [37] As per the inclusion criteria, we filtered the eligible patients' Medical Record Numbers (MRN) after getting the Institutional Review Board (IRB) approval and completed the designated CRF of the study. It is a retrospective, prevalence-based, observational single-centre study and the study proposal was gone through expedited review by the Ethical Committee of KSUMC (IRB # E-16 1981).
The following information were captured for each patient in this study:
2.2.1 Demographics: age in years, gender, duration of admissions and readmission.
2.2.3 Direct Cost: We have used the information from our recent study from KSUMC in 2018, for the total cost of each HF hospitalized patient and then calculated the direct cost which were general physician and specialist physician services, non-physician personnel services, emergency services, hospitalization without surgical services (acute and chronic diseases), day clinic services, diagnostic services (including laboratory, imaging and genetic counseling clinic) for all HF re-hospitalized patients before and after the establishment of the HF program. Then we have compared each HF hospitalized patient’s direct cost per year for the period of 5 years from 2014 [32].
2.2.4 Checklist for the cost calculation: The checklist was developed based on recommendations of the HF guidelines and included the use of angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs), ß-blockers, and influenza and pneumococcal immunizations [38]. It also had a section for education, including medications, which was carried specifically by the clinical pharmacist. We assessed the effect of the checklist on adherence to such a regimen in terms of 30-day readmission rates.
2.3 Statistical Methods and Data Analysis: We performed descriptive statistics, including the calculation of means, standard (SD), and frequencies. Additionally, we used inferential statistics as needed, including t-test and the analysis of variance (ANOVA) tests to compare the cost of HF groups. We also performed a Linear regression analysis to analyze the association between the estimated costs and different variables, such as age, gender, EF, and comorbidities. All p-values less than 0.05 were considered statistically significant. We conducted statistical analyses using the Statistical Package for the Social Sciences (SPSS) version 23 (SPSS Inc., Chicago, IL, USA).
The study included a total of 943 patients covering the period from January 2014 to December 2019. The total number of male patients was 531 as well as total number of female was 412 for the entire study period of 6 years. The mean age was 61.65 ± 1.9 years, and the average length of stay (LOS) was 11.6 days (compared to Global average which is 4-5 days). The average BMI was 29.9. The age group, LOS and BMI has been near about constant throughout these 5 years.
The table 1 showed that, Hypertension (HTN), Diabetes (DM), Dyslipidaemia and Coronary Artery Disease (CAD) were the most reported comorbidities in the study period. We were unable to collect some variables retrospectively for 2014, before the built up of HF program. Through the HF program, we were able to capture hypothyroidism, anaemia, coronary artery diseases (CAD) and DM: Diabetes Mellites, dyslipidaemia accurately, which were managed by the efficient teamwork in the program and eventually the re-admission was reduced for these associated comorbidities, shown in table 1. As per the NYHA classification, average class was 2.9. In 2014 and 2015, the patients were admitted and re-admitted with average NYHA class 2.3, but after the fully establishment of the program, we were able to manage such group in the outpatient clinic.

Abbreviation: DM: Diabetes Mellites, HTN: Hypertension, COPD: Chronic Obstructive Pulmonary Disease, CAD: Coronary Artery Disease,
Table 1: Patient’s disease characteristics.
As per the recent study for Middle East (ME) countries i.e., Egypt, Saudi Arabia and UAE, the average cost per year per patient was 8137 $. The patient’s admission and readmission cost, which is the direct cost, is the major cost driver ranging from 25% to 56% of total cost, therefore, the average admission cost was 30% of total cost. Hence the admission cost for each patient per year was 8137 $ x 30% = 2441 $.
Figure 1 below demonstrates that for the readmission of 37 patients in 2014, the total cost was $ 90317 using the Middle East and North America (MENA) cost and for 8 readmissions in 2015, total cost was $ 19528, representing a drop of 78.4%. In 2016, for 7 readmissions, the total cost was $ 17087 showing a drop of 81%. In 2017, it was 86.5% for 5 readmissions despite having the highest average comorbidities but lowest number of readmissions, in comparison of other years in our study. Finally, there was 6 readmissions with the total cost of $ 14646, representing a drop of 83.9%, maintained for 2018 and 2019 successively.
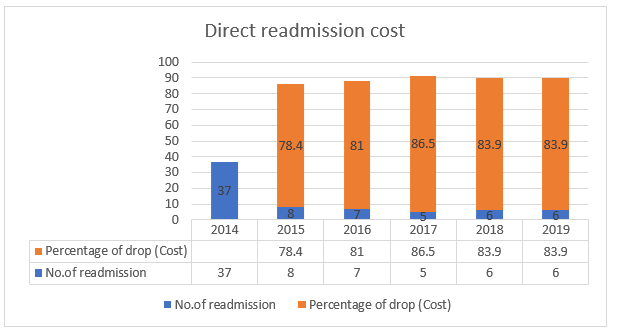
Figure 1: Direct readmission cost.
Table 2 shown the laboratory values for our study period. The average values of all the parameters were constant throughout the journey of our study, but we were able reduce the readmission of the HF patients. This represents a steady outcome after the establishment of the multidisciplinary team.
| Years | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Average |
| Hb | 12 | 12.6 | 11.9 | 11.8 | 12 | 12.1 | 12.1 |
| FERRITIN | 347.2 | 187.2 | 191.9 | 202.7 | 202.7 | 187.4 | 219.9 |
| URIC ACID | 458.7 | 515.5 | 482.9 | 487.9 | 514.1 | 491.5 | 491.8 |
| TSH | 4.8 | 4.8 | 3.6 | 4.1 | 4.9 | 2.8 | 4.2 |
| T4 FREE | 16.6 | 16.9 | 17.3 | 16.8 | 17.2 | 16.7 | 16.9 |
| PRO-BNP | 5943.3 | 6182.9 | 6384.7 | 5742.3 | 6486.5 | 5352.3 | 6015.3 |
| Na + | 133 | 133.1 | 133.5 | 135.6 | 135.5 | 135.9 | 134.4 |
| K+ | 4.8 | 4.2 | 4.2 | 4.2 | 5.7 | 5.1 | 4.7 |
| UREA | 13.9 | 12 | 13.6 | 15.2 | 17.9 | 17.6 | 15.0 |
| CREATININE | 52 | 126 | 140.2 | 141.2 | 157.9 | 156.6 | 129.0 |
| Mg+ | no data | 1.3 | 0.8 | 0.9 | 0.9 | 0.9 | 1.0 |
| SBP | no data | 113.9 | 110.6 | 111.4 | 110.9 | 113.7 | 112.1 |
| DBP | no data | 65.5 | 62.3 | 62.7 | 62.6 | 64 | 63.4 |
| HR | no data | 76.4 | 75 | 76.3 | 73.9 | 78.8 | 76.1 |
Table 2: Laboratory findings.
The estimation of the economic impact of HF on society is a great tool that provides valuable information about the use of health resources and the country’s expenditure on this disease. This will help decision makers in prioritizing healthcare policies, implementing interventions, and efficiently allocating the available health resources [38, 39].
Inpatient HF expenditure was subdivided for direct and indirect medical costs.
We aimed to develop an efficient multidisciplinary team to improve the quality of life for HF patients which eventually will increase the cost-effectiveness in heart failure. Outcome of the HF improved by adherence to the guideline-directed medical therapy (GDMT). The GDMT is for heart failure with reduced ejection fraction (HFrEF) and is recommended prior to primary prevention implantable cardiac defibrillator (ICD) placement [40]. The GDMT as shown in the appendages, were invented by our hard-working team. We had created our own HF assessment checklists to assess accurately and properly by the physicians and nurse’s specialist, titrating of medications by experienced clinical pharmacist through the medication checklist and introducing seasonal jabs checklist, echo instruction, smoking cessation counseling and dietary counseling in three separate checklists for adjusting the outcome, checklists were a helpful tool for gathering the information needed for KSUMC heart failure patients data. . We had constructed a walk-in clinic for closely monitoring patients within 2-3 weeks of discharging from the outpatient clinic.
In 2017, the patient numbers increased with all the comorbidities but by strictly adhering to our own GDMT through the efficient HF program, we were able to maintain homogenous stability.
The role of the HF Consultant from this multidisciplinary team was, to diagnose the patient and carefully evaluate the patient’s symptoms, be alert and ask for common verbal descriptors of NYHA by using his experience to classify which class of the patient fits, assess Jugular venous pressure (JVP), echocardiogram, laboratory work (for example; Brain Natriuretic Peptide (BNP) and label the patient as HF with NYHA classification.
The HF Clinical Pharmacist from the team played the most important role in both aspects of pharmacological and non-pharmacological management. They ensured the initiation of ACEI/ ARBs, BBs, and others to all HF patients and achieved the targeted therapy dose. They gave proper education and counseling about contraindications, intolerance, or other reasons to HF team in collaboration with the patients and caregivers for not utilizing proper therapies [41]. They prevent, detect, and resolves medication-related problems and provide comprehensive, and timely responses to drug information requests as well as they document the source of scientifically valid information and advice regarding the safe, appropriate, and cost-effective use of medicines and develop, review, and evaluates clinical guidelines for medications used in stated management protocol with GDMTs according to evidence, compliance with prescription during hospitalization and delivery of adequate patient education regarding medication use and follow-up, thereby improving the outcome of patients with HF [42,43].
During the transition of patients from the setting of inpatient to outpatient and being assessed by different caregivers, pharmacists play a positive role by influencing medical reconciliation and patients’ education, which will result in assuring consistency in management and reducing medication errors. Utilizing GDMT, this will decrease emergency department visits, hospitalizations for HF, and all-cause readmissions for patients with HF. We were able to evaluate patients’ adherence to medications by controlling polypharmacy problems in chronically ill patients and appointments throughout the program [44-46].
The nurses play an important role by establishing a link between the patient and the multidisciplinary team for optimal care. They educate patients on the meaning of HF and provide several strategic plans and counseling. They ensure that the patients are closely following their discharge instructions and emphasize adhering to GDMT while also focusing on timely follow up. Having nurse specialists in the multidisciplinary team increases the proper use of evidence-based HF therapies [47-48].
Figure 2 shows the KPIs checklists, for example, discharge patient on ACEi or ARB /Angiotensin receptor neprilysin inhibitor, discharge patient on beta blockers, as well as instructions upon discharge, etc. [49-50-51].


Figure 2: Heart Failure checklist
This study aimed to estimate the cost of HF treatment for the hospitalized patients using real world data. However, the study has some limitations. The study is limited to the tertiary care center which might be more enthusiastic about adhering to guidelines and evidence-based practice and this may explain the high prescription rate of medication at baseline. There is also limited geographic representation compared with other countries. The observational nature of the study with the inherent selection bias was another weakness. Observational studies are especially prone to its many forms, mainly due to the investigator's lack of control over the study. Selection bias may result when a study fails to select a representative sample from the population of interest, limiting the applicability of the study's results. In the estimation of direct costs, the study focused on direct medical costs and did not include indirect costs, such as that of transportation and housing for patients visiting from outside Riyadh. Although the study represents a large public healthcare institution in Riyadh, it does not account for those in other large institutions at a national level and from the private sector. Due to pandemic crisis caused by Covid-19, data was collected for 2020 but due to high emergency extensive care from intensive care Unit (ICU) admission and use of the resources unexpectedly, was not included to contaminate the data.
Our program has a role to keep up the positive outcomes by reducing the HF readmission, hence reduce the direct and indirect cost. We were able to do reduce the re-hospitalization for NYHA class II by managing the group in outpatient clinics and therefore reducing the total cost of HF per year after establishing and succeeding the goal of HF program.
We can improve the research quality by adding higher numbers of patients with more geographical representation and estimation of other costs, such as indirect costs may be needed in future studies.
Funding: This research received no external funding.
Institutional Review Board Statement: This study was approved by the Institutional Review Board (IRB) Committees at KSUMC (IRB # E-16 1981).
Informed Consent Statement: Informed consent was not obtained from the subjects as per the IRB protocol of the retrospective observational study.
Data Availability Statement: Data sharing not applicable.
Acknowledgments: The authors would like to extend their sincere appreciation to the
Deanship of Scientific Research, King Saud University (Riyadh, Saudi Arabia).
Conflicts of Interest: The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
