
Research Article | DOI: https://doi.org/10.31579/2641-0419/029
1 Cardiology Department, Alshifa Hospital, Gaza, and Palestine.
2 Alshifa Hospital, Radiology Department, Gaza, Palestine
*Corresponding Author: Mohammed Habib, Cardiology Department, Alshifa Hospital, Gaza, and Palestine.
Citation: Elshenat Majed., Balosha M., Habib M. (2019) Correlation of Coronary Artery Calcium and Invasive Coronary Angiographically in Patients with Atypical Angina Pectoris (CACICA - Trial). J Clinical Cardiology and Cardiovascular Interventions, 2(4); DOI:10.31579/2641-0419/029
Copyright: © 2019 Mohammed Habib. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 October 2019 | Accepted: 25 November 2019 | Published: 29 November 2019
Keywords: myocardial infarction; primary PCI; pharmacoinvasive strategy
OBJECTIVES
This study correlated the multi - detector computed tomography (MDCT) calcium scores with the results of coronary angiography in diabatic and/or hypertensive patients with atypical angina pectoris in order to assess its value to predict or exclude significant coronary artery disease (CAD).
BACKGROUND
Muti-detector computed tomography is a sensitive method to detect coronary calcium. However, it is unclear whether it may play a role as a filter before invasive procedures in patients with atypical angina pectoris.
METHODS
A total of 150 patients (116 men and 34 women) with diabetic and/or hypertension for at least 5 years and atypical angina pectoris from a single center were included in our study. patients underwent calcium screening with MDCT and have calcium score more than 100 , then all patient underwent invasive coronary angiography.
RESULTS
The Mean age was 62±5.7 and 77.3% were male, 78% of men and 88.2 % of women revealed significant coronary stenoses (> 50% lumen narrowing of left main trunk stenosis and > 70% stenosis of any epicardial coronary artery). Significant correlation between calcium scoring and significant coronary artery stenosis was seen (P: 0001). A 70% were DM, 90% were hypertensive and 61.3% were HTN and DM. The LAD artery was the most stenotic artery by 53.3% followed by RCA (37.3%) and finally LCX (30.7%). one significant coronary artery was 42% followed by two significant CAD (26.7%), while 9.3% included three-vessel disease. The significant coronary artery diseases was increased with age ( P: 0003).
CONCLUSIONS
Coronary calcium proved to have good diagnostic performance for significant coronary artery stenosis in patient with atypical angina pectoris.
Coronary heart disease is the leading cause of mortality in the Palestine and worldwide. The current gold standard to evaluate coronary artery disease is invasive coronary angiography (ICA). In Gaza alone, between 2015 and 2018 about 5411 coronary angiography and percutaneous coronary intervention procedures rose by 48 % over the last 4 years from a rate of 80 per 100,000 population in 2015 to 155 per 100,000 population in 2018. [1]
The significant coronary artery stenosis among patients underwent diagnostic coronary angiography were 54.3% of patients with stable ischemic heart disease, 66.7% in patients with unstable angina pectoris and 92.7% in patient with ST elevation myocardial infarction. [1]
There are two major concerns for the stable ischemic coronary artery disease patients: the first point: Coronary angiography is over-used and low-yield. And second point: Non-Stress imaging has improved diagnostic accuracy and can avoid invasive coronary angiography
Recent trials suggested the Coronary artery calcium (CAC) is highly specific feature of coronary atherosclerosis, and many CAD patients are asymptomatic, and early detection and treatment of CAD can reduce the incidence of acute coronary syndrome [2,3]
Studies have also shown that the coronary artery calcium score (CACS) is useful for refined risk stratification, particularly with high-risk patients and those with diabetes mellitus [4,5]
Our aim of this study to confirm correlation between computed tomographic calcium score with intermediate or high risk (Agatston score >100) and invasive coronary angiography (ICA) in patient with age more than 40 years and have diabetes and/or hypertension since at least 5 years with atypical angina pectoris.(Figure 1)
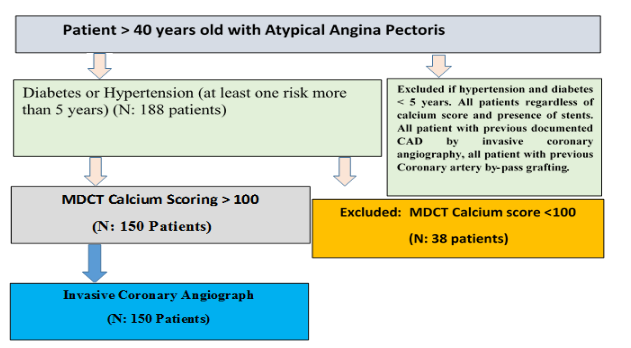
In CACICA Gaza trial we conducted a cross-sectional study enrolling atypical angina pectoris patients with diabetes and/or hypertension for at least 5 years referred for cardiac evaluation of coronary artery disease before invasive coronary angiography. The inclusion period was from June 2018 to August 2019.
Population of Patients:
A total of 150 consecutive patients with coronary Calcium scoring > 100 according to agatston score and age older than 40 years patient with atypical angina pectoris and the presence of at least 1 of the following characteristics:
The exclusion criteria were age younger than 40 years, acute coronary syndrome patients, Diabetes and hypertension treatment for less than 5 years . All patients regardless of calcium score and presence of stents. All patient with previous documented CAD by invasive coronary angiography, All patient with previous Coronary artery by-pass grafting. Written informed consent was obtained from all patients.
Definition of Atypical angina pectoris (6)
Meets two of the following characteristics.
(i) Constricting discomfort in the front of the chest or in the neck, jaw, shoulder, or arm;
(ii) Precipitated by physical exertion;
(iii) Relieved by rest or nitrates within 5 min.
The amount of calcium in the coronary arteries was assessed with a Multi Detector-Row CT (MDCT) scanner (IDT 124, Philips Medical Systems, and The Netherlands). Subjects were positioned within the gantry of the MDCT scanner in supine position. During a single breath hold, images of the heart, from the level of the tracheal bifurcation to below the base of the heart, were acquired using prospective ECG triggering at 50–80% of the RR-interval, depending on the heart rate. Scan parameters were 16x1.5 mm collimation, 205 mm field of view(FOV), 0.42 s rotation time, 0.28 s scan time per table position, 120 kVp and 40–70 mAs (patient weight <70 kg: 40 mAs; 70–90 kg: 55 mAs; >90 kg: 70 mAs). Scan duration was approximately 10 s, depending on heart rate and patient size. After completing a the study, one scan reader manually selected the calcifications within one of the coronary arteries (left main, left anterior descending, left circumflex, right coronary artery, and PDA),three-dimensional connected components above the standard threshold of 130 Hounsfield Units (HU) were considered candidate calcifications. Each patient was assigned to one of five CVD risk categories based on Agatston score : low(0),fair(1–10),moderate(11–100),intermediate(101–400),high(>400), if patient have intermediate or high agatston score coronary angiography is recommended.
Coronary angiography: The Judkin’s technique was used with at least four views of the left coronary artery and two views of the right coronary artery. Analysis of the coronary angiograms was done by an independent, experienced observer who was unaware of the coronary calcium score. The decision to perform angiography was not influenced by the calcium score. Angiography was performed within 30 days after the MDCT. Significant stenosis was defined as > 50% lumen narrowing of left main trunk stenosis and > 70% stenosis of any epicardial coronary artery.
Statistical analysis:
All data was analyzed by SPSS (version 23, IBM Corporation), For continuous variables that were not normally distributed (p< 0.1 [Shapiro-Wilks test]), the testing for differences was done using the nonparametric Wilcoxon test. For normally distributed variables, the Student t test was employed. Categorical data were compared using the Fisher exact test or the Pearson chi-square test. The distributions of continuous variables were presented with their median and range (if not normally distributed), respectively, with their mean and SD. Categorical data were presented with absolute frequencies and percentages. A spearman correlation coefficient between CTCS and Coronary angiography, results of the statistical tests are presented with two-tailed P value of < 0.05 were considered significant.
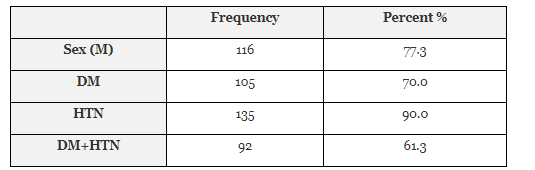
The total number of cases in this study was 150 with mean age 62±5.7, the majority of participants 77.3% were male, 70% were DM, 90% were hypertensive and 61.3% were HTN and DM. Table 1
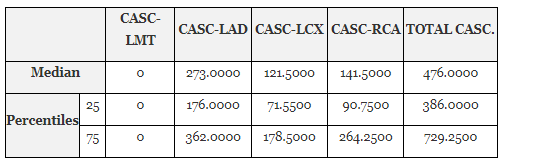
Distribution of calcium deposit in coronary artery regards to agatston score
The quantification of calcium deposit in each coronary artery and total calcium score. The LAD artery got the largest quantity of calcium followed by RCA artery and finally LCX artery.
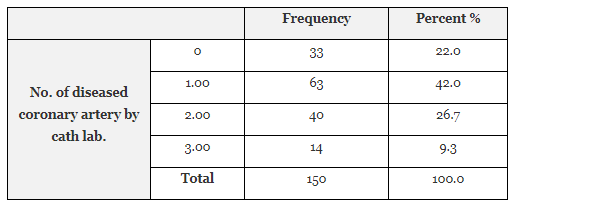
Number and percent of diseased coronary artery regards to Coronary angiography
Most coronary angiography result included one significant coronary artery by 42% followed by two significant CAD (26.7%), while 9.3% included three-vessel disease.
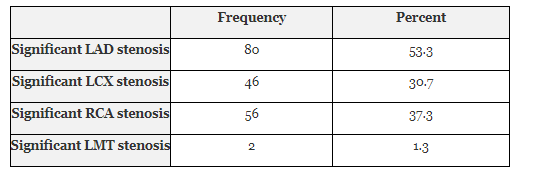
Number and percent of significant stenosis in every coronary artery
Table 4.3 shows that the LAD artery was the most stenostic artery by 53.3% followed by RCA (37.3%) and finally LCX (30.7%).
Comparison between coronary angiography and CT calcium scoring results: no difference between significant coronary artery stenosis in patient group with total Calcium score > 400 and in patient group with calcium score <400. But the major group of significant number of coronary arteries was one vessel comparison between 2 and 3 significant coronary artery stenosis (P :0.018)

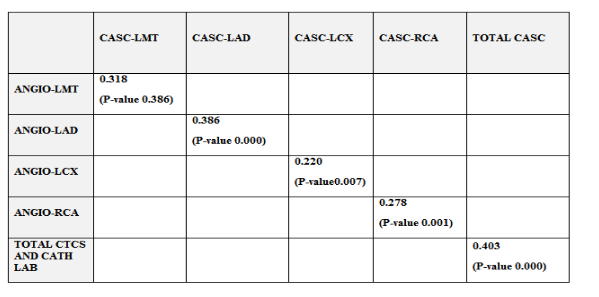
Correlation between cath lab. and CT calcium scoring results
A sperman correlation coefficient between CTCS and Coronary angiography. was done and revealed that there was a direct intermediate relationship between CTCS and Cath Lab except the LCX, where the relationship was weak direct relationship.
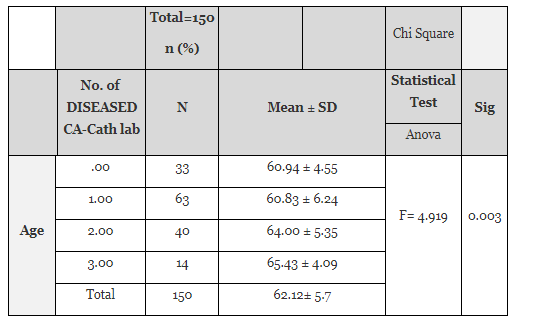
No statistical significant differences at level (P- value < 0.05) between number of diseased coronary artery and sex, DM and HTN. While there was statistical significant differences at level (P- value < 0.05) between number of diseased coronary artery and age.
This study describes the value of MDCT calcium screening in patients with atypical angina pectoris with diabetes and/or hypertension for at least 5 years who were referred to our center with suspected CAD to be proven or excluded by coronary angiography.
The strength of this study is that all the patients were evaluated in a single center with the same technology; MDCT scans and angiography were performed within a 30 days of each other and were read by independent observers in a blinded manner.
There was no significant difference in coronary calcium between men and women however, the reliability of calcium testing in predicting significant stenosis was equally effective in men and women. Finally, the diagnostic benefit of calcium screening is maintained for all age groups.
The calcium score percentiles adjusted for age and gender are significantly higher in symptomatic versus asymptomatic patients with risk factors [7].
There is no agreement on what score cut point should be used in the clinical setting. Some studies solely used exclusion of any calcium [8 –12]. Other studies used a fixed score of 100 (13). In our study, significant coronary stenosis diagnosed by coronary angiography was found in 78% of the patient who had calcium score > 100.
In CONFIRM trial, comparison between calcium scoring versus computed tomography coronary angiography. The patient with calcium score 100-400 and > 50% coronary artery stenosis were 35%, and patients with calcium score > 400 had 60% significant coronary artery stenosis. In our study comparison between calcium scoring versus invasive coronary angiography. The significant coronary artery stenosis was 78%, In CONFIRM trial the diabetic patient was 18% but in our trial the diabetic patient was 90%. In CONFIRM trial the hypertension was 59% and in our trial 70%. This difference may be related multiple risk factors: First, High risk patient group in our trial compared with confirm trial. Second, patient group in our trial all patient was atypical angina pectoris, CONFIRM trial the patient group involved typical angina, atypical angina, non-cardiac chest pain and dyspnea. Third, coronary artery stenosis confirmed by invasive coronary angiography but in CONFIRM trial computed tomography coronary angiography (14)
In the PROMISE Study, about 78% was atypical angina pectoris, 65% hypertensive and 21% diabetic, the significant coronary artery stenosis was 36% in patient with calcium score > 400 and 20% in patients with calcium score 100- 400. [15] in our trial 100% of patient was atypical angina pectoris, and 90% was diabetic.
In our trial patient with diabetic and/or hypertensive for at least 5 years and Calcium scoring 100-400 need coronary angiography, also supports the sequential testing algorithm evaluated in the CRESCENT trial (Calcium Imaging and Selective CT Angiography in Comparison to Functional Testing for Suspected Coronary Artery Disease) a prospective randomized trial that used CAC as a first-line test, advancing to CTA when CAC scores were 1 to 400. [16]
Clinical implications. On the basis of our results, we see an indication for calcium screening in patients with atypical angina pectoris and had diabetic and/or hypertension for at least 5 years, especially if noninvasive tests are not feasible or inconclusive. Calcium screening with MDCT has the potential as a filter in atypical symptomatic patients to reduce the number of invasive procedures which do not lead to intervention.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
This article is part of the Cardiology Board thesis. Palestinian Cardiology Board -AL Shifa Hospital – Gaza - Palestine
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
