
Case Report | DOI: https://doi.org/10.31579/2692-9759/054
1 Department of Internal Medicine, Faculty of Medicine and Health Sciences, Alneelain University, Khartoum, Sudan
2 Interventional cardiology, Ahmad Gasim Cardiac Centre, Ahmad Gasim Hospital, Khartoum North, Sudan
3 Sudan Medical Specialization Board (S.M.S.B), Internal Medicine Council
4 Medical Biochemistry and Molecular Biology, Khartoum, Sudan.
*Corresponding Author: Hayder A Giha, Medical Biochemistry and Molecular Biology, Khartoum, Sudan.
Citation: Osman Al-Sayed Osman Alamin, Omer Amir, Hayder A Giha (2022) Correlates and Severity of Left Ventricular Hypertrophy in Type 2 Diabetes Patients in an Afro-Arab-cross Ethnic Community. Cardiology Research and Reports. 4(4); DOI: 10.31579/2692-9759/054
Copyright: © 2022 Hayder A Giha, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2022 | Accepted: 05 April 2022 | Published: 22 April 2022
Keywords: T2DM; left ventricular hypertrophy; left ventricular mass index; relative wall thickness; afro-arab ethnicity
Background: The cardiovascular (CV) diseases, including left ventricular hypertrophy (LVH) are major causes of morbidity and mortality in T2DM. The LVH is associated with ventricular arrhythmias, ischemic heart disease (IHD), heart failure and sudden death. Although the LVH is frequent in T2DM, screening for this disorder is frequently done.
Material and Methods: In this study, 120 Sudanese T2DM patients were recruited, (70 with and 50 without LVH) from four cardiac centers in Khartoum, the latter is inhabited by most of the Sudanese Afro-Arab ethnic groups. Clinical data were obtained from almost all patients together with measurement of glycemic and renal parameters. Echocardiography was performed for each patient, the left ventricle geometry components including the relative wall thickness (RWT) were estimated and the left ventricle mass index (LVMI) was calculated.
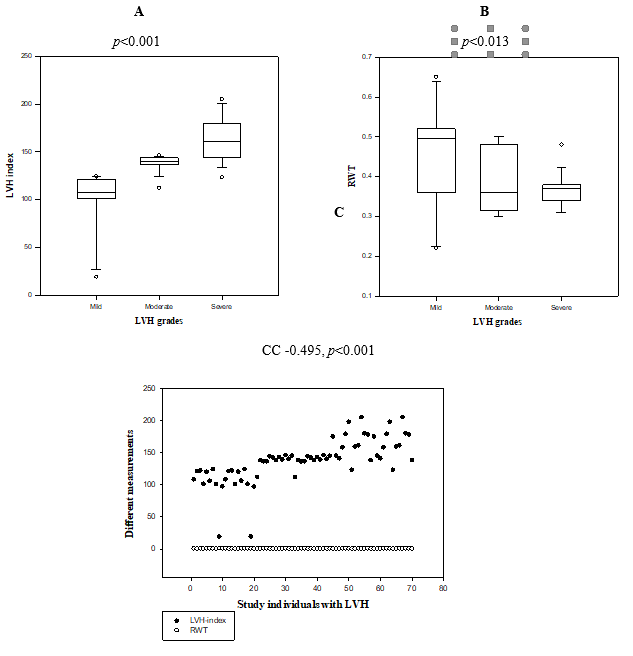
Results: The commonest LVH type was eccentric (65.7%), and grade was severe (37.1%), and both were strongly associated, p<0.001, while the frequency of the mild LVH was 28.6%. Out of 10 tested variables only HhA1c (p<0.001), urea (p=0.039) and creatinine (p=0.043) were significantly associated with LVH, while the sex, age, T2DM duration, smoking, obesity, random and fasting blood glucose were not. Moreover, the LVMI was positively correlated with HbA1c (CC0.188, p<0.039), and negatively with RWT (CC-0.495, p<0.000). Finally, significantly higher number of patients with IHD (p=0.038) and cerebral complications (p=0.014) had LVH.
Conclusion: In this unique setting of interethnic cross, the results suggest that more genetic than environmental factors could be involved in diabetic LVH development.
T2DM Type 2vDiabetes mellitus
LVH Left ventricular hypertrophy
LVMI Left ventricle mass index
IHD Ischemic heart disease
CNS Cardiovascular
PVD High density lipoprotein
FBG Fasting plasma glucose
RBG Random plasma glucose
MW Mann-Whitney Rank Sum Test
KW Kruskal-Wallis One Way Analysis of Variance
on Ranks
c2 Chi-square
RWT Relative wall thickness
IR Insulin resistance
IDF International Diabetes Federation
2H-OGTT 2-hours oral glucose tolerance test
IVS Interventricular septal thickness
BMI Body mass index
AV One Way Analysis of Variance
OHA Oral hypoglycemic agents
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by hyperglycemia due to impaired insulin secretion, insulin resistance (IR), or both. The DM is proving to be a global public health burden, according to the latest 2019 data from the International Diabetes Federation (IDF), approximately 463 million adults had DM [1], this number is expected to increase by another 200 million by 2040 [2]. Type 2 diabetes mellitus (T2DM) makes up about 85-90% of all DM cases [1]. The prevalence and incidence rates of DM in Sudan, as in many other low-income countries, are increasing to epidemic levels, leading to emergence of a public health problem of major socio-economic impact [3,4]. In Sudan, DM is associated with poor glycemic control, high prevalence of complications, and low quality of life [5,6]. As well as, DM is the commonest cause of hospital admissions due to a non-communicable disease in Sudan, with an overall increased age-adjusted mortality and reduced life expectancy of about 5–10 years [7].
It is well established that various left ventricle (LV) abnormalities are strongly promote cardiac disease and death, in particular the left ventricular hypertrophy (LVH) and LV systolic dysfunction (LVSD) [8]. Impaired long axis contraction of the LV may also be associated with increased mortality. Furthermore, LV diastolic filling abnormalities has been shown to place an individual at an increased cardiovascular (CV) risk and is associated with impaired exercise tolerance [9]. The LVH is a condition in which there is an increase in LV mass, either due to an increase in wall thickness or due to left ventricular cavity enlargement, or both. Most commonly, the LV wall thickening occurs in response to pressure overload, and chamber dilatation occurs in response to volume overload [10]. Hypertension and aortic valve stenosis are the most common causes of LVH, in both conditions; the heart is contracting against an elevated after-load leading to concentric LVH as a result of an abnormal increase in LV myocardial mass [11]. Increased filling of the LV leads to diastolic overload, which is the underlying mechanism for eccentric LVH in patients with aortic or mitral regurgitation as well as in the case of dilated cardiomyopathy [10,11].
In LVH, the sustained increase in wall stress along with cytokine and neuro-activation stimulates the development of myocardial hypertrophy or increasing muscle thickness and deposition of the extracellular matrix [11], with concomitant development of myocardial fibrosis. Initially, fibrosis is clinically manifested by diastolic dysfunction, but systolic dysfunction also develops with progressive disease.
The DM is associated with LVH, LV diastolic dysfunction, LV systolic dysfunction and cardiac autonomic neuropathy [12,13]. A large proportion of patients with T2DM whom are not known to have a primary CV disease, have LVH [14], and the regression of LVH by pharmacological intervention is associated with an improvement in prognosis [15], which are objective clues for the link between DM and LVH. The IR, which frequently accompanies T2DM, is reported to be associated with LVH [16]. Moreover, the T2DM and IR are closely associated with obesity.
The complications of T2DM are common and largely account for the excess morbidity and mortality associated with this disease. As such routine screening of asymptomatic patients with T2DM for retinopathy, nephropathy and neuropathy is recommended. However, the DM is a major risk factor for ischemic heart disease (IHD), cardiomyopathy, and congestive heart failure, which are all the most important causes of morbidity and mortality in T2DM, accounting for approximately half of total mortality [17]. T2DM is associated with a high prevalence of hypertension, dyslipidemia, and microalbuminuria, which are all known as independent CV risk factors. Even in populations with low CV risk, DM is associated with an increased incidence of CV death [18].
Genetic and ethnic difference in susceptibility to the different DM complications is well known. The Sudanese are relatively heterogeneous population with marked cross–ethnic breed, due to the intermarriage between different tribes unlike the case in the Arab, African or American societies where there are clear ethnic segregation as in USA [19] and sub-Saharan Africans [20], and familial segregation (consanguinity) as in Arabic settings [21]. In Sudan the original Africans have frequent inter marriage with the Arabs and other ethnicities [22].
The LVH is a strong predictor of CV disease among T2DM patients. The objective of this study was to determine the type and severity of LVH in T2DM as well as the risk factors, including the association with other diabetic complication, but in a different setting of patients with different genetic complexion.
Study design and area
This is a descriptive multicenter cross-sectional hospital-based study, conducted in Omdurman Teaching Hospital, Alshab Teaching Hospital, Ahmed Gasim Hospital and Alsalam Cardiac Center, in the period between April and August 2021.
Study population
The study subjects, men and women, are adult Sudanese patients, aged between 30-85 years and known to have T2DM. All diabetic patients referred from diabetic clinics or came for CV checkup to the above mentioned national cardiac centers, presented during the study period and accepted to participate in this study, were included. The exclusion criteria were; hypertension, aortic stenosis, hypertrophic obstructive cardiomypathy, severely ill patients and professional athletics.
The T2DM diagnosis in Sudan is based on either the estimation of plasma glucose [fasting plasma glucose (FPG), 2-hours oral glucose tolerance test (OGTT) and random plasma glucose (RBG)] or HbA1c. For diagnosis of T2DM the following were nationally approved: a FPG of ≥ 126 mg/dL (7.0 mmol/L), 2-h OGTT ≥ 200 mg/dL (11.1 mmol/L), RBG ≥ 200 mg/dL (11.1 mmol/L) or HbA1c ≥ 6.5% (48 mmol/mol), along with symptoms of hyperglycemia/DM. The HbA1c has also been accepted for T2DM diagnosis [23]. However, all study subjects were known to be T2DM patients.
Echocardiogram: According to the American Society of Echocardiography, the echocardiogram is the test of choice in diagnosis of LVH. Its sensitivity is significantly higher than ECG, and the test can also detect other abnormalities such as left ventricular dysfunction (systolic as well as diastolic) and valvular heart disease. Cardiac ultrasound utilizes transthoracic or transesophageal positioning of the transducer to measure the end-diastolic interventricular septal thickness (IVS), LV internal diameter, and posterior wall thickness. From these measurements and the patient’s height and weight, the LV mass index was determined. The LVH was diagnosed when LV mass index (LVMI) was >115 g/m2 in men and >95 g/m2 in women. The LVMI (LVM [left ventricular mass] normalized for body surface area or height) is calculated using the following equation: LVMI = LVM/body surface area. The LVM = 0.8 [1.04 (LVEDD + IVSd +PWd)3 - LVEDD3)] + 0.6 (Devereux et al'2000 [24]). The LVH were categorized according to the Relative Wall Thickness as follow: RWT= Posterior wall thickness x 2 / LV internal diameter at end-diastole. Based on RWT, and the LVMI, the LVH can be categorized into 2 types; concentric hypertrophy (increased LVMI and RWT more than 0.42) or eccentric hypertrophy (increased LVMI and RWT less than or equal to 0.42) [11].
Data collection tools
Data was collected through structured questionnaires consisting of the following parameters: demographic, social, clinical, therapeutic and laboratory investigations.
The LVH was the dependent variable, while the independent variables were; demographic data (age, gender, BMI), smoking, T2DM duration, diabetic complications and the laboratory variables (blood glucose, HbA1c, urea, creatinine). Data was analyzed by using a computer program Sigma Stat software, p value was considered as significant at level <0>
Ethical consideration
An ethical approval was obtained from Sudan medical specialization board (SMSB). Data used anonymously by using identity numbers to protect patient’s identity. An oral informed consent was obtained from each patient.
Characteristics of the study subjects
As seen in (Table 1), 120 T2DM patients were enrolled in this study, 50 patients without and 70 patients with LVH. Overall, 61.7% (74) were males and 38.3% (46) were females, their mean age was 59.8±11.3, (range 30.0-85.0), and 23.3% (28) of all the patients were smokers. The mean of their BMI was 28.8± 4.1, 20.0 - 39.0 kg/m, with 45% (54) were considered as obese (data not shown). The mean duration of their DM was 12.4± 7.1 (range 1.0 - 30.0) years. Most of the patients (61.7%, 74) were using oral hypoglycemic agents (OHA), 31.7% (38) insulin, 5% (6) both OHA and insulin and 1.7% (2) were on diet control (Table 2)
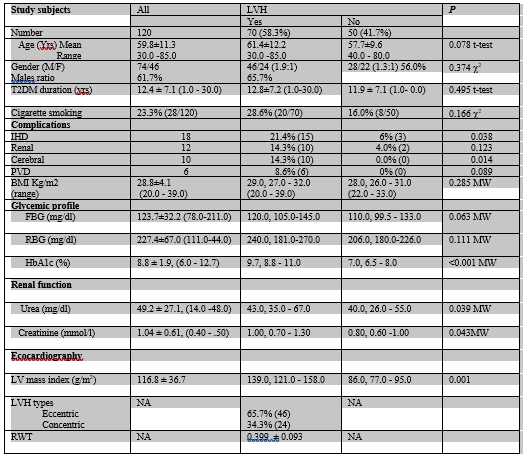
Clinical and laboratory profiles: The frequencies of the diabetic complications were as follows; ischemic heart disease (IHD) 15% (18); renal disease 10% (12); central nervous system (CVS) disease 8.3% (10); and peripheral vascular disease (PVD) 5% (6) (Table 4).
The biochemical tests’ results were as follows; mean FBG was 123.7 ± 32.2 (range 78.0 - 211.0) mg/dl, RBG was 227.4 ± 67.0 (range 111.0 - 444.0) mg/dl, and mean of HbA1c was 8.8 ± 1.9 (range 6.0 - 12.7). For the renal function tests, the mean plasma level of urea was 49.2 ± 27.1 (14.0 -148.0) mg/dl and creatinine was 1.04 ± 0.61 (range 0.40 - 4.50) mg/dl (Table 1).
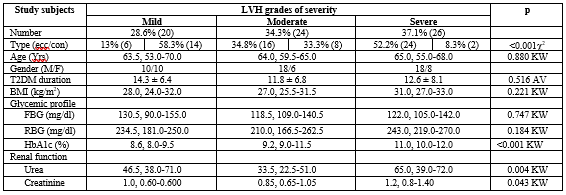
The LVH types and severity in T2DM: Out of 120 patients with T2DM, 58.3% (70) had LVH (cases) and 41.7% (50) had no LVH (control). Based on RWT, the prevalence of the eccentric LVH was 65.7% (46) and that of the concentric LVH was 34.3% (24), while the mean RWT was 0.399 ± 0.093 (Table 1). The LVH was severe in 37.1% (26/70) of the cases, in 34.8% (24/70) was moderate and in 28.6% (20/70) it was mild (Table 3). The mean of the LVHI in all study subjects was 116.8 ± 36.7 g/m2, and it was139.0, 121.0 - 158.0 in the cases and 86.0, 77.0 - 95.0, in the controls, p 0.001 (Table 1).
KW = Kruskal-Wallis One Way Analysis of Variance on Ranks
AV=One Way Analysis of Variance
The T2DM patients with and without LVH were of comparable sex distribution although males were more dominant in the former group, male to female ratio of 1.9:1 vs. 1.3:1, respectively, p 0.374 c2. The two groups had comparable mean age, 61.4±12.2 vs. 57.7±9.6 yrs., respectively, p 0.078. Moreover, both groups had comparable, T2DM disease duration (p 0.495), frequency of cigarette smoking (p 0.166), and BMI (p 0.285). The frequency of obesity (BMI ≥30kg/m) is comparable between the two study groups, 59.3% vs. 40.7%, p1.00 (Table 2). Also the usage of OHG (oral hypoglycemic drugs) and insulin was not significantly different between the patients with and without LVH, p 0.815 (Table 2). Of the T2DM complications, the prevalence of the renal (p 0.123) and PVD (p 0.089) diseases, were also comparable between the two groups. The biochemical profiles showed that the RBG (p 0.111) and FBG (p 0.063) were not significantly different between the T2DM patients with and without LVH, (Table 1). However, the prevalence of the IHD and renal complications were significantly higher in patients with LVH, p 0.038 and p 0.014, respectively. As well as, the HbA1c (p <0>
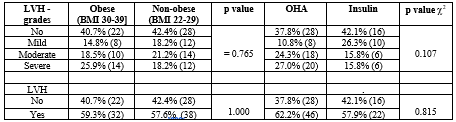
Note: 6 patients (5%) used both OHA and insulin, and 2 patients (1.7%) were on diet control, 2 from the former had mild LVH, while the rest (6) didn’t had LVH.c2= Chi-square, LVH= left ventricular hypertrophy, BMI= body mass index, OHA= oral hypoglycemic agent
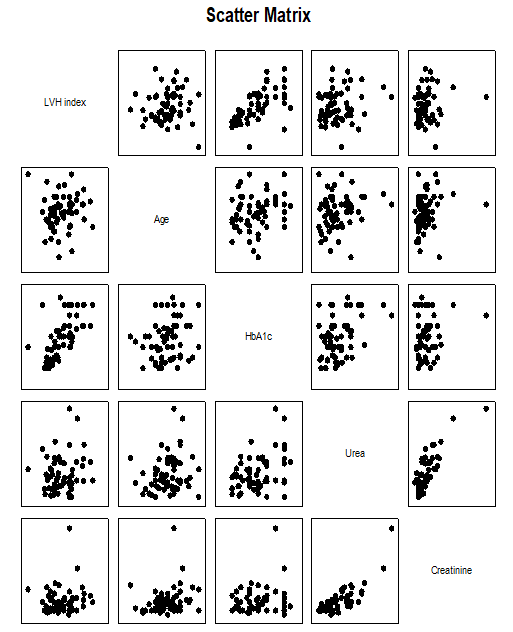
For the variants which were significantly different between the study groups, the correlation analysis showed significant positive correlations between the LVMI and HbA1c, CC 0.641, p< 0>
correlated with the former variables which were all significantly positively inter-correlated (Figure. 1). The other variables, the disease duration (p 0.608), BMI (p 0.458), RBG (p 0.234) and FBG (p 0.845) were not correlated with the LVMI.
Finally, 52.2% (24) of the patients with eccentric LVH had severe, 34.8% (16) had moderate and only 13% (6) had mild LVH, while 8.3% (2) of patients with concentric LVH had severe, 33.3% (8) had moderate and 58.3% (14) had mild LVH, p <0>
As seen in (Table 3, and Figure. 2), limiting the analysis to T2DM patients with LVH only, the prevalence of the three grades of LVH, mild, moderate and severe were 28.6% (20), 34.3% (24), and 37.1% (26), respectively. The three subgroups had similar median age distribution, 63.5, 53.0-70.0; 64.0, 59.5 - 65.0; 65.0, 55.0 - 68.0 years, respectively, p 0.880, mean T2DM disease duration, 14.3 ± 6.4; 11.8 ± 6.8; and 12.6 ± 8.1 years, respectively, p 0.516, and median BMI, 28.0, 24.0-32.0, 27.0, 25.5-31.5, and 31.0, 27.0 - 33.0 kg/m2, respectively, p 0.221. Among the glycemic parameters (RBG, FBG, and HbA1c), only higher HbA1c was significantly associated with LVH severity, 8.6, 8.0- 9.5; 9.2, 9.0 - 11.5; and 11.0, 10.0 - 12.0, respectively, p <0>
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
