
Case Report | DOI: https://doi.org/10.31579/2690-4861/635
1OGBUZ "Bratsk Children's City Hospital", Irkutsk Region, Russia.
2Irkutsk State Medical University, Russia.
*Corresponding Author: M.F. Ermachenko, Ogbuz
Citation: M.F. Ermachenko., R.A. Ivanov., L.I. Sergeeva., R.M. Khakimov., O.S. Klimova, (2025), Postural Ventricular Tachycardia from Peripherally Inserted Central Catheter Line Placed Using a Tip Confirmation System, International Journal of Clinical Case Reports and Reviews, 23(2); DOI:10.31579/2690-4861/635
Copyright: © 2025, M.F. Ermachenko. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2025 | Accepted: 31 January 2025 | Published: 14 February 2025
Keywords: sepsis; meningoencephalitis; trepanation
Control of bone hemostasis using bone wax is convincing. Around the prolapsed brain from the previous trepanation, a bone bridge was formed, which was also resected using Kerrison pliers. In the opened field, cyanotic, slightly protruding outward relative to the bone window, dura mater is visible, with traces of brain detritus, thrombotic masses and purulent film. The dura mater was opened for the purpose of subsequent sail plasty using the Xeno Dura implant, to provide a larger useful volume of the intracranial cavity for the purpose of subsequent prevention of wedging.
Purulent meningitis and purulent meningoencephalitis constitute a significant part (20-40%) in the structure of neuroinfections in children and the relevance of their study is due to the severity of the course, high frequency of disabling consequences and fatal outcomes (8-39%) [1,2,3,4,5,7,9,10]. According to statistics, bacterial meningitis is diagnosed in 3-10 people per 100 thousand population worldwide [1, 2, 6,9,10]. Bacterial purulent meningitis and meningoencephalitis are the most severe forms of infectious pathology of the central nervous system in children [3,4,6,8,15]. The leading role in their etiological factor is played by such pathogens as meningococcus, pneumococcus, streptococcus and Haemophilus influenzae [1,2,6,9,10]. These pathogens can affect not only the pia mater, but also the brain tissue. A high protein content is noted in the cerebrospinal fluid with the formation of fibrin capsules, in which the pathogen is preserved for a long time [1,6,7]. As a result, the disease takes on a severe course with frequent development of encephalitic syndromes, protracted and recurrent course, high frequency of residual effects [1, 2,6,8,9,10]. Children with purulent meningoencephalitis and intracranial empyema often have a severe, septic course of the disease, with a high frequency of disability and mortality [6,7,8,9,10]. Often such patients have to use combined treatment, combining conservative methods with surgical [1,3, 5,6,9,10].
The aim of the work is to analyze a rare case of combined treatment of sepsis against the background of purulent meningoencephalitis in an adolescent in the intensive care unit.
Material and methods. Under our observation in the intensive care unit of the Regional State Budgetary Healthcare Institution "Bratsk Children's City Hospital" there was a patient B., 14 years old, with sepsis that arose against the background of purulent meningoencephalitis, which required combined treatment (a combination of conservative and surgical tactics).
It is known from the anamnesis that she fell ill acutely, with a temperature rise to 39-40 0 C , headache, sore throat, rhinorrhea , and was ill for 6 days. The girl took antipyretics on her own. About 9 days ago, she fell during training, hitting her right parietal-temporal region. She did not lose consciousness. She is not registered with pediatric specialists. She has been vaccinated according to her age. Her allergy history is not complicated. On September 12, 2024, due to deterioration of her condition, impaired consciousness, increased headache, and the appearance of repeated vomiting, the ambulance team hospitalized her in the intensive care unit of the Bratsk Children's City Hospital with DS : Acute secondary purulent meningitis, severe, of unspecified etiology. The patient's condition on admission is severe. Conscious, very lethargic, hypodynamic. Consciousness level assessment according to the GCS is 14 points (stupefaction). Verbal contact is possible, answers questions correctly. Complains of weakness. Speech is inhibited. The face is symmetrical, the tongue is in the oral cavity along the midline. Pupils D > S , photoreactions are preserved. Meningeal symptoms (rigidity of the occipital muscles, Kernig's sign) are positive. Muscle tone is moderately diffusely reduced.
The skin is pale, gray in color, warm, dry. In the right temporoparietal region there is a subcutaneous hematoma about 3 cm in diameter. Acrocyanosis. Low skin turgor. Sunken eyes. Guedel's test 4 sec. The mucous membrane of the lips is dry, pale. The pharynx is hyperemic. The tongue is dry, coated with a white coating. The subcutaneous fat layer is poorly developed. Body temperature is 39.5 0 C. There is no shortness of breath. Percussion over the entire surface of the lungs - a clear pulmonary sound. In the lungs, breathing is harsh, conducted along all fields, there are no wheezing. Respiratory rate is 20 in min., SpO2 98%. Heart sounds are muffled, rhythmic. Pulse on a. radialis is of satisfactory quality. HR 129 beats. in min. BP 112/64 mm Hg.
The abdomen is sunken, painless on palpation. The liver and spleen are not enlarged.
09/13/2024 deterioration of condition to extreme severity. Consciousness Coma I - II. Transferred to the Newport ventilator in SIMV mode, FiO 2 30%, f 18 per min, PIP 22 mbar PEEP 5 mbar. The consultation made a diagnosis, taking into account the MSC examination: Basic: Severe sepsis of unspecified etiology.
Acute purulent meningoencephalitis, severe, of unspecified bacterial etiology.
Complication: Toxic exicosis of 1-2 degrees of severity. Infectious toxic shock of 1-2 degrees of severity.
Supplement. Diagnosis: Hygroma of the right parietal -temporal region? Empyema of the brain? Hematoma? (based on the results of MSCT of the brain).
A consultation with a neurosurgeon was held to decide on urgent surgical intervention.
On September 13, 2024, under combined endotracheal anesthesia, the following operation was performed: decompression trepanation of the skull of the right parietal-temporal region, opening of the subdural empyema.
When the dura mater was opened under pressure, liquid white pus was released. A bacterial culture was taken. The burr hole was widened to 4.0 x 4.0 cm. The dura mater was cut crosswise. Up to 150.0 ml of pus was evacuated. Two drains were installed in the subdural space for outflow through separate punctures of the skin. The subdural space was sanitized with a physiological solution until the waters were clear. Brain pulsation was preserved.
The condition after the surgery remained extremely serious. Artificial ventilation, drug-induced sleep, and intensive therapy were administered.
Control MSCT of the head on 09/16/2024 with clarification of the main DS : Bacterial sepsis, severe, unspecified etiology.
Acute purulent meningoencephalitis, severe, of unspecified bacterial etiology.
Infectious toxic shock grade 1-2.
Complication: Subdural empyema of the right parietal temporal region (surgery 09/13/2024)
Competing diagnosis: Child abuse syndrome? Closed craniocerebral injury? Subdural hematoma? Intracranial hematomas?
Complication: Suppuration of the subdural hematoma with transition to subdural empyema of the right parietal temporal region.
On September 18, 2024, under combined endotracheal anesthesia, a repeat surgical intervention was performed: Decompression infratemporal craniotomy on the right, dura mater plastic surgery.
The bone stage of trepanation was performed with subsequent intraoperative maximum accessible infratemporal decompression, as a result the bone window was about 12x10 cm. Control of bone hemostasis using bone wax is convincing. In the opened field, cyanotic, slightly protruding outward relative to the bone window, dura mater is visible, with traces of brain detritus, thrombotic masses and purulent film. The brain prolapse from the previous trepanation was revised , encephalotomy was partially performed , brain detritus, necrotic brain tissue were removed, surgical cellulose was laid out for hemostasis. A smear was taken from the brain area for bacteriological culture. The brain tissue itself began to slightly reflect the transmitted pulsation.
The department conducted an examination:
UAC dated September 12, 2024 ESR – 15 mm/h; Hb – 123 g/l; er – 4.3 X 10 12 ; Le – 14.0 X 10 9 ; n – 50; s – 44; l – 4; m – 2; e – 0; yu – 0; thrombus. – 178 X 10 9/l
OAC from 9/13/2024. SOE – 41 mm/h; Hb – 103 g/L; er – 3.6 X 10 The – 8.7 X 10 9 ; p – 46; s – 27; l – 6; m – 5; e – 0; y – 16; thrombus. – 93 X 10 9/l
OAC from 09/17/2024. SOE – 57 mm/h; Hb – 96 g/L; er – 3.3 X 10 The – 26.7 X 10 9 ; p – 6; s – 72; l – 13; m – 4; e – 0; y – 3; thrombus. – 161 X 10 9/l
UAC dated September 21, 2024 ESR – 70 mm/h; Hb – 92 g/l; er – 3.11 X 10 12 ; Le – 15.3 X 10 9 ; n – 9; s – 71; l – 12; m – 7; e – 1; yu – 0; thrombus. – 494 X 10 9/l
Biochemical blood test.
12.09.2024 AlT– 10.9 u / l ; AsT – 11.7u/ l ; total protein - 69.8 g/l; urea - 2.29 mm/l; creatinine 56 mm/l; c-Reactive Protein – 214; sugar - 8.8 mmol/l; bilirubin - 14 μm/l; LDL-C - 1.53 mmol/l; LPVP - 0.23 mmol/l;
17.09.2024 AlT u / l – 52.3; AsT – 58.9 u / l ; total protein - 69.6 g/l; urea - 6.3 mm/l; creatinine 47.4 mm/l; c-Reactive Protein - 68.8; sugar - 7.9 mmol/l; bilirubin - 13 μm/l;
21.09.2024 AlT u / l – 14.8; AsT – 46.3 u / l ; total protein - 67.7 g/l; urea - 7.8 mm/l; creatinine 45 mm/l; sugar - 7.2 mmol/l; bilirubin - 11 μm/l;
Contents of purulent discharge from the wound (craniotomy 09/13/2024) - streptococcus sp . sensitive to meropenem , vancomycin.
Blood for sterility from 09/13/2024. - negative .
Urine for sterility from 09/13/2024. - negative .
Bronchial lavage for microflora from 09/13/2024. - streptococcus viridans 10 x4 .

Figure 1: First trepanation of the skull. After opening the dura mater, the purulent discharge is cleaned.
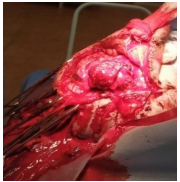
Figure 2: Repeated craniotomy, the bone window was about 12x10 cm. A section of the prolapsed brain is visible. The brain prolapse from the previous trepanation has been revised, partially completed. encephalotomy, brain debris removed.
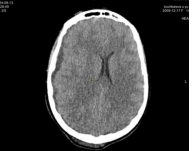
Figure 3: MSCT of the brain from 09/13/2024. Displacement of midline structures to the left. MSCT signs of subdural hygroma in the frontal-parietal-temporal region on the right. Suspected subarachnoid hemorrhage, with the presence of a hyperdense component in the frontal region on the right.
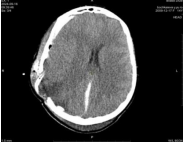
Figure 4: MSCT of the brain from 09/16/2024. Condition after surgery. Displacement of midline structures to the left (not distinct, weakly expressed positive dynamics). MSCT signs of subarachnoid hemorrhage. Additional hyperdense component in the cranial cavity in the frontal-parietal region on the right (subarachnoid hemorrhage? subdural hemorrhage?). MSCT signs of cerebral edema. MSCT picture of prolapse of the caudal contour of the cerebellar tonsils under the foramen magnum.

Figure 5: MSCT of the brain from 09/17/2024. In the parietal and occipital regions and in the frontal-parietal-temporal region on the right, an increase in the volume of superficial soft tissues is noted, due to the presence of an additional component of about 19H in their projection, in the frontal-parietal-temporal region on the right, also with the presence of a component of up to 76H.
In the parietal bone on the right, a postoperative defect of about 4.59 x 3.57 cm is noted. The median structures of the brain are shifted to the left by about 0.55 cm. Smoothing of the convex grooves is noted.

Figure 6: MSCT of the brain from 09/20/2024. Condition after surgery. Dynamics show expansion of the postoperative defect in the bones of the skull on the right. Displacement of the midline structures is not noted at the time of the study.
The patient was treated in the anesthesiology and intensive care unit of the Bratsk Children's City Hospital for 11 days. The development of sepsis and meningoencephalitis was facilitated by two factors: a head injury during training (hematoma in the right temporoparietal region) and bacterial nasopharyngitis with penetration of streptococcal infection under the dura mater. In addition to conservative treatment (transfer to Newport mechanical ventilation in SIMV mode , FiO 2 30%, f 18 per min, PIP 22 mbar PEEP 5 mbar 8 hours after admission; antibacterial therapy: meronem 120 mg/kg/day intravenously; vancomycin 40 mg/kg/day intravenously; immunocorrective therapy _ immunovenin 50 ml intravenously No. 5; infusion therapy (infusion of colloids and crystalloids, fresh frozen plasma, EMOLT); Hormonal therapy - dexamethasone 0.1 mg/kg/day intravenously - anti-edema therapy: mannitol 15% - 0.5 g/kg intravenously by drip + lasix 1% - 2.0 ml; for the purpose of synchronization with mechanical ventilation: sibazon, sodium oxybate 20P mg/kg/hour, fentanyl 0.005% 2 mcg/kg/hour via infusion pump; intravenous omeprazole 40 mg; intravenous etamsylate 12.5% - 2.0 ml; inotropic support with norepinephrine 0.12 mcg/kg/hour, metrogyl 7.5 mg/kg 3 times a day intravenously; fluconazole according to the regimen 1st day 6 mg/kg/day, 2nd day 3 mg/kg/day in connection with long-term antibacterial therapy, and surgical treatment was also performed twice:
Operation #1, September 13, 2024. Decompression trepanation of the skull in the right parietal-temporal region, opening of the subdural empyema.
Under combined endotracheal anesthesia, an arcuate incision was made in the right parietal-temporal region. A burr hole was made, when the dura mater was opened under pressure, liquid white pus was released. Bacterial culture. The burr hole was expanded to a size of 4.0 x 4.0 cm. The dura mater was dissected crosswise. Up to 150.0 ml of pus was evacuated. 2 drains were installed in the subdural space for outflow through separate punctures of the skin. Sanitation of the subdural space with saline until the waters were clear. Brain pulsation is preserved.
However, despite the conservative and surgical treatment, the patient's condition remained extremely serious, which required frequent medical consultations and constant monitoring with the resuscitation and advisory center of the Irkutsk State Children's Clinical Hospital in Irkutsk. (ISCHCH). Considering that the patient's condition remained extremely serious and the symptoms of brain compression persisted, the risk of transportation to the regional hospital (threat of brain wedging), a pediatric neurosurgeon was called to the Bratsk Children's Hospital and a second operation was performed.
Operation No. 2 from September 18, 2024. Decompression subtemporal craniotomy on the right, dura mater plastic surgery.
Under combined endotracheal anesthesia, using Luer pliers and Kerrison pistol pliers , the bone stage of trepanation was performed with subsequent intraoperatively maximally accessible infratemporal decompression, as a result, the bone window was about 12x10 cm. Control of bone hemostasis using bone wax is convincing. Around the prolapsed brain from the previous trepanation, a bone bridge was formed, which was also resected using Kerrison pliers. In the opened field, cyanotic, slightly protruding outward relative to the bone window, dura mater is visible, with traces of brain detritus, thrombotic masses and purulent film. The dura mater was opened for the purpose of subsequent sail plasty using the XenoDura implant, to provide a larger useful volume of the intracranial cavity for the purpose of subsequent prevention of wedging.
prolapse from the previous trepanation was revised, encephalotomy was partially performed, brain detritus and necrotic brain tissue were removed, surgical cellulose was laid out for hemostasis. A smear was taken from the area opened after the incision of the dura mater of the brain for bacteriological culture. The brain tissue itself began to slightly reflect the transmitted pulsation. Within the surgical field, a purulent film, blood clots and brain detritus were noted on the brain tissue. A template for subsequent plastic surgery with the material " XenoDura " was cut out using sterile material.
The dura mater plastic surgery was performed partially - the brain prolapse from the previous trepanation could not be eliminated completely. The next stage is the placement of a counter- perforate subgaleal catching drainage. The drainage is connected to a passive collection system.
After the combined treatment, the patient’s condition went from extremely serious to severe and transportable.
When analyzing the test results, it was revealed that the patient had postoperative anemia (a decrease in Hb from 123 g/l to 92 g/l), against the background of compensation for blood loss with a single-group EMOLT.
There was an increase in ALT to 52.3 u / l , AST to 58.9 u / l , a decrease in total protein to 67.7 g/l, an increase in C - reactive protein to 214, and urea, creatinine, and bilirubin levels within normal limits.
Changes in microelement and coagulogram parameters were also noted, which required infusion correction. In the general urine analysis, changes were also noted in the form of the appearance of protein up to 0.35 g/l and ketone bodies. The procalcitonin test was at the level of 0.5 – 2 ng /ml.
Streptococcus was isolated from a postoperative wound (cranial trepanation on 09/13/2024). sp . sensitive to meropenem, vancomycin. Bronchial lavage for microflora from 09/13/2024. - streptococcus viridans 10 x 4.
Ultrasound of internal organs, echocardiography, and ECG also showed changes caused by the acute stage of the purulent process and intoxication.
In Fig. 1 – craniotomy, sanitation of purulent discharge from under the dura mater. In Fig. 2 – repeated craniotomy, the bone window was about 12x10 cm. A section of the prolapsed brain is visible. The brain prolapse from the previous trepanation has been revised, partially performed encephalotomy, brain debris removed.
In the series of MSCT images Fig. 3, Fig. 4, Fig. 5, a shift of the midline structures of the brain to the left is visible, in Fig. 6, no shift of the midline structures of the brain is noted.
Thus, in the intensive care unit of the Bratsk City Children's Hospital, it was possible to stabilize the patient's condition.
At the time of transfer: the patient's condition is severe, with positive dynamics. The level of consciousness is coma 1. According to the PSSM 17 points, according to Glasgow 6, according to FOUR - 9 points. In response to loud speech, the patient tries to open his eyes slightly, nods his head. Tries to stick out his tongue, squeeze his hand (squeezes the right one better). When asked to move his legs, he bends the right leg better. He breathes into the ventilator. Reflexes with TBP, corneal and corneal reflexes are present. Both pupils react weakly to light, they are the same. Muscle tone is diffusely reduced. No seizures were noted. Infusion of 0.005
Despite the development of sepsis and purulent meningoencephalitis, with a high probability of a fatal outcome, the patient was brought from a state of extreme severity to a state of severe transportability with the help of the correct medical tactics (a combination of conservative and surgical treatment) and transferred for follow-up treatment to a 3rd level institution in the Irkutsk Regional Children's Hospital. The patient recovered, underwent a course of neurological rehabilitation and is awaiting surgery: plastic surgery of the trepanation hole.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
