
Research Article | DOI: https://doi.org/10.31579/2578-8965/161
1 Sidi Mohamed Ben Abdellah University, Department of Gynécology and Obstetrics II, HASSAN II university hospital of Fez.
2 Sidi Mohamed Ben Abdellah University, laboratory of epidémiology and clinical research.
*Corresponding Author: Alpha Boubacar Conté, Sidi Mohamed Ben Abdellah University, Department of Gynécology and Obstetrics II, HASSAN II university hospital of Fez Morocco.
Citation: Alpha B. Conte., Sofia Jayi, Moutari S. Hadiza., Bineta J. Diagne., Fdili Aloui EZ., et al (2023), Correlation between ultrasound, hysteroscopy and histology in the exploration of postmenopausal metrorrhagia (about 90 cases). Single Center Study, J. Obstetrics Gynecology and Reproductive Sciences, 7(2); DOI:10.31579/2578-8965/161
Copyright: © 2023, Alpha Boubacar Conté. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 April 2023 | Accepted: 14 April 2023 | Published: 21 April 2023
Keywords: menopause; metrorrhagia; ultrasound; hysteroscopy; histology
Introduction
Postmenopausal metrorrhagia (PMMs) is a common reason for consultation in gynaecology. It may reveal, during exploration, a benign or malignant pathology that must be differentiated following a para-clinical assessment with the main pathology to eliminate being endometrial cancer. The goal of our study was to assess the correlation between ultrasound, hysteroscopy and histology in the exploration of endo-cavitary lesions when faced with PMMs.
Materials and methods:
This is a retrospective descriptive and analytic study, based on 90 patients treated for postmenopausal metrorrhagia (PMM) in the department of Gynaecology and Obstetrics II of HASSAN II teaching hospital of FES, from January 2014 to January 2017.
Results: The mean age of the patients was 59 years. The correlation of the ultrasound and hysteroscopy data showed that the ultrasound presented sensitivity, specificity, PPV and NPV equal to 100% for endometrial atrophy. For hypertrophy, these values were respectively 74%, 95%, 88%, 87.5%. For the suspicion of cancer, the sensitivity was 100%, the specificity of 98.6%, the PPV of 93% and the NPV of 96%. As for the correlation between hysteroscopy-histology on biopsy, sensitivity, specificity, PPV and NPV were respectively 96.7%, 98.3%, 96.7% and 98.3% for hyperplasia and 94%, 100%, 100% and 98.6% for suspected cancer. The hysteroscopy-histology correlation on the surgical specimen showed 100% sensitivity, specificity, PPV and NPV for polyps and leiomyomas, respectively 96%, 92%, 83.8% and 98.3% for hyperplasia’s and values of 72%, 100%, 100% and 92% for suspected cancer. The degree of performance of each means of exploration was variable according to the lesion in question of the metrorrhagia and generally, the hysteroscopy was more reliable in the exploration of the MMPs than the ultrasound: Kappa of 0.74 against 0.50.
Conclusion: Our results are consistent with the data in the literature, which attributes to hysteroscopy having a greater reliability compared to a pelvic ultrasound in the diagnosis of endo-cavitary lesions as the origin of postmenopausal metrorrhagia. An Ultrasound is the first-line examination in the exploration of PMMs, it should be coupled with diagnostic hysteroscopy and biopsy for better diagnostic accuracy.
Postmenopausal metrorrhagia (MPM) is a frequent reason for consultation and also the main warning signal for endometrial cancer. 70% of gynaecological consultations during peri or post menopause are linked to bleeding [1].
Explorations can reveal benign or malignant pathologies and the methods available to assess endometrial lesions have evolved in recent years. Transvaginal ultrasound (coupled with colour Doppler) is accessible, non-invasive and has become the gold standard in cases of MPM as part of an initial exploration, given the risk of endometrial cancer. The field of investigation has expanded in particular with the development of hysteroscopy.
The objective of our study was to evaluate the correlation between the results of ultrasound, hysteroscopy and histology in the exploration of these MPM, by evaluating for each its feasibility, sensitivity, specificity in the detection endocavitary lesions.
This is a retrospective study describing and analysing over a 3year period (from January 2014 to January 2017), 90 cases of MPM treated in the Gynaecology Obstetrics II department at the UTH Hassan II in Fez.
We defined postmenopausal metrorrhagia as any abnormal uterine bleeding occurring in a woman who had not seen menstrual blood flow for at least 12 consecutive months.
The data was collected from department registers, clinical records, operating reports and the results of the anatomopathological study.
The analysis of the results was made using the IBM SPSS version 20 software. All the quantitative variables were expressed in the form of means and their standard deviation and all the categorical variables in the form of frequency. Then, a univariate analysis was done looking for sensitivity (Se), specificity (Sp), positive predictive value (PPV), negative predictive value (NPV), and concordance. The Kappa test was used to measure the concordance between 2 independent judgments on the same endocavitary lesions. We agreed that the concordance is good if Kappa > 0.6, bad if < 0.3 and intermediate between the two.
I- Descriptive study
Epidemiology and clinical manifestation:
MPMs represent 62% of hospitalisations among postmenopausal women in the department. The average age of the patients was 59 years ± 8.148 years [47 to 92 years]. 53.4% were between 47 and 59 years old and 35.5Percentage between 60 and 69 years old.
Isolated MPMs represented the most frequent reason for consultation with a proportion of 82.20% followed by MPMs associated with pelvic pain (7.80%) and MPMs associated with leucorrhoea (5.60%). The association of pelvic pain – leucorrhoea and abdominopelvic mass represented respectively 2.20% of the reasons for consultation.
More than half of our patients had moderate obesity (57%) and 39% were overweight. The most documented medical history was hypertension in 21.10% of cases followed by Type 2 diabetes in 12.20% of cases. Hormone replacement therapy (HRT) was observed in one patient and tamoxifen treatment in 2 patients. Nulliparity was observed in 19% of cases. The average age of onset of menopause was 49.9 years ± 4.3 years (36-62 years); 3% had had an early menopause (< 40> 55 years old).
Ultrasound results:
This examination revealed endometrial hypertrophy with a thickness greater than 5 mm in 70 patients (78%), endometrial atrophy with endometrial thickness less than 5 mm in 15.5% of cases and myomas in 6.6% of cases.
The Doppler study was only specified in 4 patients among those who had an appearance with suspicion of malignancy. In these patients, neovascularization of the endometrium has been reported but without studies of the uterine artery.
Results of hysteroscopy:
Several lesions were sometimes found in the same patient. Certain procedures have been associated with hysteroscopy such as: endometrial biopsy (in 98.8% of cases), cervical biopsy in 13% of cases. The main lesions found were endometrial hypertrophy, polyps, suspected cancer, endometrial atrophy and uterine myomas with respective proportions of 34.4%, 22.2, 17.7, 15.5% and 8.8%.
Pathology: biopsy and surgical specimen
Biopsy histology revealed 15 cases of cancer (including 10 endometrioid adenocarcinomas, 2 cervical cancers and 3 other types).
The 28 cases of polyp and myomas found at hysteroscopy were resected by surgical hysteroscopy and the anatomopathological results confirmed their nature.
43.3% of the patients (39) underwent a surgical hysterectomy (HST) for therapeutic purposes and 11% underwent a diagnostic HST. The pathological results on surgical specimens are as follows: polyps (25.9%), hyperplasia with atypia (22%), endometrioid adenocarcinoma (19.4%), hyperplasia without atypia (12.9%), leiomyomas (10.9 %), cancers of the cervix (2.5%) and other types of cancers (6.4%).
Analytical study
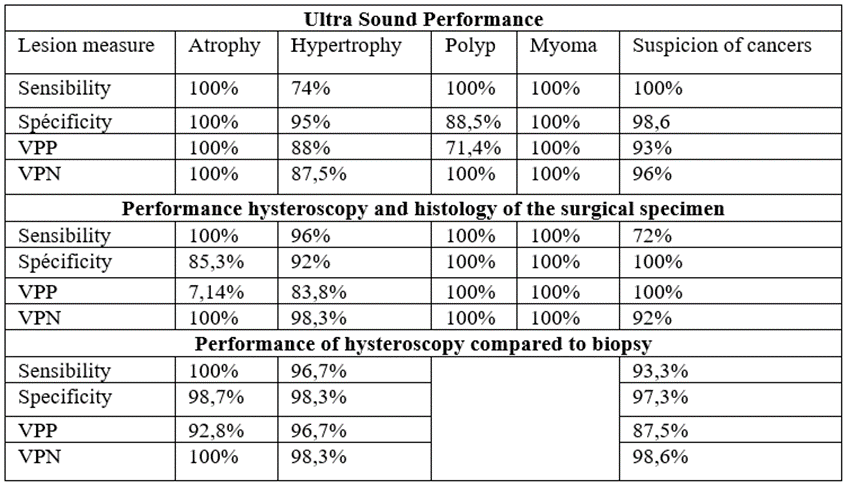
Performance study between hysteroscopy and histology on the surgical specimen (Table 1).
The hysteroscopy-histology correlation on the surgical specimen was variable according to the aetiologies, with a good performance for the majority of the lesions.
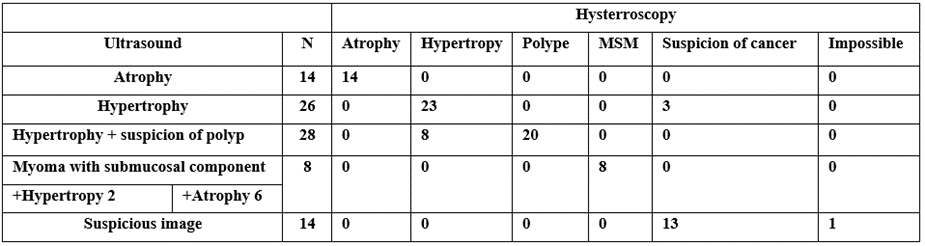
Table 2: Correlation between ultrasound and hysteroscopy
The correlation between ultrasound and hysteroscopy found a medium concordance with a Kappa of 0.50, so there is a medium concordance.
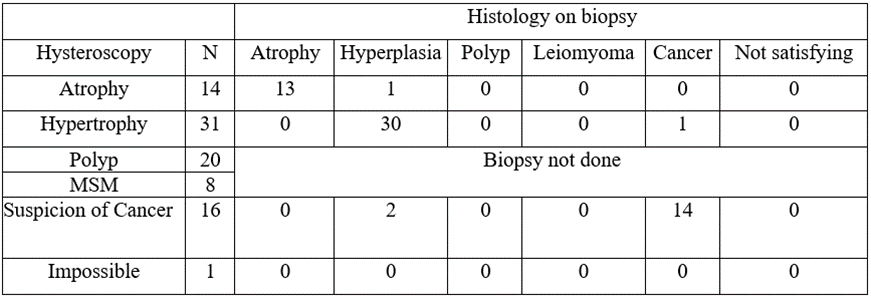
Table 3: Correlation between hysteroscopy and biopsy histology
The agreement between the results of hysteroscopy and histology on biopsy was good with a kappa value equal to 0.68.
Correlation between hysteroscopy and histology on surgical specimen (Table 4)
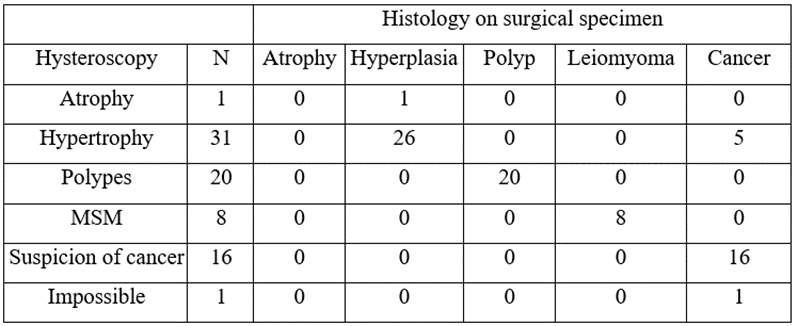
Table 4: Correlation between hysteroscopy and histology on surgical specimen
We noted a good correlation between the results of the hysteroscopy and the histology on the operating specimen with a Kappa value equal to 0.74.
In the exploration of the uterus and its annexes in the event of uterine bleeding, ultrasound is an essential first-line examination. Its contribution to diagnostic research is widely demonstrated in the literature.
In post menopause, an ultrasound is considered normal when the endometrium is thin with an endometrial thickness of less than 5 mm in a woman without hormone replacement therapy (HRT) and less than 8 mm in a woman on HRT. Hypertrophy when the thickness of the endometrium is greater than or equal to 5mm in a woman without HRT and greater than 8mm in a woman on HRT [2-4]. The thresholds considered in our study for the diagnoses are similar to those used by these authors. Ultrasounds also makes it possible to visualize the signs of malignancy such as hypervascularization, myometrial invasion.
Okaro E and Bourne T [5], report that regardless of whether HRT is taken or not, considering a threshold greater than 4mm for abnormal endometrium makes it possible to detect 96% of endometrial cancers, and 92% of pathologies endometrial (hyperplasia, polyps), with respective false positives of 39 and 19%, while in two other studies conducted by Dorum A et al, [6] and Gupta JK et al [7], the authors explain that, used alone, this threshold value is not sufficient to exclude endometrial pathology. For the latter, ultrasound alone cannot replace histological examination in the evaluation of the endometrium in the event of postmenopausal metrorrhagia. Because of habit, we resort to other examinations as soon as abnormalities are detected on the ultrasound or when we find a discrepancy between the clinical picture of the patient and the results found on the ultrasound.
One study [8] reported a small proportion (0.1 to 1%) of cases of endometrial cancer with endometrial thickness less than or equal to 4mm. Despite this observation made by the authors of this study [8], other authors consider that additional examinations are not necessary in case of thickness less than 5 mm [9,10]. We also consider that there is no need to resort to further investigations when the thickness of the endometrium is less than 5 mm because in our study, we did not find any malignant pathology for thicknesses of the endometrium. endometrium less than 5 mm.
Correlation ultrasound and hysteroscopy and histology.
Hysteroscopy (HSC) is the examination of choice for exploring endocavitary lesions suspected on ultrasound or in the absence of individualized lesions by ultrasound [11]. It makes it possible to better visualize the signs of atypia such as anarchic vascularisation, the aspects in candle spots and thus to direct the biopsies.
The comparison of the different results observed on ultrasound and hysteroscopy allows us to say that these 2 explorations are 100% concordant for the diagnosis of atrophy.
On the other hand, among the 26 cases of hypertrophy found on ultrasound, only 23 were confirmed by hysteroscopy and 3 lesions were found to be suspicious of malignancy with a concordance of 74%. This could be explained by the fact that the study of the Doppler ultrasound of the endometrium and the uterine artery in search of signs of malignancy had not been done systematically.
The ultrasound had objectified 14 suspicious images among which 13 were confirmed by the hysteroscopy since in one woman the hysteroscopy could not be done which gives us a concordance of 100%.
Among the 28 cases of hypertrophy associated with a suspected polyp objectified on ultrasound, 20 cases of polyps were confirmed on hysteroscopy and the 8 other cases had returned in favor of polyploid hypertrophy plus candle spots and this with 75
We separately studied the sensitivity, specificity, positive and negative predictive values of pelvic ultrasound and hysteroscopy in the exploration of postmenopausal metrorrhagia. The degree of performance of each means of exploration varied according to the lesion in question of metrorrhagia and in general hysteroscopy (Kappa 0.74) was more reliable in the exploration of metrorrhagia than ultrasound (Kappa 0.50). We believe that hysteroscopy may not be performed during the first episodes of MPM if the ultrasound shows endometrial atrophy, but it is important that the ultrasound is performed or supervised by an experienced operator. For endometrial hypertrophy, ultrasound must always be supplemented by Doppler in search of endometrial neovascularization plus the study of the uterine artery, which would improve the concordance between ultrasound and hysteroscopy in the diagnosis of aspects of atypia. Hysteroscopy should be performed whenever ultrasound finds an abnormality, outside of atrophy.
Conflicts of interest: No conflict of interest between the different authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
