
Research Article | DOI: https://doi.org/10.31579/2578-8965/102
1Omam Hospital, Department of Gynecology and Obstetrics, 2 Elbatal Ahmed Abdelaziz St., 12611 Giza, Egypt
2Department of Primary Care and Population Health, University of Nicosia Medical School, 2408, Nicosia, Cyprus
3Ain Shams University, Faculty of Medicine, Department of Pathology, 38, Abbasia, Al Wailli, 11566 Cairo, Egypt
4President Scientific Council Egyptian Board of Pathology
5St George’s, University of London MBBS Programme at the University of Nicosia Medical School, 2408, Nicosia, Cyprus
6University of Nicosia - Medical School, and Aretaeio Hospital, 2024, Nicosia, Cyprus
*Corresponding Author: Vasilios Tanos, University of Nicosia - Medical School, and Aretaeio Hospital, 2024, Nicosia, Cyprus
Citation: Sayed El-Akhras, Mohamed A. elenen, Christiana Demetriou C., Nafissa M.A El Badawy, Balami S., Tanos V. (2022) Correlation of Bladder Wall Endometriosis Histological Location, To Infertility Patients’ Clinical Characteristics and Severity of Peritoneal Endometriosis. J. Obstetrics Gynecology and Reproductive Sciences; 6(2) DOI:10.31579/2578-8965/102
Copyright: © 2022, Vasilios Tanos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 October 2021 | Accepted: 30 November 2021 | Published: 05 January 2022
Keywords: bladder endometriosis; bladder wall endometriosis; peritoneal endometriosis; bladder endometriosis and patients’ clinical characteristics, histopathology and bladder endometriosis
Study question: What is the correlation of bladder wall endometriosis histological location, to the severity of peritoneal endometriosis in infertility patients?
Summary answer: Secondary infertility, back pain, micturition problems, history of ectopic pregnancy and number of abortions can probably be considered as high-risk factors for bladder wall endometriosis for infertility patients.
What is known already: Bladder and/or ureter endometriosis occur in 70–85% among patients with deep infiltrating endometriosis. The knowledge regarding the bladder wall involvement with endometriosis in association to peritoneal endometriosis and infertility patients’ clinical characteristics is limited.
Study design, size, duration: Retrospective, longitudinal cohort, Sixty-six, primary and secondary infertility patients, collection of surgical and clinical data between 2010 to 2018.
Participants/materials, setting, and methods: An experienced histopathologist on endometriosis was asked to review all the patients’ histopathological results. The histopathological reported findings were reviewed prior to the study to reassure the bladder wall depth of endometriosis involvement.
The operation and tissue macroscopic description reports before processing were also reviewed. Attention was paid for possible discrepancies or missed important data that could influence the histopathological results. In cases where results were equivocal, the paraffin blocks were available for additional sections for reassuring the diagnosis. An extra effort was made to meticulously observe and identify the involvement of the bladder serosa, muscularis and mucosa with endometriotic cells and glands.
Main results and the role of chance: Primary infertility was the indication for the current laparoscopic surgeries in 32 out of 66 (48.5%) patients and secondary infertility for the rest of the group. The highest incidence of bladder endometriosis (BE) was detected on the serosa of 12 patients and in the detrusor muscle (DM) of 11 cases. Bladder serosa endometriosis (BSE) was significantly more prominent among patients with history of ectopic pregnancy (p=0.004) and among patients with secondary infertility (p=0.029). Destrusor muscle endometriosis (DME) was significantly more frequent (p=0.012) in patients with increasing number of abortions. DME highest rates of 37.7% were observed among the severe spread of abdominal endometriosis as compared to 19% of the cases with bladder serosa endometriosis. No statistically significant difference found between serosa and detrusor muscle endometriosis involvement, when compared to severity and spread of endometriosis within the abdominal cavity. Back pain was most prominent with statistical significant difference (p=0.007) in 8 patients with BSE + DME as compared with other groups of patients (4 BSE, 3 DME and 3 BME+DME patients). Among 30 cases with an ovarian endometrioma detected by TVU, DME was diagnosed in 13 patients, in serosa of 10, and in serosa and DM of 6 patients. Statistical analysis was performed using Pearson chi-square, Fisher’s exact tests and the Kruskal-Wallis test by STATA version 15 SE (StataCorp. 2017).
Limitations, reasons for caution: This is a cohort retrospective study. There is a possibility that other areas with endometriosis were also involved in the BW other than those diagnosed and treated. The mixture of patients with primary and secondary infertility could also affect the results, although statistical analysis did not show any significance in BWE, clinical symptoms and surgical findings. BE is rarely an isolated condition, and other forms of endometriosis are frequently concomitant
Wider implications of the findings: Detrusor muscle endometriosis involvement was in 68% and bladder serosa in 32% of all cases with bladder endometriosis and infertility investigated. The severity of the peritoneal endometriosis can probably direct to meticulous intraoperative investigation for bladder endometriosis.
Study funding/competing interest(s): This study has been performed without any funding
Bladder Endometriosis in infertility patients
Urinary tract endometriosis is evident in approximately 1% of women with endometriosis (Leone Roberti Maggiore et al., 2017). Its prevalence increases to 19–53% among patients with deep infiltrating endometriosis (DIE) (Gabriel et al., 2011; Knabben et al., 2015). DIE is a particular form of endometriosis that penetrates > 5 mm under the peritoneal surface (Koninckx and Martin, 1994). Bladder and/or ureter endometriosis occur in 70–85% of cases with severe endometriosis (Knabben et al., 2015).
The anatomical proximity of the bladder to the anterior cul-de-sac and uterus as well as the standing posture and the effects of gravity, have been suspected to contribute in the development of endometriosis in the vesicovaginal septum (Vercellini et al., 2002). The distance between the bladder and anterior uterine wall seems to be a crucial factor since no BE was detected in cases with retroverted uterus (Vercellini et al., 2002). Spontaneous growth of bladder peritoneum and interstitial endometriotic nodules is possible, induced by oestrogens during artificial reproductive techniques and may cause obstetrical complications especially during caesarean section (Somigliana et al., 2015a; Leone Roberti Maggiore et al., 2016). Trans-tubal regurgitation of menstrual endometrium facilitates implantation on peritoneal surfaces.
BE is defined as the presence of endometrial glands and stroma in the detrusor muscle. The dome and the base are the most frequently affected sites. Primary BE is extremely rare. It presents as a spontaneously occurring manifestation among a generalized pelvic endometriosis. So far, the development of adenomyotic nodules found in the verumontanum, trigone, ureterovesical junction and lateral wall of the bladder has been attributed to Mullerian duct remnant metaplasia (Vigano et al,. 2009). Secondary BE is considered a dissemination and progression of cells due to iatrogenic causes, occurring after pelvic surgery, such as caesarean delivery or hysterectomy or secondary to other forms of pelvic endometriosis (Somigliana et al., 2007). BE is not an independent form of the disease and at least one other site of the abdomen is involved Abrao et al., 2009). According to ASRM staging system, the presence of BE is classified as stage IV, as DIE.
When endometrial glands and stroma are present within the detrusor muscle, it is defined as bladder adenomyosis. Ninety percent of patients with BE, usually complain of urinary frequency, dysuria and less frequently of bladder pain, urgency and haematuria Abrao et al., 2009). Hence, dysuria, pelvic pain and micturition problems in absence of urinary tract infection should raise suspicion and direct the mode of management in these patients.
BE as an isolated pathology does not seem to cause infertility. However, it is reported that surgical interventions in cases with deep infiltrating endometriosis and BE lesions have been increasing the IVF pregnancy rates to 42–44% (Meuleman et al., 2009; . Soriano et al., 2011). In case of fertility treatment, it has been calculated that only 20–25% of women may really benefit from an isolated bladder nodule resection (Meuleman et al., 2009). IVF appears to be more effective and less risky compared to bladder surgery in patients with moderate pelvic endometriosis and BE (Somigliana & Garcia-Velasco, 2015b).
In this cohort study, the impact of abdominal endometriosis on the bladder wall depth of endometriosis involvement has been investigated among infertility patients. All patients were diagnosed with BE. The extent of the peritoneal endometriotic lesions diagnosed by laparoscopy was corelated to BE according to histopathological findings, including the bladder serosa, detrusor muscle and mucosa. Patients’ age, past health problems and operations, as well as present laparoscopic surgery results were investigated in relation to BE involvement. A potential association between patients’ parity, gravidity, infertility, pain status, and menstruation characteristics with the bladder wall endometriosis involvement was also investigated.
Sixty-six patients operated in Omam private Hospital in Cairo, diagnosed with bladder endometriosis (BE) between 2010 and 2018 were included in this cohort study. Patients records, including age, gravidity, parity, obstetrical outcome, history of health problems and operations, clinical symptoms and examination results, current minimally invasive surgery indication and results, and histopathological reports were extracted, and compiled into a database. Tables I, II and III demonstrate in detail patients’ clinical records and histopathological examination results in relation to BE involvement.
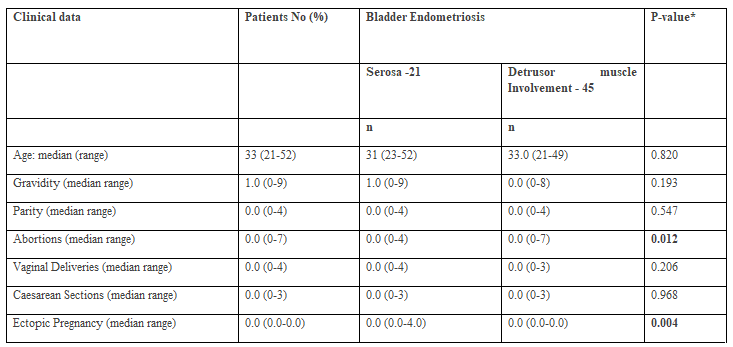
* P-value compares each variable between bladder endometriosis categories.
As the numbers are no low, table 1 would benefit from showing n numbers and mean in addition to median and range. Also ensuring that the abbreviation and terminology are consistent between the tables and the
text in the paper.
Why isn't the TVU data presented in the tables (polyps, fibroid)?

Endoma = endometrioma
* P-value compares each variable between bladder endometriosis categories
* P-value from a Pearson chi-square test
For categorical variables, the Pearson’s Chi-square test was used. For continuous non-normally distributed variables, the Kruskal-Wallis test was used.
∞ Only among non-virgin participants (ntotal=60, nserosa=20, nDetrusor muscle Involvement within=37)
BSE = Bladder Serosa Endometriosis
DME = Detrusor Muscle Endometriosis
BME = Bladder Mucosa Endometriosis
Surgical Management
All patients underwent laparoscopy and were diagnosed with an endometriotic lesion on the bladder serosa mainly on the anterior and fundal walls. Since the nodule develops from the outer layer of the bladder wall towards the detrusor muscle inner layer, local excision was performed until free from endometriosis margins were visually confirmed. In excisions that involved only the bladder serosa, a single layer wound closure was performed, while for interstitial excisions, the wound was closed in 2 layers, using 2.0 and / or 3.0 PDS sutures. The bladder serosa integrity was then examined by infusing into the bladder 300 ml of normal saline stained with methylene blue dye. The serosa part of the specimen was designated by placing a suture, assisting histopathologist orientation. Cystoscopy was performed in 15 cases and 11 cases underwent ureteric stenting.
Histopathology
The histopathological reported findings were reviewed prior to the study to reassure the bladder wall depth of involvement. An experienced histopathologist on endometriosis was asked to review all the patients’ histopathological results. The operation and tissue macroscopic description reports before processing were also reviewed. Attention was paid for possible discrepancies or missed important data that could influence the histopathological results. Light microscopy using x40 x100 magnification was performed on all the patients’ sections slides. In cases where results were equivocal, the paraffin blocks were available for additional sections for reassuring the diagnosis. An extra effort was made to meticulously observe and identify the involvement of the bladder serosa, muscularis and mucosa with endometriotic cells and glands.
Demographic, reproductive and medical history variables were compared between women with different bladder wall endometriosis and adenomyosis involvement using univariate tests. Bladder endometriosis was investigated according to depth of BWE involvement and according to four histopathological localizations of endometriosis
(Serosa [BSE]
Detrusor muscle [DME])
(Serosa [BSE] vs. Detrusor muscle [DME]
Mucosa [BME] & Detrusor muscle [DME]).
For categorical variables, the Pearson chi-square or the Fisher’s exact tests were used, the latter being reserved for comparisons with small sample numbers. For continuous non-normally distributed variables, the Kruskal-Wallis test was used. The statistical significance threshold was set at 0.05. Statistically significant associations with depth of BWE involvement were also tested with univariate logistic regression analysis. All statistical analyses were performed using STATA version 15 SE (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Ethical approval: The study was examined and approved by the internal Bioethics committee of the OMAM Hospital, Cairo.
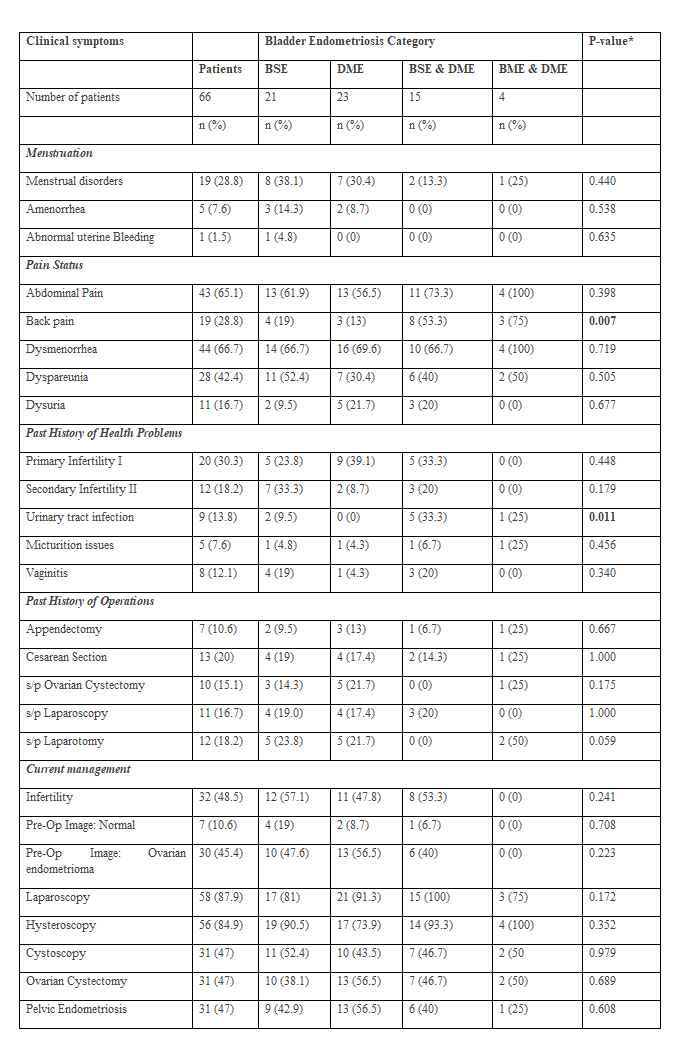
Among 66 patients diagnosed with bladder biopsy confirmed endometriosis, in 21 cases, endometriosis was isolated on the bladder serosa (BSE) and in 45 cases endometriosis was found within the detrusor muscle (DME) (Tables I&II). The frequency of bladder endometriosis (BE) involvement according to histological findings on bladder serosa and detrusor muscle, was investigated in association with age, gravidity, parity, number of abortions, ectopic pregnancies, normal deliveries and caesarean sections, as demonstrated in Table I. The frequencies of BSE and DME in association to menstruation, pain status, past medical and surgical history, management and endometriosis spread within the abdominal cavity are presented in Table II.
The average patients’ age recorded for BSE was 31 years and for DME 33 years. No significance was found between the patients’ age in both groups. No significance was found among the two groups for gravidity, parity, vaginal and caesarean section mode of delivery (Table I). BSE was significantly more prominent among patients with history of ectopic pregnancy (p=0.004) (Table I) and among patients with secondary infertility (p=0.029) (Table II). DME was significantly more frequent (p=0.012) in patients with increasing number of abortions (Table I).
No significance was found between serosa and detrusor muscle endometriosis involvement, when compared to severity and spread of endometriosis within the abdominal cavity (Table II).
Micturition problems were reported by 5 (7.6%) patients, urinary tract infection was diagnosed in 9 (13.8%) patients and vaginitis in 8 (12.1%) out of the 66 patients. Looking at the four histopathological BWE localisation categories, among 5 patients with micturition problems, endometriosis was diagnosed in 1 patient in each 4 histological locations, i.e serosa, serosa + DM, DM + mucosa and mucosa. In 8 patients with vaginitis, BE was mostly detected in the bladder serosa and non in mucosa and DM (Table III).
Seven patients reported a past-operations history of appendicectomy and 13 had caesarean sections, BE was mostly detected in BW and serosa. Ten patients had ovarian endometrioma surgery, 11 patients had laparoscopic surgery and 12 patients had laparotomies for various health issues, and BE was mostly detected in bladder serosa and DM. None of the past surgeries reported were found to have any statistically significant correlation with the BWE subgroups diagnosis (Table II).
Since all patients with BE were stage IV according to ASRM endometriosis classification. In order to be able to fulfil the scope of our study, the severity of endometriosis within the abdominal cavity was defined as mild when 20 cases presented only multiple foci of endometriosis in the pelvis, moderate when in 25 patients endometrioma was present and severe when 21 patients had deep infiltrating nodule/s. Pearson x2 test and Kruskal Wallis test used to compare each variable mild, moderate and severe endometriosis between BE histological locations did not reach any significance (Table II). Although missing of any significance, the statistical model showed a higher risk of DME when severe endometriosis was reported in the abdominal cavity.
In association with the four categories, the frequency of menstrual abnormalities and pain, including abdominal pain dysmenorrhoea, dyspareunia and dysuria were associated with DME involvement, without any significance. However, back pain was most prominent and significance (p=0.007) in 8 patients with BSE + DME as compared to BSE found in the serosa of 4 patients; in DME of 3 patients and BME + DME of 3 patients. (Table III). An association between the BWE and patients’ past history of health problems and operations, as well as current management findings and operative approach, did not show any significance among the endometriosis histological locations across the BW as defined above.
The highest incidence of BE was detected in the DM in 9 patients with primary (I) infertility and in the bladder serosa of 7 patients with secondary (II) infertility (Table III). No significance was noted among the I and II infertility patients and the histological locations of endometriosis on the serosa, DM and mucosa. Among patients with urinary tract infection (UTI), endometriosis was mostly diagnosed with significance (p = 0.011), in patients with endometriosis on the serosa and DM as compared to women with endometriosis throughout the BW (serosa, DM and mucosa). No UTI was reported among patients with DME alone (Table III).
Primary infertility was the indication for the current laparoscopic surgeries in 32 out of 66 (48.5%) patients and secondary infertility for the rest of the group. The highest incidence of BE was detected on the serosa of 12 patients and in the DM of 11 cases. Preoperative uterine imaging by TVU revealed that in 7 cases with benign pathologies like fibroids and / or polyps, there was no correlation to any BE histological locations either. Among 30 cases with an ovarian endometrioma detected by TVU, DME was diagnosed in 13 patients, in serosa of 10, and in serosa and DM of 6 patients.
A group of 8 patients converted from laparoscopy to laparotomy. In 58 patients that underwent laparoscopic surgery DME was evident in 21 cases, in BSE in 17 women, BSE and DME in 15 women and BME and DME in 3 patients. However, no significance was found among the BE histological locations and laparoscopic surgeries. Pelvic and abdominal endometriosis, stripping of endometrioma and cystoscopy were diagnosed and performed in 31 (47%) patients and BSE and DME was diagnosed in 38 – 56.5% of the cases without any significance. Among 56 patients who underwent hysteroscopy, BSE was detected in 21 cases, in DME in 23 cases, in BSE+DME in 15 and BME+DME in 4 cases, however without reaching any significance (Table III).
Univariate logistic regression analysis of endometriosis on the bladder serosa and DM associated to menstruation, pain status, past medical and surgical history, management and endometriosis spread within the abdominal cavity. No significance were found among patients’ age and obstetrical history when univariate logistic regression analysis was performed, comparing BSE and DME. BSE of 33.3% was significantly more prevalent (p=0.036), among patients with secondary infertility as compared to DME involvement 11.1%. No significance between BSE and DME were detected for the rest of the 27 parameters underwent regression analysis.
In this cohort study we tried to identify if histopathological locations of BWE were associated with patients’ age, obstetrical, medical and operation history, clinical characteristics, management and spread of endometriosis within the abdominal cavity. Among the 66 patients with BE, histological sections diagnosed endometriosis in only 4 cases on the bladder mucosa 6%, in 21 cases on the serosa 32%, and in 45 cases within the DM 64%. Many sections (19/66) 29% presented endometriosis in more than one layer of the BW. The high incidence of 68.2% of DM endometriosis involvement, agrees with earlier studies which presented similar results (Leone Roberti Maggiore et al., 2017). The fact that no significance was found between BSE and DME involvement, when compared to severity and spread of endometriosis within the abdominal cavity, complies with the current experience of symptoms variability and abdominal endometriosis severity (Table II). Although without any statistical significance, the higher risk of DME when severe endometriosis was reported in the abdominal cavity draws the attention for meticulous intraoperative BWE investigation. The statistically significant more frequent DME in patients with increasing number of abortions (p=0.012) seems to mimic the development of adenomyosis within the myometrium. The anatomical proximity of the bladder and uterus allows for the increased risk of trauma during the uterine intracavitary interventions and subsequently increased risk of developing DME, i.e. bladder wall adenomyosis. Circumstantial evidence suggests that microtraumatizations allow for the activation of the ‘tissue injury and repair’ mechanism which stimulates local estrogen production. Consequently, leading to permanent hyperperistalsis and self-perpetuation of the disease process. (Leyendecker G. et.al., 2009)
There are higher rates of pain, infertility, micturition problems, past operations and severity of endometriosis findings within the abdominal cavity in patients with DME, as compared to those with BSE. Despite the findings lacking significance, this supports previous literature findings and reassures the study’s results (Leone Roberti Maggiore et al., 2017). Indeed, back pain was most prominent (p=0.007) in 8 patients with BSE + DME as compared to endometriosis in the other histopathological locations of BWE; denoting the importance of BWE involvement within the serosa and DM and might be considered as a significant pre-operative symptom. This can be attributed to the neuroanatomy of the pelvis. De Sousa et al. demonstrated the spread of endometriosis from the uterine cavity along the autonomic nerves in the pelvis into the lumbosacral plexus [28]. Further spread of the endometriotic lesions into the spinal nerves and even the dura of the spinal cord was proposed to be a possible aetiology of DIE [1,28].
The backpain symptom may direct patients to 3D ultrasound (US) and magnetic resonance imaging (MRI) focusing on BWE diagnosis. It has been suggested that 3D US acquisition may improve endometriotic nodule localisation and evaluation of its size, volume, and infiltration of the bladder wall in comparison to two-dimensional transvaginal ultrasound (TVS) (Thonnon et al., 2015). TVS is the most accurate in defining the size of the lesions, infiltration of the DM, and continuity with extravesical lesions (Fedele et al., 1997). Also reports high accuracy, reproducibility and specificity but fair sensitivity in the diagnosis of BE (Tammaa et al., 2015). BWE in TVS appears as a filling defect of the posterior wall with iso/hypoechoic protrusions into the lumen, usually not vascularised (Leone Roberti Maggiore et al., 2017).
The higher rates of UTI (p=0.011) in patients with BSE+DME reflects the urinary bladder dysfunction due to BWE and to chronic inflammation caused by endometriosis. Dysuria has been reported in 21–69% of patients with BWE. Bladder pain and frequency and less commonly haematuria, urgency, and urinary incontinence are symptoms associated with the presence of BWE (Villa et al., 2007;,Leone Roberti Maggiore et al., 2015). Haematuria was reported in only 2 women out of the 66 patients. Patients experiencing urgency and/or urinary frequency, dysuria provoked during bladder filling, raises the suspicion of a DME.
In general, DIE is associated with lower urinary tract symptoms and the incidence ranges between 2% and 77% (Bonneau et al., 2013;,Ballester et al., 2014). Endometriosis and interstitial cystitis have been associated with recurrent cystitis and overactive bladder and symptoms of chronic bladder and pelvic pain or discomfort, and may be accompanied with persistent urge to void or frequency in the absence of any identifiable pathology or infection (van de Merwe et al., 2008;,Hanno et al., 2010). Univariate logistic regression analysis did not show any significant correlation between DME and UTI micturition problems or vaginitis. A recent study reported no difference in the rate of urgency, urinary frequency, voiding symptoms and bladder pain between patient with posterior endometriosis plus BE compared with those with posterior endometriosis only (Panel et al., 2016). Women of reproductive age complaining of lower urinary tract symptoms, particularly in combination with dysmenorrhoea, back pain and/or anterior sensitivity during vaginal examination, should be always considered as high risk for BWE. 2/3D TVS and MRI should follow although absence of endometriotic nodules in imaging cannot exclude BWE, hence, laparoscopy and eventually cystoscopy are necessary for final diagnosis and treatment.
In 15 out of 66 cases, cystoscopy was performed to rule out endometriotic lesions on the bladder mucosa. Four cases advancing from the bladder serosa towards the DM and appearing on the mucosa were diagnosed. Typical red or bluish nodules have been observed but not any ulcerations, which comes into agreement with other studies (Thonnon et al., 2015;,Fedele et al., 1997). Cystoscopy has limited value for screening or routine purposes in women with endometriosis and should be reserved for those cases at high risk for BME. Identifying the endometriotic lesion position, especially those close to the trigonum and ureteral ostia, inadvertent trauma can be avoided during surgery. Cystoscopy is mandatory in cases with suspicion of malignancy, excluding bladder carcinoma, varices, papillomas, angiomas, and detrusor mesenchymal tumours (Leone Roberti Maggiore et al., 2017).
The highest incidence of BE involving only the serosa in 21 patients and only the DM of 23 cases follows the results of other studies that BWE presents a severe form of endometriosis with bad prognosis for fertility potential [(Vercellini et al., 2014a;,Vercellini et al., 2014b)]. Logistic regression analysis as presented in the results, demonstrated that BSE 33.3% was significantly more prevalent (p=0.036) among patients with secondary infertility, as compared to DME involvement of 11.1%; this probably reflects a partial protection by prior pregnancy, but not complete immunity of the disease. Although current research suggests no evidence on pregnancy reducing the size or number of endometriotic lesions, it might be worth questioning the conclusions of these few studies of very limited quality.
Brigitte Leeners, Fabia Damaso, Nicole Ochsenbein-Kölble, Cindy Farquhar, The effect of pregnancy on endometriosis—facts or fiction?, Human Reproduction Update, Volume 24, Issue 3, May-June 2018, Pages 290–299, https://doi.org/10.1093/humupd/dmy004
Within the context that adenomyosis may interfere with fertility, similarly women with BE may probably, at least partly, contribute to uterine dysfunction. However, in most series published, no adenomyotic nodules of the uterine wall were found in association with BE [Leone Roberti Maggiore U, et al. 2017]. Interestingly, 11 cases of male endometriosis reported in the literature, four developed endometriosis of the bladder concomitant with high estrogen exposure, probably indicating a similar susceptibility between the detrusor muscle and myometrium [Leone Roberti Maggiore U, et al. 2017]. The fact that BSE was statistically significant among patients with secondary infertility and history of ectopic pregnancy, reflects the consequences of endometriosis and formation of intrabdominal adhesions due to chronic inflammation.
Although the big majority of the patients 53/66 (80.3%) had a history of abdominal operations, no significance was found of BWE and histological subgroups, among these patients, neither of the 13 cases underwent caesarean sections and the 10 cases after ovarian endometrioma surgery. In 46 out of 66 patients, 70% who had the bladder wall affected by endometriosis, underwent a gynaecological surgical procedure prior to diagnosis of BE, raising the possibility of iatrogenic dissemination of endometriotic cells. However, a recent cross-sectional incidence of isolated BE, reported patients with and without a history of uterine surgery 37.5% and 41.7% respectively without any significance (p = 0.6) (Leone Roberti Maggiore et al., 2017). Among BWE cases, the incidence observed was 58.6% (95% confidence interval [CI] 45.2–71.2) for superficial peritoneal implants, 44.8% (95% CI 32.2–58.2) for ovarian endometriomas, 81.0% (95% CI 68.4–89.6) for adhesions, and 27.6% (95% CI 16.7-40.8). Hormonal treatments are effective for a temporal disease suppression but not curing. Significant improvements in pain and urinary symptoms have been observed after excision of the whole bladder lesion, which also minimises the risk of recurrence [Soriano et al., 2016;,Seracchioli et al., 2010;,Chapronet al., 2010)].
In our study 45 cases underwent a full thickness bladder wall segmental excision due to severity of the disease.
In another 21 cases, BSE was diagnosed after wedge resection of the lesion and confirmation of clear margins from the disease. Several studies have shown that segmental cystectomy is an effective technique with excellent long-term results in terms of symptom relief and recurrence [(Chapron et al., 2010;,Kjer et al., 2014)]. Excision of endometriotic nodules of the bladder may lead to inadvertent removal of healthy bladder muscle, particularly in case of large endometriotic lesions. Postoperative complications and symptoms are mainly due to small bladder volume. An effort to spare most of the healthy bladder tissue is imperative. [(Fedele et al., 2005;,Vercellini et al., 2009;,Antonelli et al., 2006)]. Preventive ureteric catheterisation was performed in 11 cases due to lesion proximity to trigonum. Ureters stenting can be of great help when surgery is performed on the posterior bladder wall and endometriotic nodules are close to the ureteral meatuses [(Vercellini et al., 1998)].
Surgery for BE usually accompanies treatment for adhesions, endometriomas, superficial implants, and other deep localisations of the disease (Somigliana et al., 2007). Deep peritoneal endometriosis is associated with adenomyosis and according to our study there is a higher risk of DME in relation to severity of the peritoneal endometriosis; although there was no significance. [(Kunz et al., 2005;,Exacoustos et al., 2013)]. Occasionally bladder lesions are buried under adhesions while chronic inflammation and extended fibrosis present an operative challenge. In a study by Kovoor et al 50% of infertile women with BWE conceived naturally after an intervention [(Wells et al., 2014)]. The surgery radicality of DIE and BWE for infertility treatment remains debatable (Somigliana & Garcia-Velasco, 2015b).
This is a cohort retrospective study. There is a possibility that other areas with endometriosis were also involved in the BW other than those diagnosed and treated. The mixture of patients with any type of infertility, primary and secondary infertility and history of past abdominal operations could also affect the results, although statistical analysis did not show any significance in BWE, clinical symptoms and surgical findings. BE is rarely an isolated condition, and other forms of endometriosis are frequently concomitant (Vigano et al., 2009).
DME involvement presented 68% and BSE 32 of all cases with BE and infertility investigated. Secondary infertility, back pains, micturition problems and number of abortions can be considered as high-risk factors for BE for women of reproductive age. The severity of the peritoneal endometriosis can probably direct to meticulous intraoperative investigation for BE.
Dr Sayed El-Akhras: Performed all of the operations and collected the clinical and surgery data
Mohamed Abo-elenen: Involved in patients’ data collection, review all patients’ files, collection of data and formation of the excel file
Christiana Demetriou: Statistical analysis, editing the results, review the article
Nafissa Mohamed Amin El Badawy: Performed and review all patients’ histopathology results, writing and review section of histopathology in methods
Safinez Balami: review and editing of the article
Vasilios Tanos: Involved in the operations, study concept and design, review of patients’ data collection and preparation of the excel file, review of statistics and formation of tables, writing the manuscript and editing
No funding
There is no conflict of interest for none of the authors
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
