
Review Article | DOI: https://doi.org/10.31579/2693-7247/044
1Assistant professor of Medicine, Unit-3, Lahore General Hospital / PGMI / AMC. Pakistan.
2University of Lahore, Pakistan.
3Associate Professor & Head of Department of Urology, University College of Medicine, University of Lahore
*Corresponding Author: Kashif Aziz Ahmad, Assistant professor of Medicine, Unit-3, Lahore General Hospital / PGMI / AMC. Pakistan.
Citation: Kashif Aziz Ahmad, Saleha Akram Nizami, Muhammad Haroon Ghous. (2022) Coronavirus - Drug Discovery and Therapeutic Drug Monitoring Options, J. Pharmaceutics and Pharmacology Research, 5(2); DOI: 10.31579/2693-7247/044
Copyright: © 2022 Kashif Aziz Ahmad, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 November 2021 | Accepted: 13 December 2021 | Published: 05 January 2022
Keywords: drug discovery; therapeutic drug; COVID-19
COVID-19 is basically a medium size RNA virus and the nucleic acid is about 30 kb long, positive in sense, single stranded and polyadenylated. The RNA which is found in this virus is the largest known RNA and codes for a large polyprotein. In addition, coronaviruses are capable of genetic recombination if 2 viruses infect the same cell at the same time. SARS-CoV emerged first in southern China and rapidly spread around the globe in 2002–2003. In November 2002, an unusual epidemic of atypical pneumonia with a high rate of nosocomial transmission to health-care workers occurred in Foshan, Guangdong, China. In March 2003, a novel CoV was confirmed to be the causative agent for SARS, and was thus named SARS-CoV. Despite the report of a large number of virus-based and host-based treatment options with potent in vitro activities for SARS and MERS, only a few are likely to fulfil their potential in the clinical setting in the foreseeable future. Most drugs have one or more major limitations that prevent them from proceeding beyond the in vitro stage. First, many drugs have high EC50/Cmax ratios at clinically relevant dosages
The history of corona virus family is very old, it begins in 1965 when Tyrrell and Bynoe found that there was a virus family who damage the respiratory pathway. This virus was named as B814 in that time. It was transmitted from animals to humans. Now, in 2020 there is a virus COVID-19 which is also belongs to the family of corona virus is infected the whole world. People all around the world facing the situation of pandemic. This virus effected the whole world and do not believe in racism.
COVID-19 is basically a medium size RNA virus and the nucleic acid is about 30 kb long, positive in sense, single stranded and polyadenylated. The RNA which is found in this virus is the largest known RNA and codes for a large polyprotein. In addition, coronaviruses are capable of genetic recombination if 2 viruses infect the same cell at the same time.
The most common symptoms of COVID-19 is cold, flu, fever and infection in lungs. There are different stages in the attacking of this virus. At stage one and at the start patient just feel flu and temperature just like common cold and flu. But after seven days it becomes more worse and patient feels shortness of breath and dry cough. At advanced stage the patients become also suffered from pneumonia. There is no vaccine and antiviral therapy until now.
In this short communication we will talk about current situation of COVID-19 in Pakistan. It was basically starts from China from December 2019, when there was a person who died in Wuhan (a city of China) due to an unknown virus. What started as an epidemic mainly limited to China has now become a truly global pandemic. There have now been over 392,331 confirmed cases and 17,156 deaths, according the John Hopkins University Covid-19 dashboard, which collates information from national and international health authorities. The disease has been detected in more 196 countries and territories, with Italy, the US and Spain experiencing the most widespread outbreaks outside of China. There were 438,441 cases from which 19,650 died and 111,877 were recovered all around the world.
SARS-CoV started first in southern China and quickly spread the world over in 2002–2003. In November 2002, an irregular pandemic of atypical pneumonia with a high pace of nosocomial transmission to human services laborers happened in Foshan, Guangdong, China. In March 2003, a novel CoV was affirmed to be the causative specialist for SARS, and was in this manner named SARS-CoV. The disengagement of a novel βCoV from a patient in Jeddah, Saudi Arabia, who passed on of extreme pneumonia and multi-organ disappointment in June 2012, was first detailed in September 2012. At first named 'human coronavirus Erasmus Medical Center', the infection was later renamed MERS-CoV by global accord, and the sickness was called Middle East respiratory syn-drome (MERS). Review examination of a group of nosocomial cases in April 2012 in Jordan affirmed that MERS-CoV was likewise liable for that flare-up. In the course of recent years, MERS-CoV has kept on spreading inside and past the Middle East, and there are progressing reports of inconsistent cases and network and social insurance related groups of tainted people in the Middle East, particularly in Saudi Arabia and the United Arab Emirate. Travel-related cases and groups have likewise been progressively given an account of different mainlands. Starting at 9 October 2015, 1,593 lab affirmed instances of MERS, including 568 passings, have been accounted for to the World Health Organization.
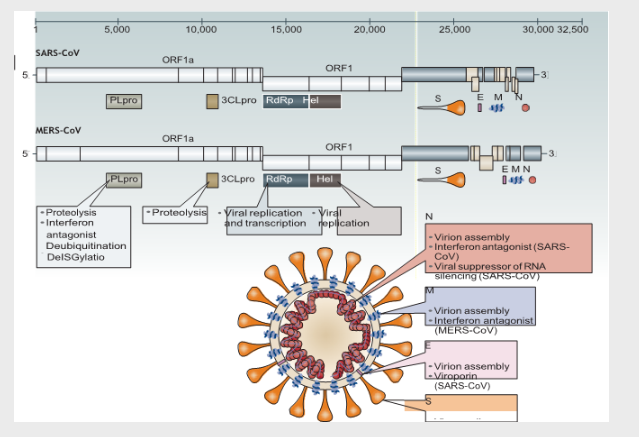
Figure 1: Genomes and structures of SARS-CoV and MERS-CoV.
Non-structural proteins Structural and accessory proteins
The typical coronavirus (CoV) genome is a single‑stranded, non‑segmented RNA genome, which is approximately 26–32kb. It contains 5ʹ‑methylated caps and 3ʹ‑polyadenylated tails and is arranged in the order of 5ʹ, replicase genes, genes encoding structural proteins (spike glycoprotein (S), envelopeprotein (E), membrane protein(M) and nucleocapsid protein (N)), poly adenylated tail and then the 3ʹ end. The partially overlapping 5ʹ‑terminal open reading frame 1a/b (ORF1a/b) is within the 5ʹ two‑thirds of the CoV genomeand encodes the large replicase poly protein 1a (pp1a)and pp1ab.
Approachesto anti-CoV drugscreening
The main two human-pathogenic CoVs known before the SARS pestilence were HCoV-229E and HCoV-OC43, which as a rule because self-constraining upper respiratory tract contaminations. Along these lines, analysts and examination offices, particularly those associated with antiviral turn of events, were underprepared when SARS-CoV out of nowhere emerged in 2003. In this manner, three general methodologies were utilized to find potential enemy of CoV treatment alternatives for human-pathogenic CoVs particularly SARS-CoV and the rising MERS-CoV.
The main way to deal with sedate revelation is to test existing wide range antiviral medications that have been utilized to treat other viral diseases by utilizing standard examines that measure the impacts of these medications on the cytopathi city, infection yield and plaque development of live and additionally pseudo composed CoVs. Instances of medications distinguished utilizing this methodology incorporate interferon alfa, interferon beta, interferon gamma, ribavirin and inhibitors of cyclophilin. These medications have the undeniable preferred position of being promptly accessible with known pharmacokinetic and pharmacodynamic properties, symptoms and dosing regimens. Nonetheless, they don't have explicit enemy of CoV impacts and might be related with serious antagonistic impacts. The second enemy of CoV medicate revelation approach includes the screening of substance libraries involving huge quantities of existing mixes or databases that contain data on transcriptional marks in various cell lines. This methodology gives quick, high-throughput screening of numerous promptly accessible aggravates that would then be able to be additionally assessed by hostile to viral tests. Different classes of medications have been distinguished in these medication repurposing programs, including numerous that have significant physiological as well as immunological impacts, for example, those that influence synapse guideline, the estrogen receptor, kinase flagging, lipid or sterol digestion, protein handling and DNA amalgamation or fix.
Nucleosides and nucleotides are the building blocks of viral nucleic acids. Medications that target nucleosides or nucleotides as well as viral nucleic acids by and large have expansive range movement against a wide scope of CoVs and different viruses. Mycophenolate mofetil is an enemy of dismissal tranquilize that represses inosine monophos-phate dehydrogenase and the union of guanine monophosphate. The dynamic compound, mycophenolic corrosive, displays antiviral action in vitro against different viruses, including hepatitis B infection (HBV), hepatitis C infection (HCV) and arbo viruses. Mycophenolic corrosive was distinguished as a potential enemy of MERS-CoV sedate utilizing high-throughput screening and has powerful enemy of MERS-CoV action in vitro122. In any case, an ensuing report in a non-human primate model demonstrated that MERS-CoV-tainted normal marmosets rewarded with mycophenolate mofetil had a more regrettable result with progressively extreme illness and higher viral loads in necropsied lung and extra pneumonic tissues than untreated creatures. Renal transplant beneficiaries who were on upkeep mycophenolate mofetil treatment additionally created serious or deadly MERS. Subsequently, the standard measurement of mycophenolate mofetil monotherapy is probably not going to be helpful for prophylaxis or treatment of CoV contaminations.
Advancement of MERS-CoV immunizations
Quick diagnostics and compelling immunizations are regularly correlative to antiviral treatment in the control of pandemics brought about by developing viruses. In spite of the fact that there has not been any new human SARS case for more than 10 years, inconsistent cases and groups of MERS keep on happening in the Middle East inferable from the diligence of zoonotic sources in endemic territories, and these cases spread to different areas. Powerful MERS-CoV antibodies are basic for intruding on the chain of transmission from creature stores and contaminated people to helpless hosts. Live-constricted antibodies, which have been recently assessed in creature models for SARS, may be related with dispersed disease in resistant traded off patients. Inactivated antibodies may be related with immunopathology during creature challenge. These are un great methodologies for MERS antibody advancement on the grounds that a considerable extent of patients with serious MERS have comorbidities or fundamental resistant bargaining conditions. Other immunization systems for MERS that utilization DNA plasmids, viral vectors, nanoparticles, infection like particles and recombinant protein subunits are being developed and some have been assessed in creature models. The accessibility of a sheltered and powerful MERS-CoV antibody for dromedary camels and non-invulnerable people at high danger of camel contact in endemic locales, for example, the Middle East and the more prominent Horn of Africa would be a significant measure for controlling the progressing pandemic.
Reasonable creature models are particularly significant for testing hostile to CoV drugs in light of the fact that the vast majority of these medications have not been utilized in people. As opposed to the set number of creature models set up for the mellow diseases brought about by HCoV-229E, HCoV-OC43, HCoV-NL63 and HCoV-HKU1, different little creature and non-human primate models have been assessed for investigations of the pathogenesis and treatment of SARS and MERS.
Despite the report of a large number of virus-based and host-based treatment options with potent in vitro activities for SARS and MERS, only a few are likely to fulfil their potential in the clinical setting in the foreseeable future. Most medications have at least one significant impediments that keep them from continuing past the in vitro stage. In the first place, numerous medications have high EC50/Cmax proportions at clinically significant measurements. Instances of such medications incorporate cyclosporine, chlorpromazine and interferon alfa. Second, some have extreme symptoms or cause immunosuppression. For instance, the utilization of high-portion ribavirin might be related with haemolytic iron deficiency, neutropenia, teratogenicity and cardiorespiratory trouble. MERSCoV-contaminated basic marmosets rewarded with mycophenolate mofetil built up a deadly disease with significantly higher viral burdens in their lungs and extra aspiratory tissues than untreated controls did128. Operators focusing on have flagging pathways or receptors may instigate immunopathology. Moreover, the absence of a solid medication conveyance strategy in vivo is especially tricky for siRNAs and different operators that have not been recently utilized in people.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
